Previously treated advanced neuroendocrine tumors (pancreatic and extra-pancreatic NETs) — Alliance for Clinical Trials in Oncology (NCI-funded; Exelixis collaboration with NCI-CTEP)
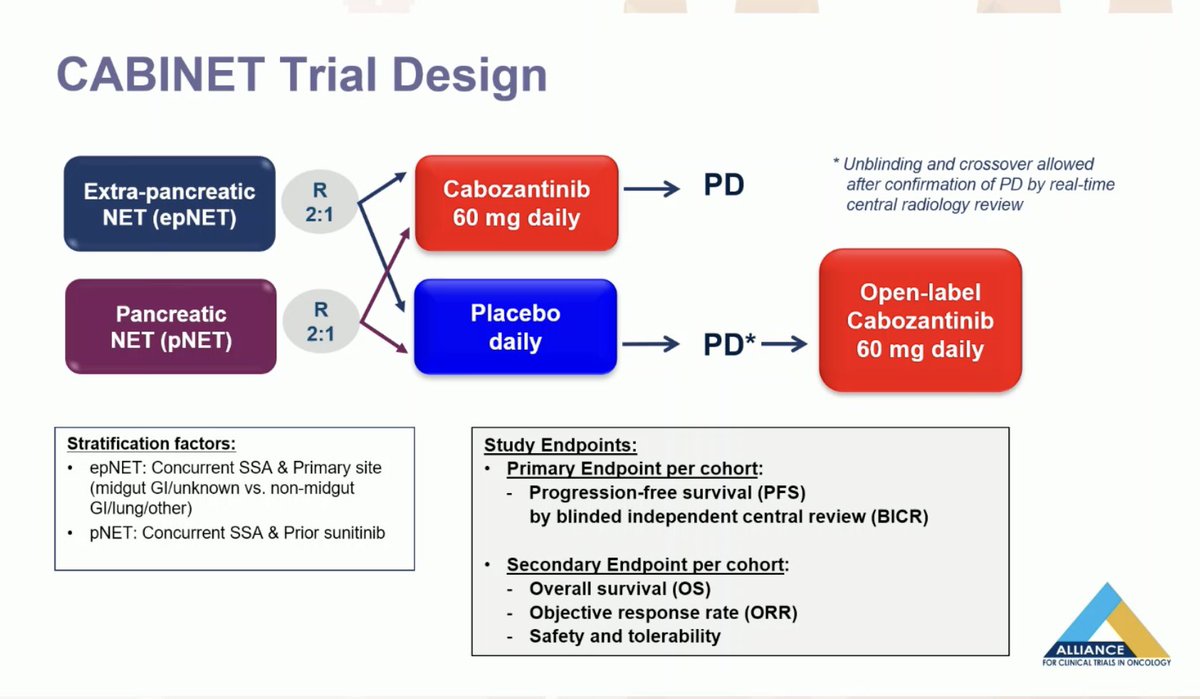
Discover KOL Sentiment on CABINET →Design - Phase 3 randomized, double-blind, placebo-controlled trial of cabozantinib (Cabometyx) vs placebo in previously treated advanced well-differentiated pancreatic (pNET) and extra-pancreatic (epNET) neuroendocrine tumors (NCT03375320; Alliance A021602 / NCI-CTEP).
PFS - pNET cohort (primary) - Median 13.8 vs 3.3 months, HR 0.22 (95% CI ~0.12-0.42), P<0.0001.
