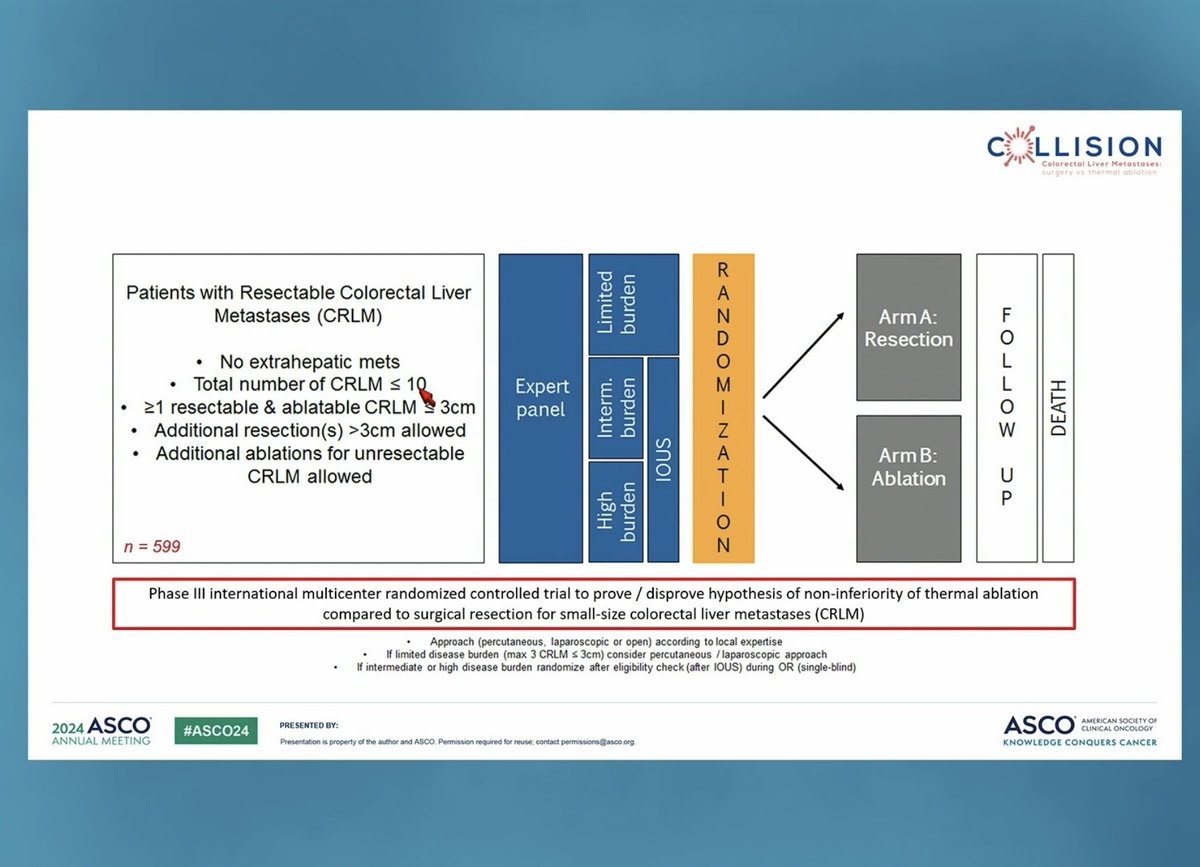
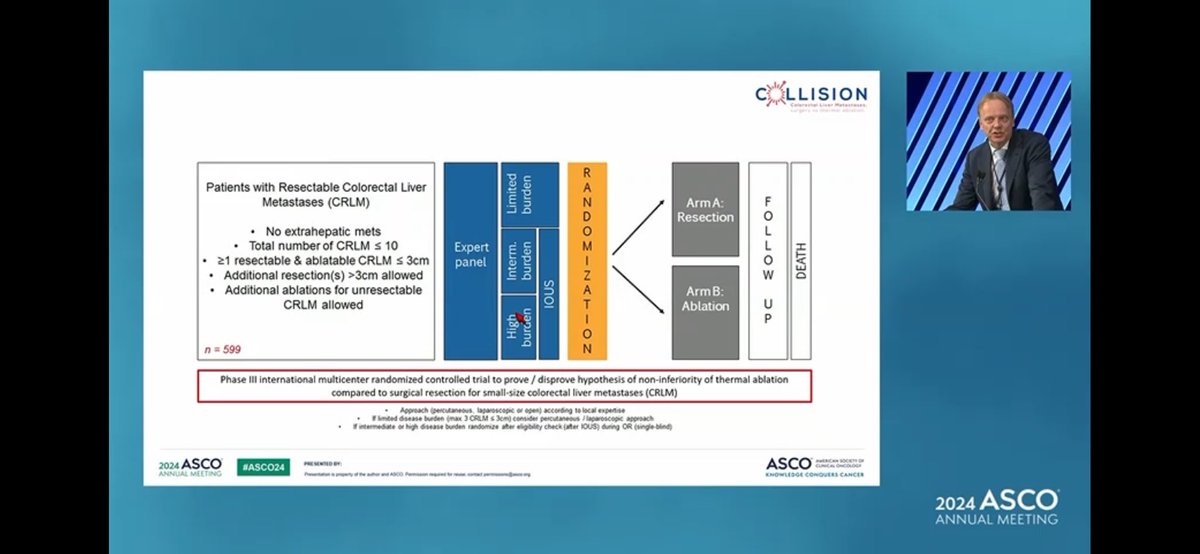
Resectable colorectal liver metastases ≤3 cm (up to 10 CRLM, no extrahepatic disease) — Amsterdam UMC (VUmc) / Dutch Colorectal Cancer Group; funded by Medtronic-Covidien Investigator-Sponsored Research grant
Discover KOL Sentiment on COLLISION →Design - Phase 3 non-inferiority: thermal ablation (RFA/MWA) vs surgical resection, resectable colorectal liver metastases <=3 cm (NCT03088150); 299 randomized (147 ablation, 148 resection); primary OS non-inferiority.
