ER+/HER2- advanced breast cancer, 2L+ after CDK4/6 inhibitor, ESR1-mutant — Arvinas + Pfizer
Visit Interactive Trial Page →













May 1, 2026 — The FDA approved vepdegestrant (brand: VEPPANU; Arvinas / Pfizer) as monotherapy for adults with ER+/HER2–, ESR1-mutated advanced or metastatic breast cancer who progressed on at least one prior endocrine therapy. This is the first FDA-approved PROTAC (PROteolysis TArgeting Chimera) — a heterobifunctional protein degrader that recruits an E3 ligase to tag and destroy the estrogen receptor.
Why it matters: Vepdegestrant joins elacestrant and imlunestrant as monotherapy options in the ESR1-mutant post–CDK4/6i setting, but is the only mechanism that degrades the receptor rather than antagonizes it. Approval was based on the VERITAC-2 Phase 3 trial.
Notable caveat: ~10% of patients on vepdegestrant develop QT prolongation — flagged on labeling and in early KOL commentary as a real-world consideration.
Threads below are the most active KOL voices reacting to the approval, sourced from X over May 1–4.

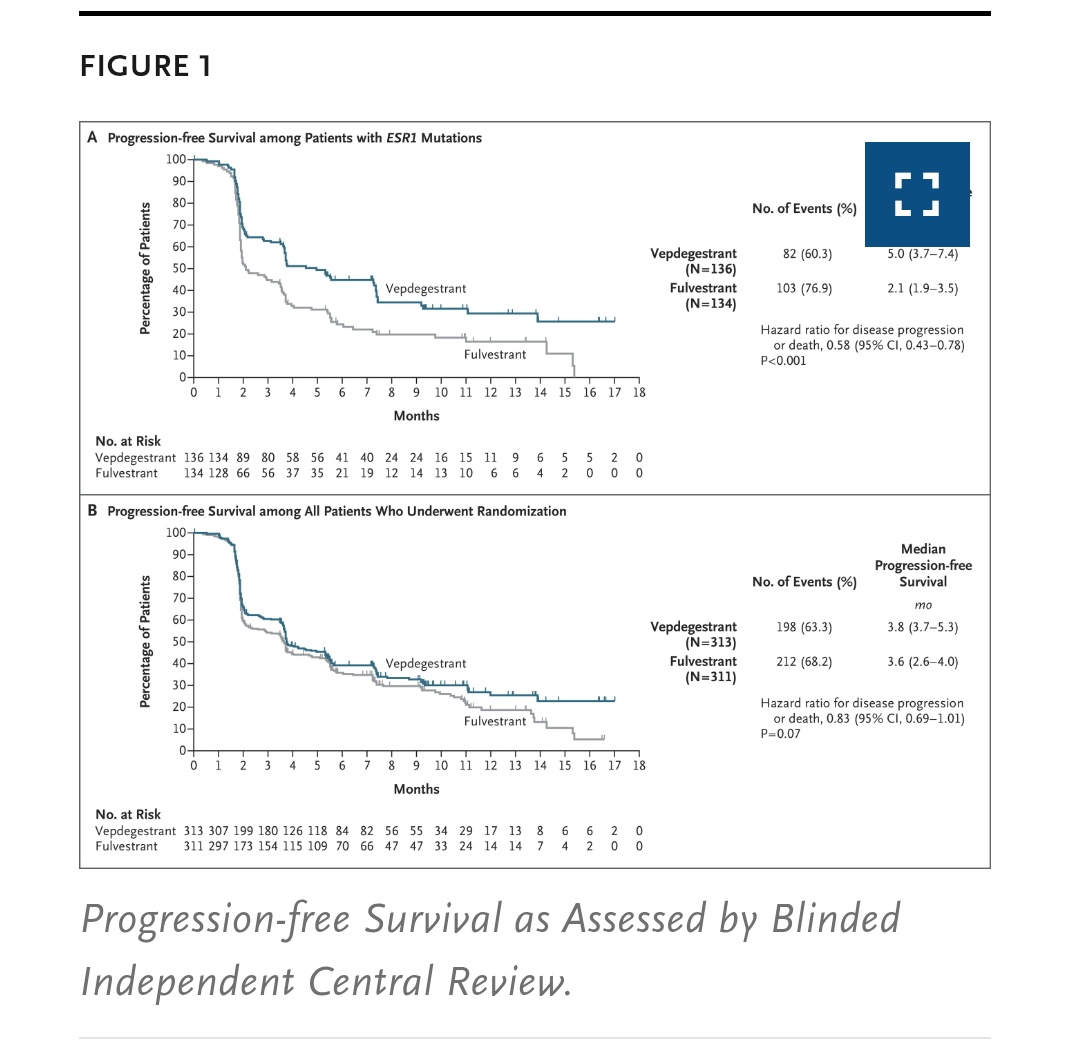
Vepdegestrant (PROTAC ER degrader) @US_FDA ✅ for HR+ metastatic breast based off #Veritac2 Ph III vs. (Fulvestrant) after CDK4/6i + AI: - mPFS 5.0 vs 2.1 mos in ESR1m (HR=0.57) - OS is immature - Well-tolerated, low discontinuation #bcsm @OncUpdates @OncoAlert https://t.co/P4A

FDA Approval in #BreastCancer based on VERITAC-2 https://t.co/S2Y8Aya18n On May 1, 2026, the FDA approved vepdegestrant, a heterobifunctional protein degrader, for ER-positive, HER2-negative, ESR1-mutated advanced breast cancer after progression on endocrine therapy. Approval

Vepdegestrant is now approved for the treatment of patients with ESR1-mutant HR+/HER2- MBC post–≥1 prior ET. It marks the first approval for a PROTAC in oncology — though its approval and efficacy are quite overlapping with oral SERDs. Will you use vepdegestrant in the clinic?