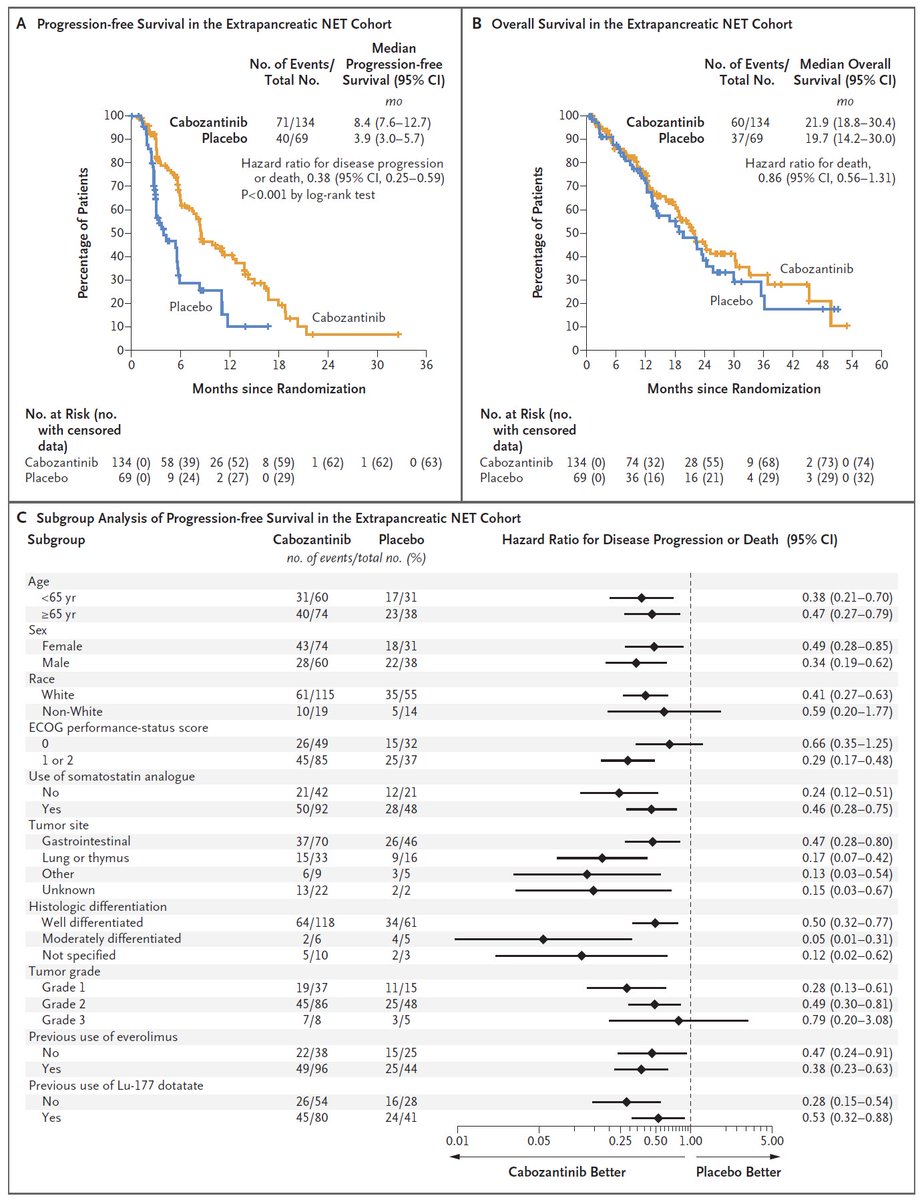
PFS - epNET cohort (primary) - Median 8.5 vs 4.2 months, HR 0.40, P<0.0001.
Overall survival - Immature at interim and confounded by extensive crossover (52% of placebo pNET, 37% of placebo epNET crossed to open-label cabozantinib): HR 1.01 (pNET) and 1.05 (epNET).
Safety - Common adverse events were hypertension, fatigue and diarrhea; profile consistent with prior cabozantinib studies with no new safety signals.
Regulatory / sponsor - FDA approved March 26, 2025 (previously treated advanced pNET + epNET, age >=12). Sponsor Alliance/NCI; cabozantinib (Cabometyx, Exelixis).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.








Top tweets by impressions — click to view on X
💊Cabozantinib for NETs
Full results of CABINET trial @NEJM
➡️Compared to placebo, in previosly treated patients
✅ORR ⬆️
✅PFS⬆️
✅in both pancreatic and extrapancreatic…
Original Article: Phase 3 Trial of Cabozantinib to Treat Advanced Neuroendocrine Tumors (CABINET) https://t.co/VQHcOTKrUV
#ESMO24 | @myESMO https://t.co/Bj4qP0NeC4
#Cabozantinib is now approved in #NET based off #CABINET study! We discussed the design, findings, sequencing, and AEs w/ @AmanChauhanMD
Full 🗣️:
⭐️ https://t.co/AjXESHSbZl
⭐️ Also on the “Oncology…
8/10 CABINET #NET
ph3 cabozantinib vs placebo in pre-treated advanced #Neuroendocrine NETs
@ASCO #ASCO24 @NEJM
📌results presented by BICR for epNET and pNET
➡️ORR by BICR 5% vs 0 in epNET, 19% vs 0…
@OncBrothers @AmanChauhanMD @SylvesterCancer @GlopesMd @NVijayvergiaMD @UGrewalMD @IMG_Oncologists @OncoThor @GrupoGetne @PancPathologist @rcarvalhoonco @T4Cancer The CABINET study’s real-world…
CABINET is the pivotal Phase 3 that established cabozantinib as a new SOC for previously treated advanced well-differentiated pancreatic and extra-pancreatic NETs. Trial stopped early due to efficacy in both cohorts with dramatic PFS improvements (HR 0.22 pNET, HR 0.40 epNET). ORR modest (5-18%) but durable. Adds to limited NET therapeutic armamentarium. Particularly strong signal in lung/thymic NET (ESMO 2025 HR 0.19). NCCN Category 1/2A. Complements STARTER-NET (everolimus + lanreotide in 1L poor-prognosis GEP-NETs, Batch C) in expanding NET treatment options.
