Newly diagnosed light chain (AL) amyloidosis — Janssen Biotech
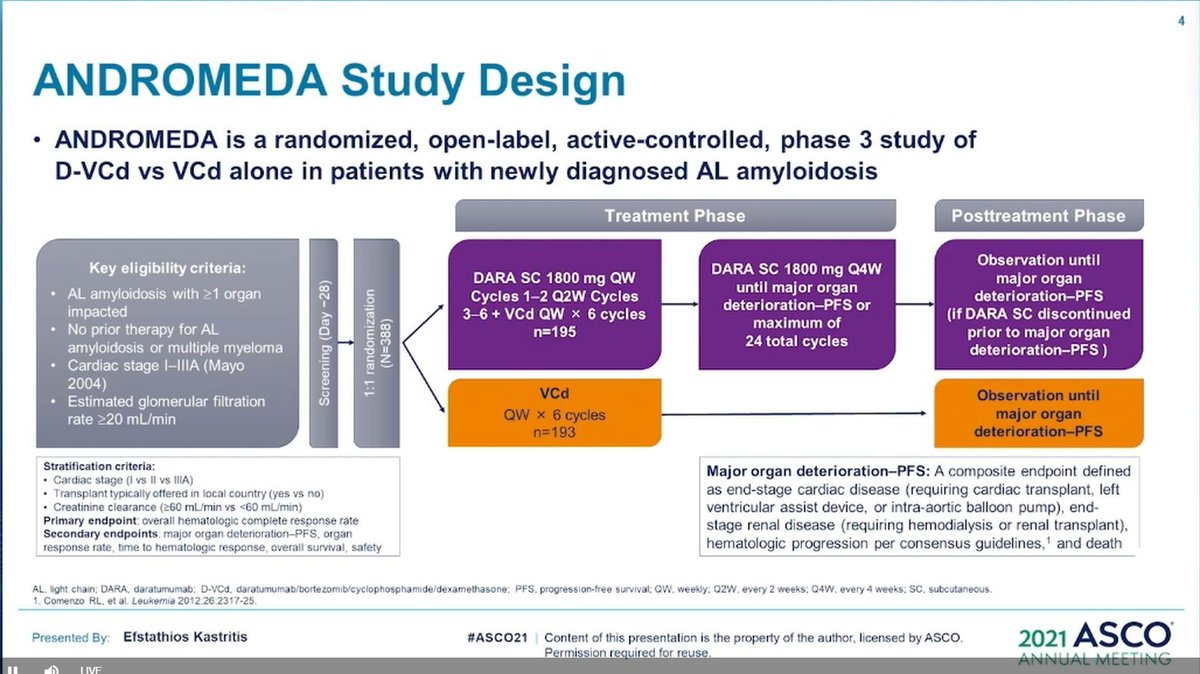
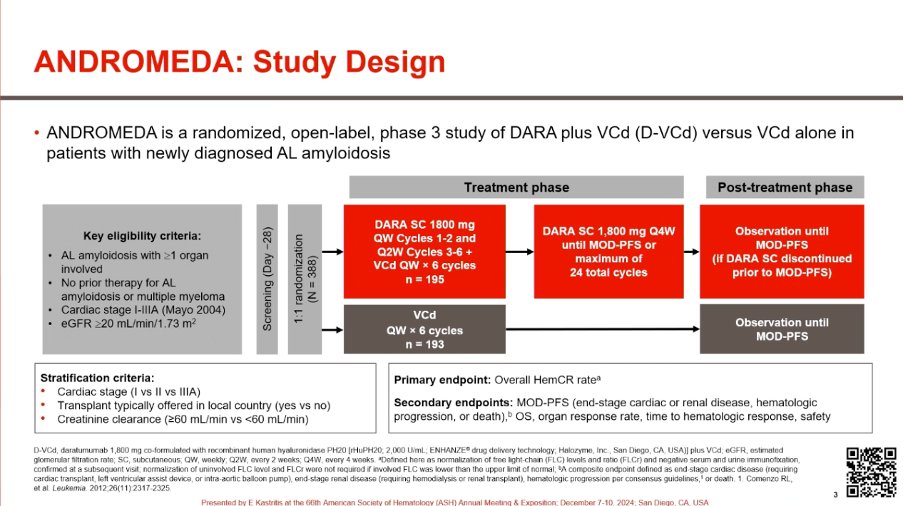
Discover KOL Sentiment on ANDROMEDA →Design - Phase 3 open-label D-VCd vs VCd in newly diagnosed AL amyloidosis, N=388 (NCT03201965).