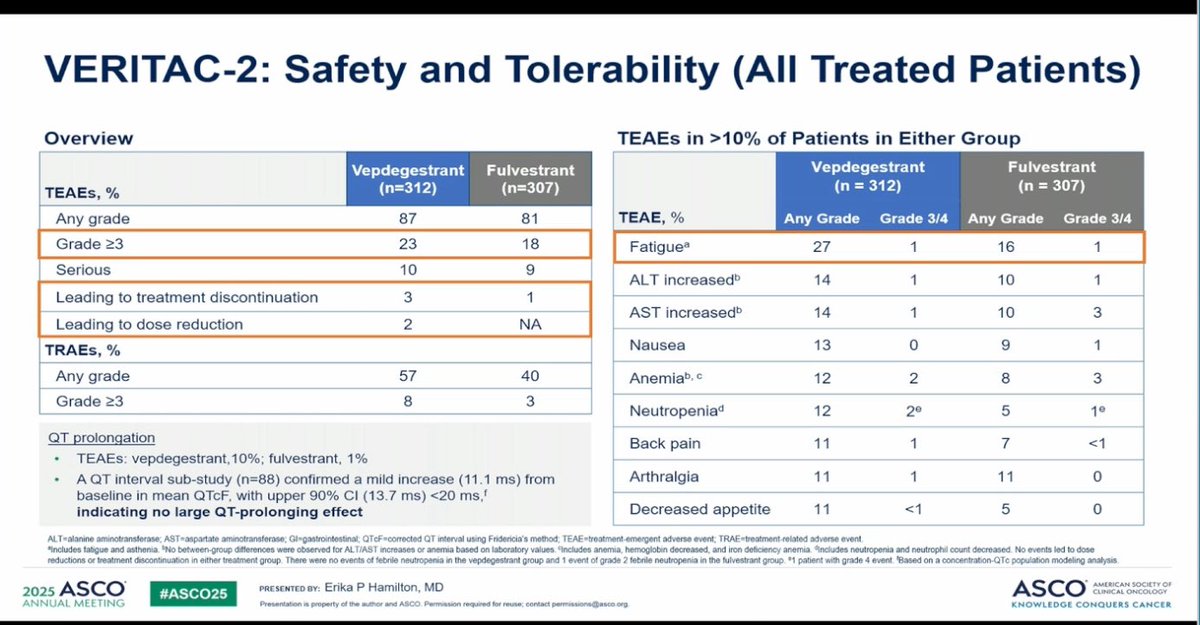
⚠️ Important to remember: 10% of patients on vepdegestrant are expected to develop QT prolongation (1.6% G3) — warranting caution in the coadministration of other QT-prolonging drugs https://t.co/mlJs7Av8fD

FDA approval of vepdegestrant marks a targeted advance in ESR1-mutant HR+/HER2– mBC post CDK4/6. VERITAC-2: improved PFS (5.0 vs 2.1 mo; HR 0.57) vs fulvestrant; OS immature. https://t.co/Lh9qsmfZ6b @OncoAlert @FernandoOnco #BreastCancer #bcsm @FDAOncology @FDA https://t.co/Sm
Mixed polling results on the use of vepdegestrant now that it is FDA approved https://t.co/CgTNfRmYov https://t.co/G8ZfIR9nKm

$ARVN $PFE FDA approves VEPPANU (vepdegestrant) 🎉 → first FDA-approved PROTAC, supporting validation of Arvinas’ protein degradation platform → indicated for ER+/HER2-, ESR1-mutated advanced/metastatic breast cancer after ≥1 endocrine therapy → new commercial product in a https:

@LoiSher this study doesn't prove camizestrant has superior activity over approved degraders (vepdegestrant, imlunestrant). until a h2h trial is done in a standardized population, results only prove the 'early switch' strategy extends pfs. it doesn't establish higher potency in l
Top tweets by impressions — click to view on X
Vepdegestrant demonstrates significant improvement in PFS in 2L in pts with ESR1m HR+ mBC (hazard ratio better than 0.60 targeted in the study). No significant benefit seen in ITT.