Median: 13.8 months (cabozantinib (pNET cohort), 95% CI 8.9-17.0) vs. 3.3 months (placebo (pNET cohort), 95% CI 2.8-5.7) vs. 8.5 months (cabozantinib (epNET cohort), 95% CI 6.8-12.5) vs. 4.2 months (placebo (epNET cohort), 95% CI 3.0-5.7). HR 0.22 (95% CI 0.12-0.41), P<0.0001 pNET cohort rate: 0.22% (HR) vs. 0.12-0.41% (95% CI) vs. <0.0001% (P) vs. 18% (ORR cabo) vs. 0% (ORR placebo). epNET cohort rate: 0.4% (HR) vs. 0.26-0.61% (95% CI) vs. <0.0001% (P) vs. 5% (ORR cabo) vs. 0% (ORR placebo). Lung/thymic NET subgroup (ESMO 2025) rate: 0.19% (HR) vs. 0.06-0.54% (95% CI) vs. 8.2% (mPFS cabo) vs. 2.7% (mPFS placebo). Phase 3 double-blind placebo-controlled trial, N=298 (pNET 99, epNET 199). Randomized 2:1 cabozantinib 60mg daily vs. placebo. STOPPED EARLY for efficacy in both cohorts. pNET: mPFS 13.8 vs. 3.3 months (HR 0.22, 95% CI 0.12-0.41, P<0.0001); ORR 18% vs. 0%. epNET: mPFS 8.5 vs. 4.2 months (HR 0.40, 95% CI 0.26-0.61, P<0.0001); ORR 5% vs. 0%. Lung/thymic NET subgroup (ESMO 2025): HR 0.19 stratified, mPFS 8.2 vs. 2.7 months. Study chair: Jennifer Chan, MD, MPH (Dana-Farber). NEJM 2024 publication.
HR 1.01 (95% CI 0.55-1.83) OS immature at interim. pNET: 32 deaths cabo / 17 deaths placebo, HR 1.01 (95% CI 0.55-1.83). epNET: 83 deaths cabo / 40 deaths placebo, HR 1.05 (95% CI 0.71-1.54). 52% of placebo pNET patients crossed over to open-label cabozantinib (37% in epNET), potentially confounding OS evaluation.
Key AEs: hypertension, fatigue, diarrhea. Safety profile consistent with prior cabozantinib studies. No new safety signals. NCCN Guidelines (January 2025) updated to include cabozantinib as category 1 or 2A preferred regimen for certain well-differentiated NETs.
✅ FDA-approved (March 26, 2025): First new SOC for previously treated NETs in >5 years. CABINET is the pivotal Phase 3 that established cabozantinib as a new SOC for previously treated advanced well-differentiated pancreatic and extra-pancreatic NETs. Trial stopped early due to efficacy in both cohorts with dramatic PFS improvements (HR 0.22 pNET, HR 0.40 epNET). ORR modest (5-18%) but durable. Adds to limited NET therapeutic armamentarium. Particularly strong signal in lung/thymic NET (ESMO 2025 HR 0.19). NCCN Category 1/2A. Complements STARTER-NET (everolimus + lanreotide in 1L poor-prognosis GEP-NETs, Batch C) in expanding NET treatment options.
CABINET (Alliance A021602, NCT03375320) is a Phase 3, randomized, double-blind, placebo-controlled trial run by the Alliance for Clinical Trials in Oncology and the NCI that tested cabozantinib (Cabometyx) versus placebo in patients with previously treated advanced well-differentiated pancreatic and extra-pancreatic neuroendocrine tumors. Progression-free survival was the primary endpoint in each cohort.
Cabozantinib significantly prolonged progression-free survival in both cohorts: median 13.8 versus 3.3 months in the pancreatic NET cohort (hazard ratio 0.22, P<0.0001) and 8.5 versus 4.2 months in the extra-pancreatic NET cohort (hazard ratio 0.40, P<0.0001). The trial was stopped early for efficacy. Overall survival was immature and confounded by extensive crossover from placebo to open-label cabozantinib.
Yes. On March 26, 2025 the FDA approved cabozantinib (Cabometyx) for adults and children 12 years and older with previously treated, unresectable, locally advanced or metastatic well-differentiated pancreatic and extra-pancreatic neuroendocrine tumors. It is the first systemic therapy approved for previously treated NET regardless of primary tumor site, grade, somatostatin-receptor expression, or functional status.
The most common adverse events in CABINET were hypertension, fatigue and diarrhea, consistent with cabozantinib's established safety profile with no new safety signals. As with other multikinase inhibitors, monitoring for hypertension and dose modification for tolerability are part of routine management.
CABINET is the pivotal Phase 3 trial that established cabozantinib as a new standard of care for previously treated advanced neuroendocrine tumors - the first new systemic option for this setting in more than five years. NCCN guidelines (January 2025) were updated to include cabozantinib as a preferred regimen for certain well-differentiated NETs.