MOD-PFS (primary) - Median not reached vs 30.2 mo, HR 0.47 (95% CI 0.33-0.67), P<0.0001.
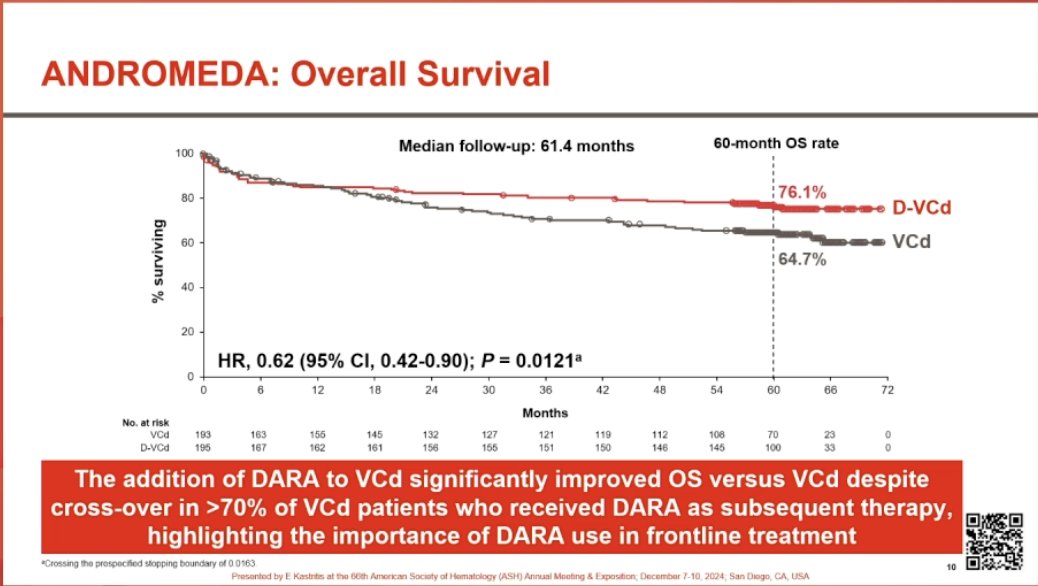
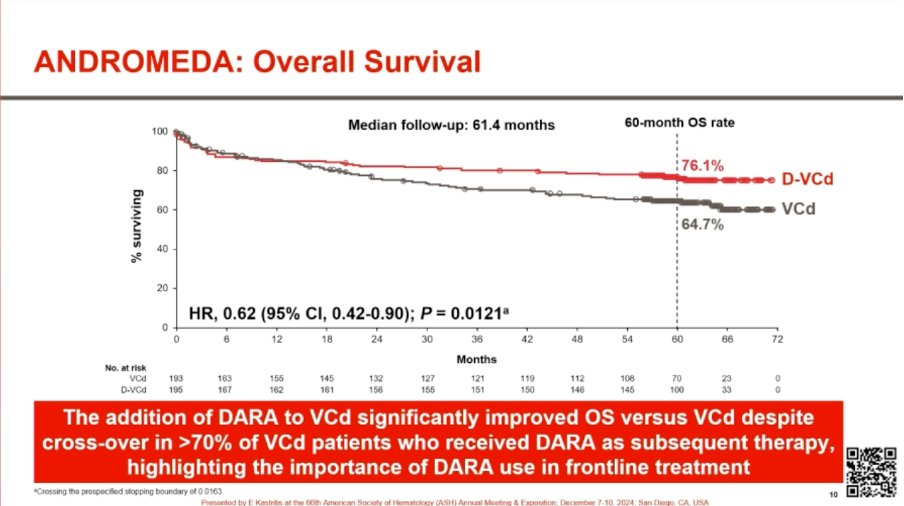
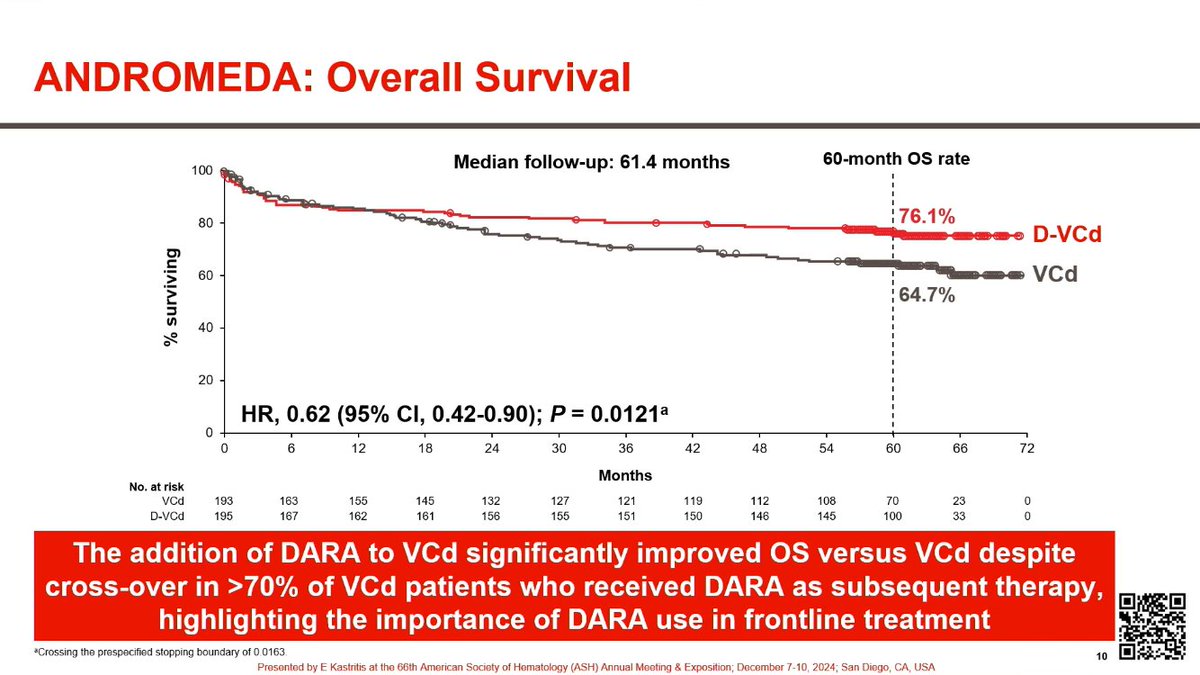
OS - HR 0.62 (95% CI 0.42-0.90), P=0.0121 - a 38% reduction in risk of death; 5-year OS rate 76.1% with D-VCd.
Safety - Grade >=3 lymphopenia 13% and pneumonia 8% in the D-VCd arm; boxed/labeled cardiac-toxicity precaution; not for NYHA IIIB/IV or Mayo Stage IIIB outside trials.
Regulatory - FDA accelerated approval January 15, 2021; traditional approval November 19, 2025 - first approved therapy for newly diagnosed AL amyloidosis.
Sponsor / drug - Janssen Biotech (Johnson & Johnson); daratumumab and hyaluronidase-fihj (Darzalex Faspro) + VCd.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.








Top tweets by impressions — click to view on X
#ASH24 #mmsm
1️⃣ ANDROMEDA overall survival results
➡️ https://t.co/B0Blz7BXwh
✅With 2/3 of pts randomised to VCD receiving subsequent Dara, OS was better with upfront Dara-VCD
✅ Dara-VCD:
- PFS:…
DARZALEX (daratumumab) SC-based regimens improve MRD negativity and PFS in NDMM (CEPHEUS, AURIGA), and OS in AL amyloidosis (ANDROMEDA) #ASH24 $JNJ $GMAB
CEPHEUS: 85% of pts who achieved MRD…
ANDROMEDA trial shows OS benefit in AL Amyloidosis: 5-year OS with Dara-VCd vs VCd-76% vs 64% (HR 0.62; p=0.12).
OS benefit despite ~70% of pts in VCd arm receiving Dara subsequently!
Cardiac CR…
#ASH24 #mmsm @ASH_hematology