First PROTAC…
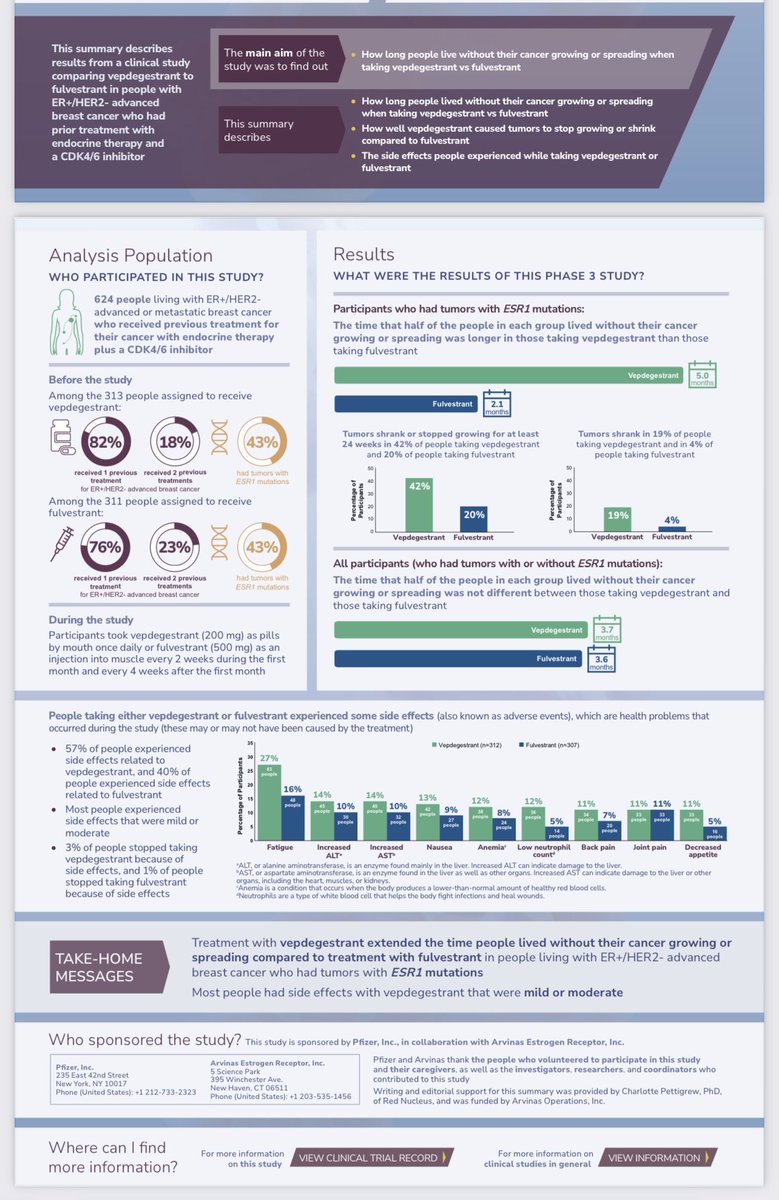
Love @ASCO's patient summaries!
Patients are who we are here for. Communicating findings in lay person wording so everyone can learn is so important!