Oral amyloidosis: Final update of ANDROMEDA
A great study with OS improvement (despite more than 70% of pts in control arm received Dara based regimen)
This is…
Addition of daratumumab to CVD in newly diagnosed AL amyloidosis improves depth of organ response and overall survival in 5 year follow-up of ANDROMEDA trial #ASH24 @OzAmyloidosis…
#ASH24 @ASH_hematology #mmsm
Challenges encountered with the use of ANDROMEDA trial with unmet needs https://t.co/bzQ7WqRcBI
Andromeda! Reaching the stars with survival data! #ASH24 https://t.co/uWh9Zevgvo
CONGRESS | #ASH24 | Efstathios Kastritis @uoaofficial shares OS, PFS, and organ deterioration data from the ANDROMEDA study of SC dara-VCd in ND AL amyloidosis. For D-VCd and VCd, 60-mo PFS 76.1% and…

For US #HCPs attending #ASH24: don’t miss Dr. Efstathios Kastritis present the final analysis, including overall survival, from the Phase 3 ANDROMEDA study of an anti-CD38 antibody-based regimen in…
ANDROMEDA is the pivotal trial for the first-ever approved therapy for newly diagnosed AL amyloidosis. Daratumumab SC added to VCd significantly improved MOD-PFS (HR 0.47, P<0.0001), OS (HR 0.62, P=0.0121), and doubled cardiac + renal response rates. Accelerated approval 2021 → traditional approval November 19, 2025 on 61.4-mo median follow-up. Cardiac toxicity in stage IIIB/IV patients remains a concern; EMN22 is evaluating dara mono in this high-risk subset (77.5% hemORR). D-VCd is the new global SOC for newly diagnosed AL amyloidosis.