#VERITAC2 #PROTAC #bcsm #vepdegestrant…
$ARVN & $PFE's vepdegestrant disappoints, and Arvinas shares plunge 40%. My take, via @ApexOnco https://t.co/YanBaOK4pG https://t.co/vXZVjjnDrY
🧬 VERITAC-2 Trial (NEJM May 2025)
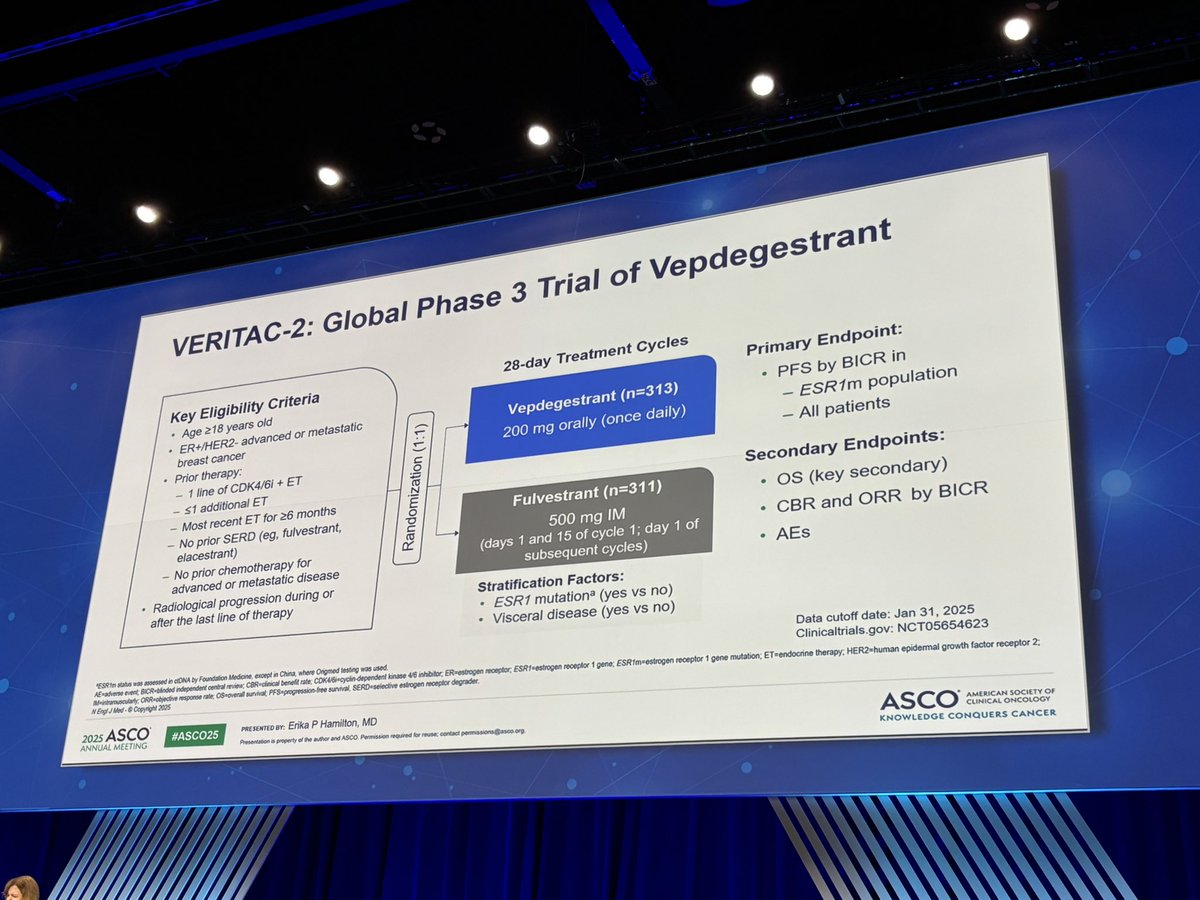
📌 Oral PROTAC ER degrader vepdegestrant vs. fulvestrant in ER+/HER2– MBC post-CDK4/6i
🎯 Primary PFS Results: — ESR1-mut+ ⬆️ PFS:
5.0 vs 2.1 mo
HR 0.58 | p <…
Today at #ASCO25, I’ll be presenting findings from the VERITAC-2 study on vepdegestrant in ER+/HER2- metastatic #breastcancer, the most common subtype, demonstrating a 43% risk reduction in…
Not really surprised to see that vepdegestrant worked in ESR1 mutants, but not in the overall Veritac-2 population $ARVN $PFE https://t.co/L4pzFImdlO
Seeing the Arvinas VERITAC-2 data today reminds me BSB readers recently got the heads up it was unlikely to succeed in allcomers, might have a shot in ESR1 mutant disease… https://t.co/LZS3J4jIRr
Arvinas and Pfizer Announce Positive Topline Results from Phase 3 VERITAC-2 Clinical Trial https://t.co/gpwT1Y6XCS
Join us in Hall B1 this afternoon to hear the details.
What am I particularly excited about?