Median: not reached (Dara + VCd (D-VCd)) vs. 30.2 months (VCd alone). HR 0.47 (95% CI 0.33-0.67), P<0.0001 Median follow-up at final analysis rate: 61.4% (months). Phase 3 open-label randomized active-controlled trial, N=388 (D-VCd N=195, VCd N=193). Median follow-up 61.4 months. MOD-PFS (composite: hematologic progression, major organ deterioration, or death) HR 0.47 (95% CI 0.33-0.67, P<0.0001). Median MOD-PFS NOT REACHED with D-VCd vs. 30.2 months with VCd. Primary endpoint met for BOTH accelerated (2021) and traditional (Nov 2025) FDA approvals. Kastritis et al., ANDROMEDA final analysis.
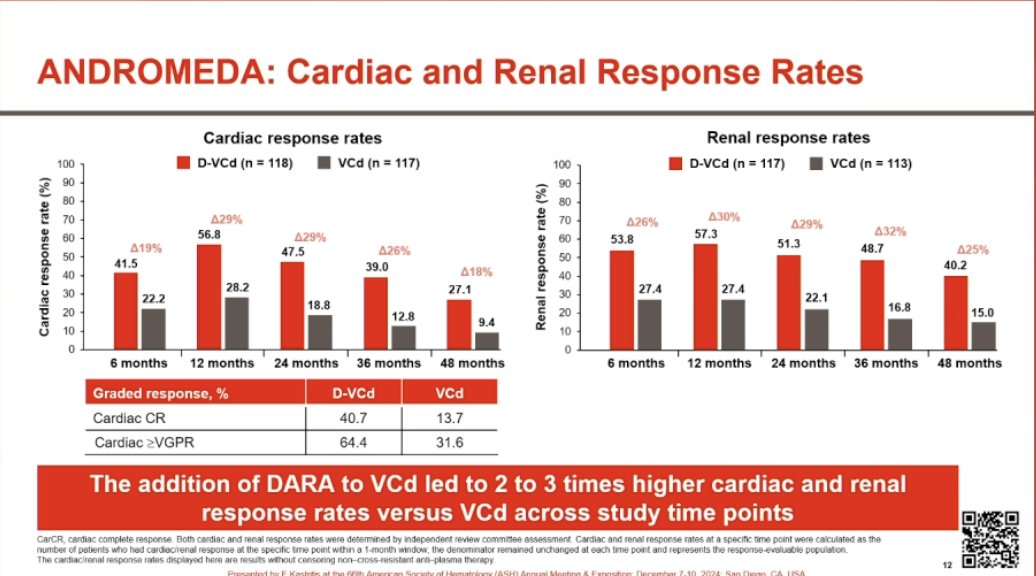
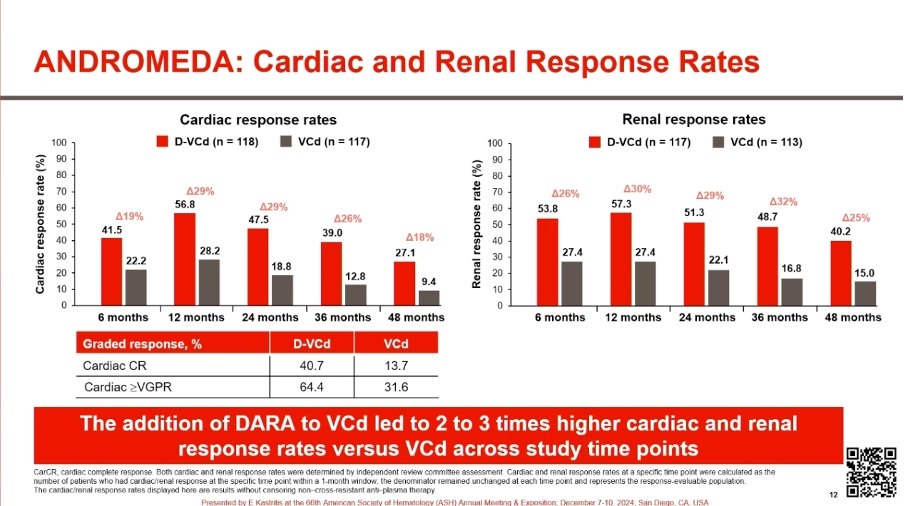
HR 0.62 (95% CI 0.42-0.90), P=0.0121 Final OS analysis: HR 0.62 (95% CI 0.42-0.90, P=0.0121) — 38% reduction in risk of death. Median OS not reached in either arm. 5-year OS rate 76.1% with D-VCd. Complete hematologic response rate at 6 months 50% (D-VCd) vs. 14% (VCd) per primary (HR 6.1, P<0.001). ORR 92% vs. 77%; ≥VGPR 79% vs. 49% (OR 3.8). 6-month cardiac response rate 42% (D-VCd) vs. 22% (VCd) (P=0.0029). 6-month renal response rate 54% vs. 27% (P<0.0001).