Of course 5.0 vs. 2.1 months for ESR1m
But...it's the tolerability! Discontinuations and reductions…
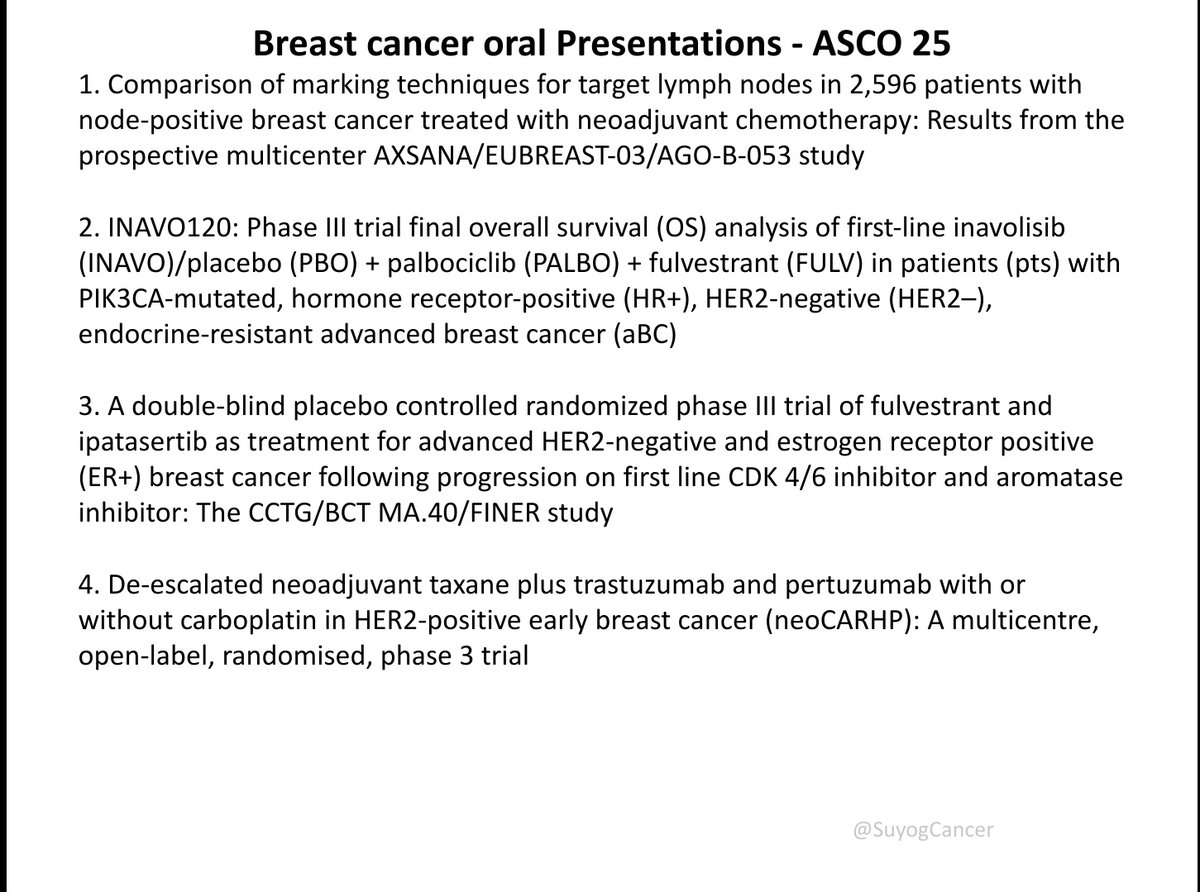
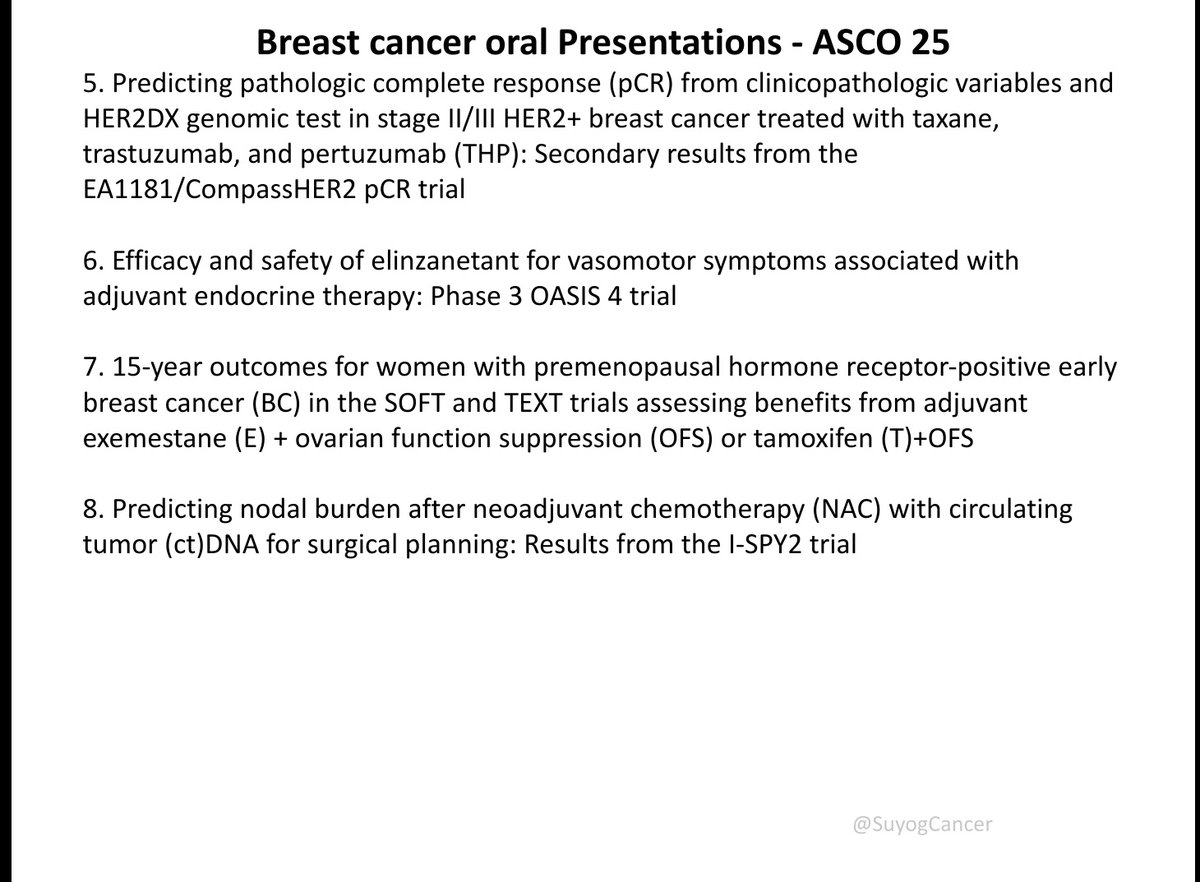
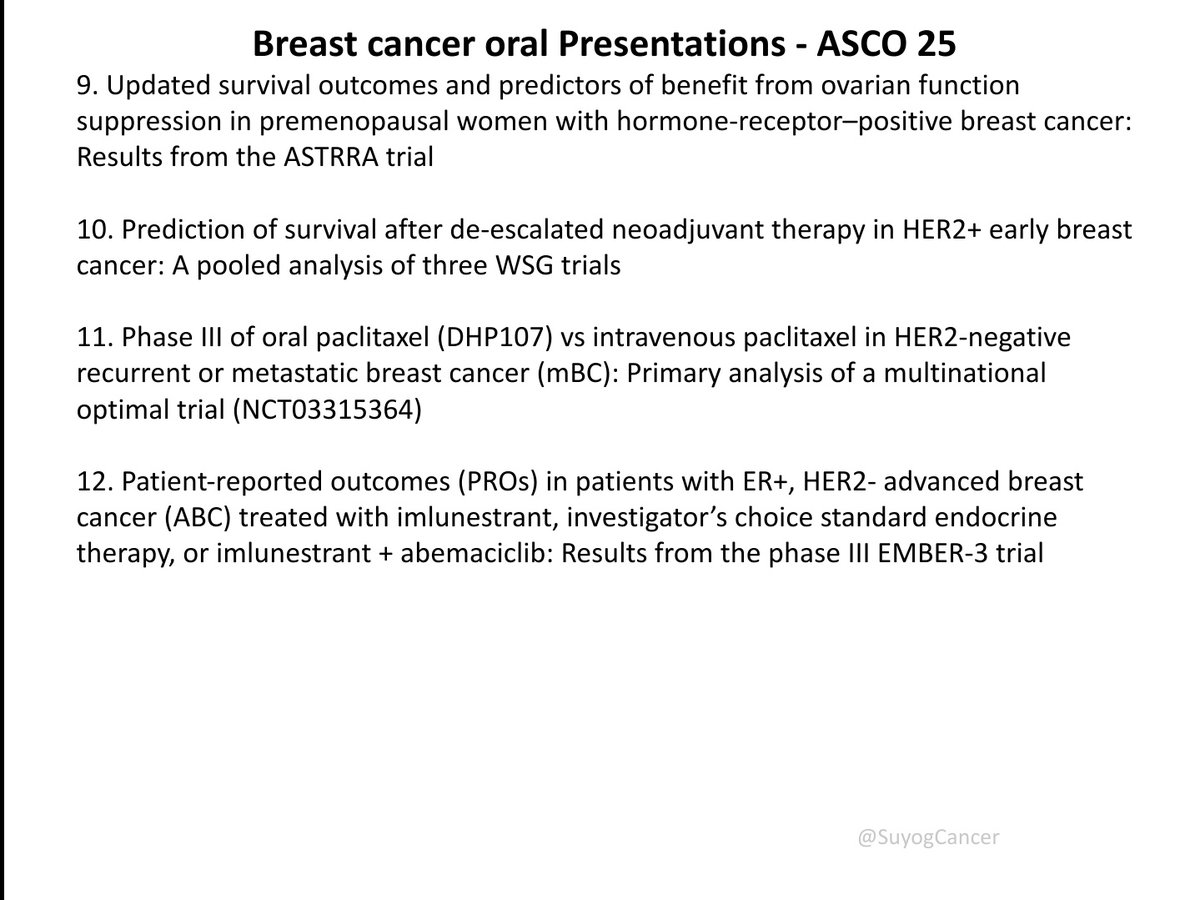
key oral abstracts in breast cancer from #ASCO25
Covering neoadjuvant, adjuvant & metastatic settings: INAVO120, EMBER-3, VERITAC-2, DESTINY-Breast06, AXSANA, I-SPY2 & more! @ASCO @OncoAlert…
VERITAC-2 is the first positive Phase 3 trial of a PROTAC degrader in any cancer. PFS benefit robust in ESR1-mutant subgroup (HR 0.57) but ITT miss (HR 0.83, P=0.07) will shape the approved label. Competes with elacestrant (EMERALD/EMBER-3) for ESR1-mutant 2L ER+ mBC. Oral once-daily with favorable tolerability. OS data maturing.
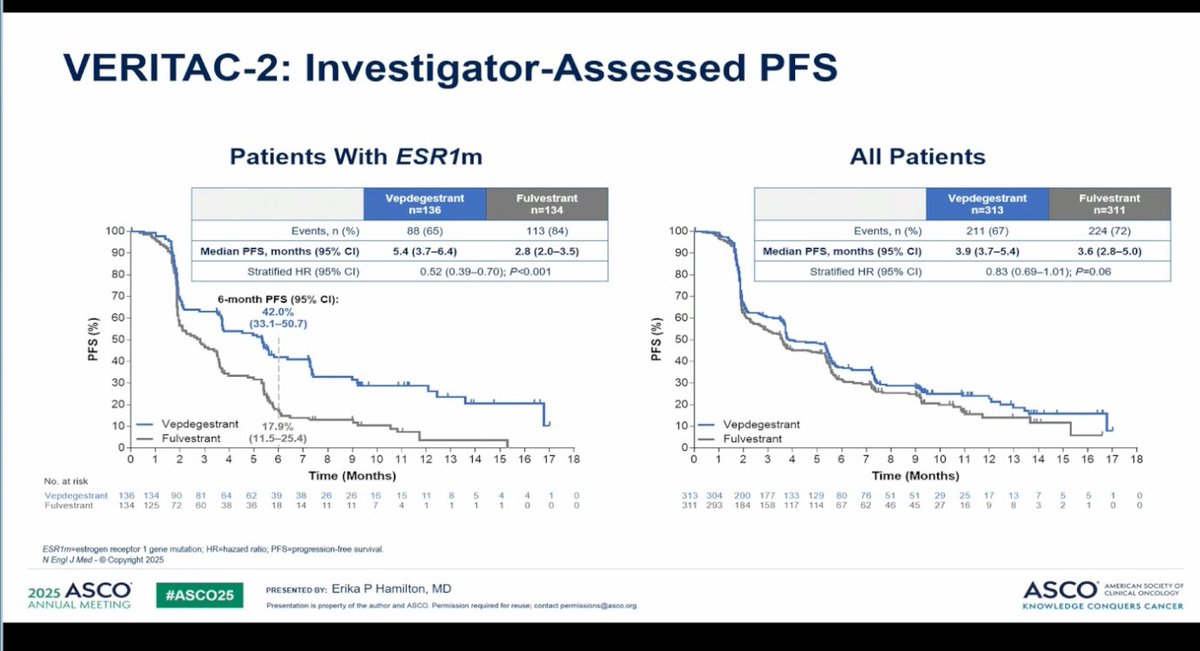
Median: 5.0 months (vepdegestrant, 95% CI 3.7-7.4) vs. 2.1 months (fulvestrant, 95% CI 1.9-3.5). HR 0.57 (95% CI 0.42-0.77), P<0.001 6-month PFS rate: 45.2% (vepdegestrant) vs. 22.7% (fulvestrant). In ESR1-mutant population (n=270, 43% of enrolled), median PFS 5.0 months (95% CI 3.7-7.4) with vepdegestrant vs. 2.1 months (95% CI 1.9-3.5) with fulvestrant; HR 0.57 (95% CI 0.42-0.77, P<0.001) — 43% reduction in risk of progression or death. ORR 18.6% vs. 4.0% (OR 5.45, P=0.001). CBR 42.1% vs. 20.2%. In ITT population, median PFS 3.7 vs. 3.6 months (HR 0.83, 95% CI 0.68-1.02, P=0.07) — did NOT reach statistical significance.