Key AEs: Grade ≥3: lymphopenia (13%), pneumonia (8%) - in D-VCd arm. Serious/fatal CARDIAC adverse reactions occurred — Warning and Precaution for cardiac toxicity in prescribing info. NOT indicated for NYHA Class IIIB/IV or Mayo Stage IIIB outside clinical trials. Other boxed concerns: hypersensitivity / administrative reactions, neutropenia, thrombocytopenia, embryo-fetal toxicity, interference with cross-matching / RBC antibody screening. Recommended dose: 1,800 mg daratumumab + 30,000 units hyaluronidase-fihj SC into abdomen per schedule.
✅ FDA traditional approval (Nov 19, 2025): D-VCd is the first approved therapy for newly diagnosed AL amyloidosis. ANDROMEDA is the pivotal trial for the first-ever approved therapy for newly diagnosed AL amyloidosis. Daratumumab SC added to VCd significantly improved MOD-PFS (HR 0.47, P<0.0001), OS (HR 0.62, P=0.0121), and doubled cardiac + renal response rates. Accelerated approval 2021 → traditional approval November 19, 2025 on 61.4-mo median follow-up. Cardiac toxicity in stage IIIB/IV patients remains a concern; EMN22 is evaluating dara mono in this high-risk subset (77.5% hemORR). D-VCd is the new global SOC for newly diagnosed AL amyloidosis.
ANDROMEDA is a Phase 3 open-label, randomized, active-controlled trial (NCT03201965; N=388) of subcutaneous daratumumab added to bortezomib, cyclophosphamide and dexamethasone (D-VCd) versus VCd alone in patients with newly diagnosed light chain (AL) amyloidosis. Major organ deterioration progression-free survival (MOD-PFS) was the primary endpoint.
Adding subcutaneous daratumumab significantly improved major organ deterioration progression-free survival (median not reached vs 30.2 months; HR 0.47; 95% CI 0.33-0.67; P<0.0001) and, at the final analysis, overall survival (HR 0.62; 95% CI 0.42-0.90; P=0.0121) - a 38% reduction in the risk of death, with a 5-year OS rate of 76.1% in the D-VCd arm. Hematologic complete response rates were also higher with D-VCd.
Yes. Daratumumab and hyaluronidase-fihj (Darzalex Faspro) with bortezomib, cyclophosphamide and dexamethasone received FDA accelerated approval on January 15, 2021 for newly diagnosed AL amyloidosis, and the FDA converted it to traditional (regular) approval on November 19, 2025 based on the ANDROMEDA final analysis. It is the first therapy approved for newly diagnosed AL amyloidosis.
Grade 3 or higher lymphopenia (13%) and pneumonia (8%) were among the more common events in the D-VCd arm, and serious or fatal cardiac adverse reactions occurred, prompting a labeled cardiac-toxicity precaution. Darzalex Faspro with VCd is not indicated for patients with NYHA Class IIIB or IV cardiac disease or Mayo Stage IIIB disease outside of controlled clinical trials.
The regimen is for patients with newly diagnosed AL amyloidosis with measurable disease and at least one affected organ. Because of cardiac-toxicity risk, patients with advanced cardiac involvement (NYHA Class IIIB/IV or Mayo Stage IIIB) are excluded from the approved indication outside of clinical trials, and careful cardiac assessment is required.