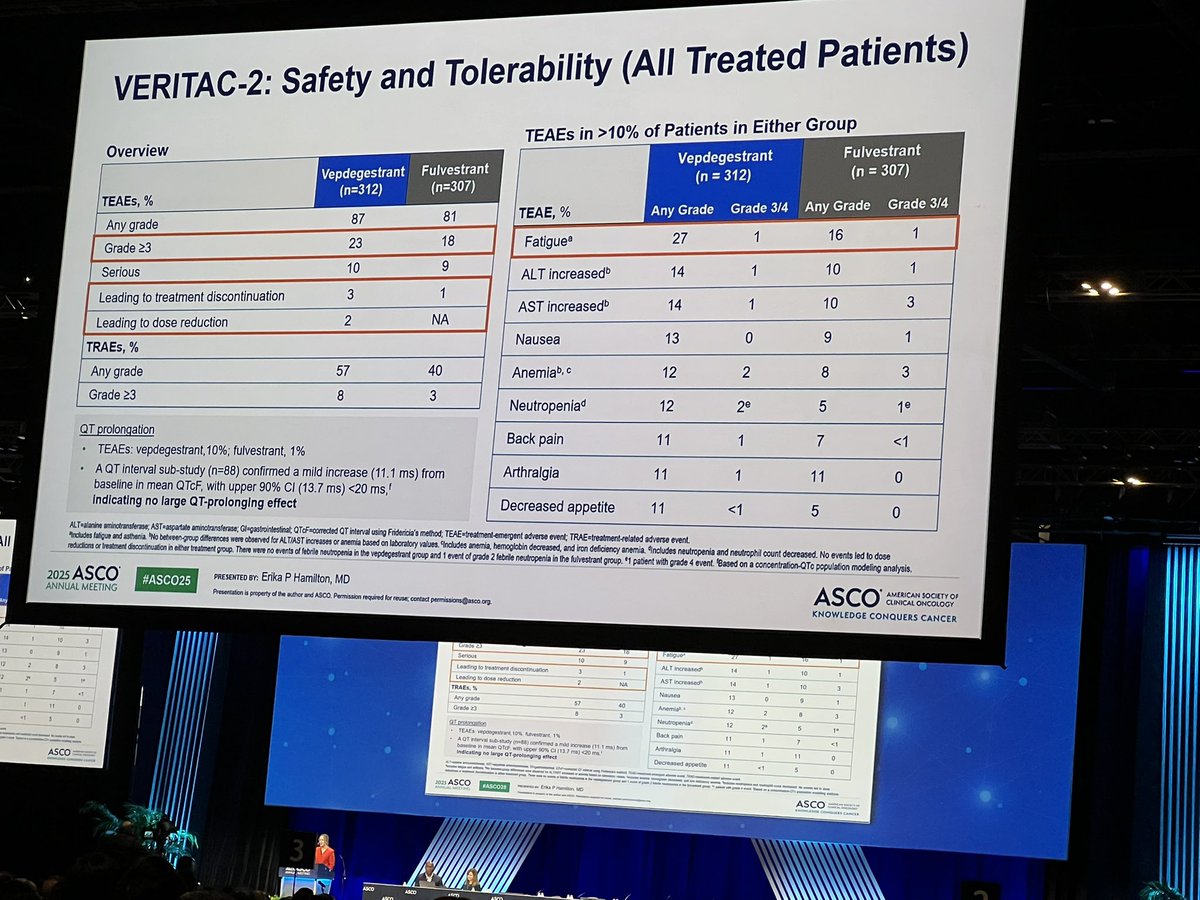
Overall survival (key secondary endpoint) immature at time of primary analysis — less than a quarter of required events had occurred. No treatment-related deaths in either arm.
Grade ≥3 adverse events: 8% (vepde) vs. 3% (fulv). Discontinuation due to AEs: 2.9% (vepde) vs. 0.7% (fulv). Key AEs: fatigue (26.6%), ALT/AST increase (14% each), nausea (13%), anemia (12%). Oral PROTAC degrader generally well tolerated. Grade ≥3 TRAE 8% vs. 3%. Most common TEAEs fatigue, AST/ALT elevation, nausea. GI toxicity rates low (nausea 13.5%, vomiting 6.4%, diarrhea 6.4%). No treatment-related deaths in either arm.
🔄 First PROTAC degrader with Phase 3 positivity; NDA under review (PDUFA June 5, 2026). VERITAC-2 is the first positive Phase 3 trial of a PROTAC degrader in any cancer. PFS benefit robust in ESR1-mutant subgroup (HR 0.57) but ITT miss (HR 0.83, P=0.07) will shape the approved label. Competes with elacestrant (EMERALD/EMBER-3) for ESR1-mutant 2L ER+ mBC. Oral once-daily with favorable tolerability. OS data maturing.