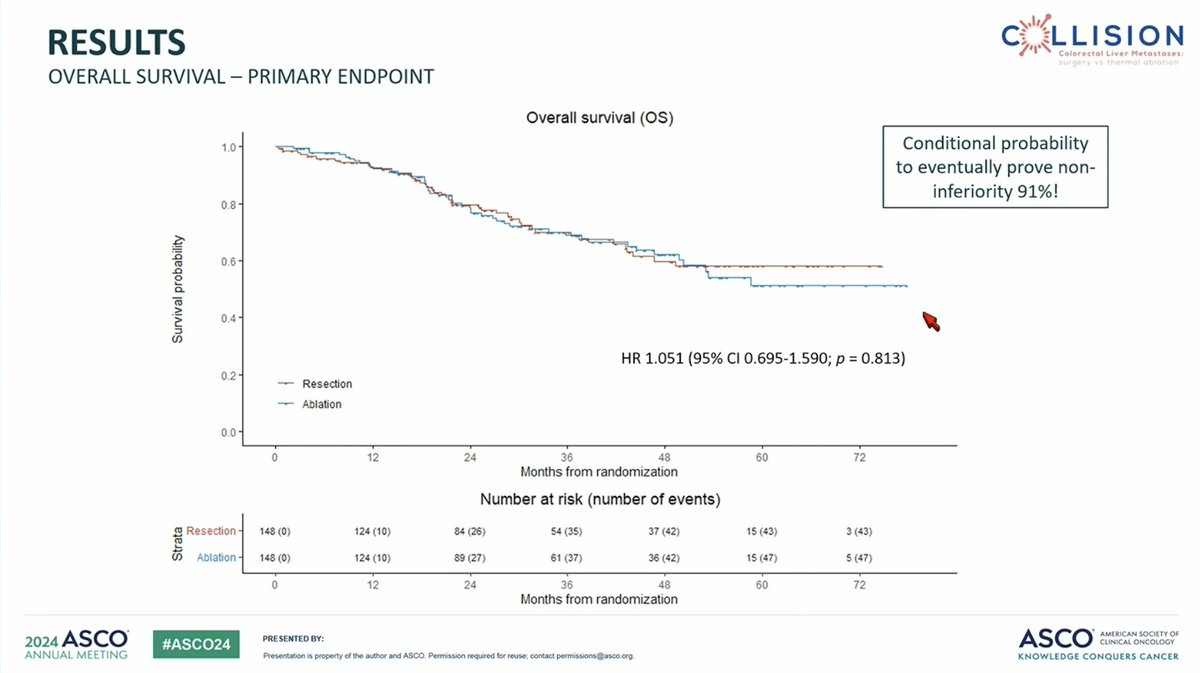
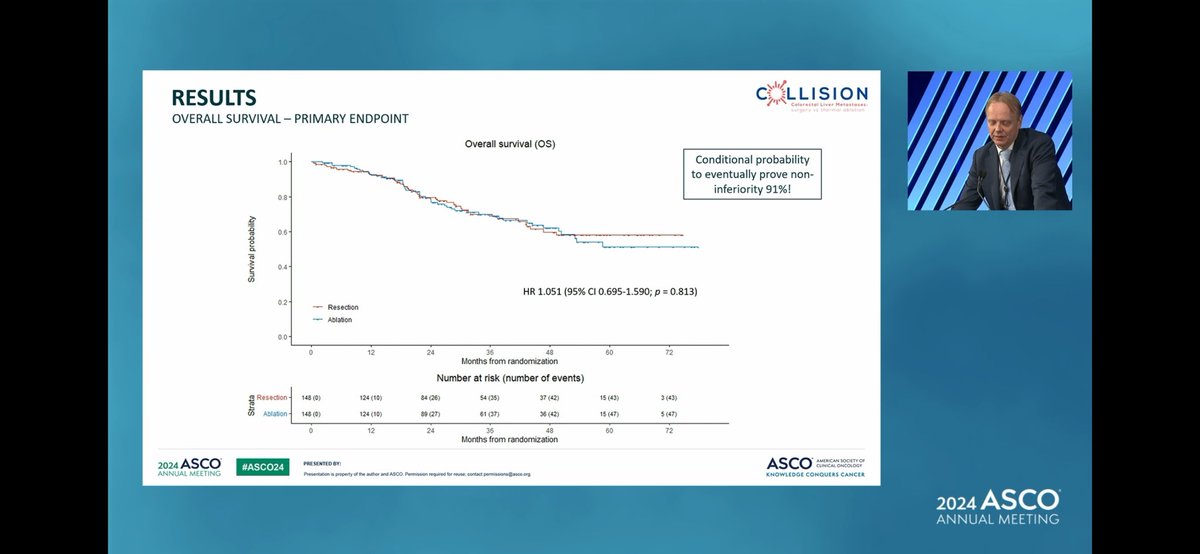
OS (primary, non-inferiority MET) - Medians not reached; HR 1.042 (95% CI 0.689-1.576), P=0.846 - ablation non-inferior to surgery.
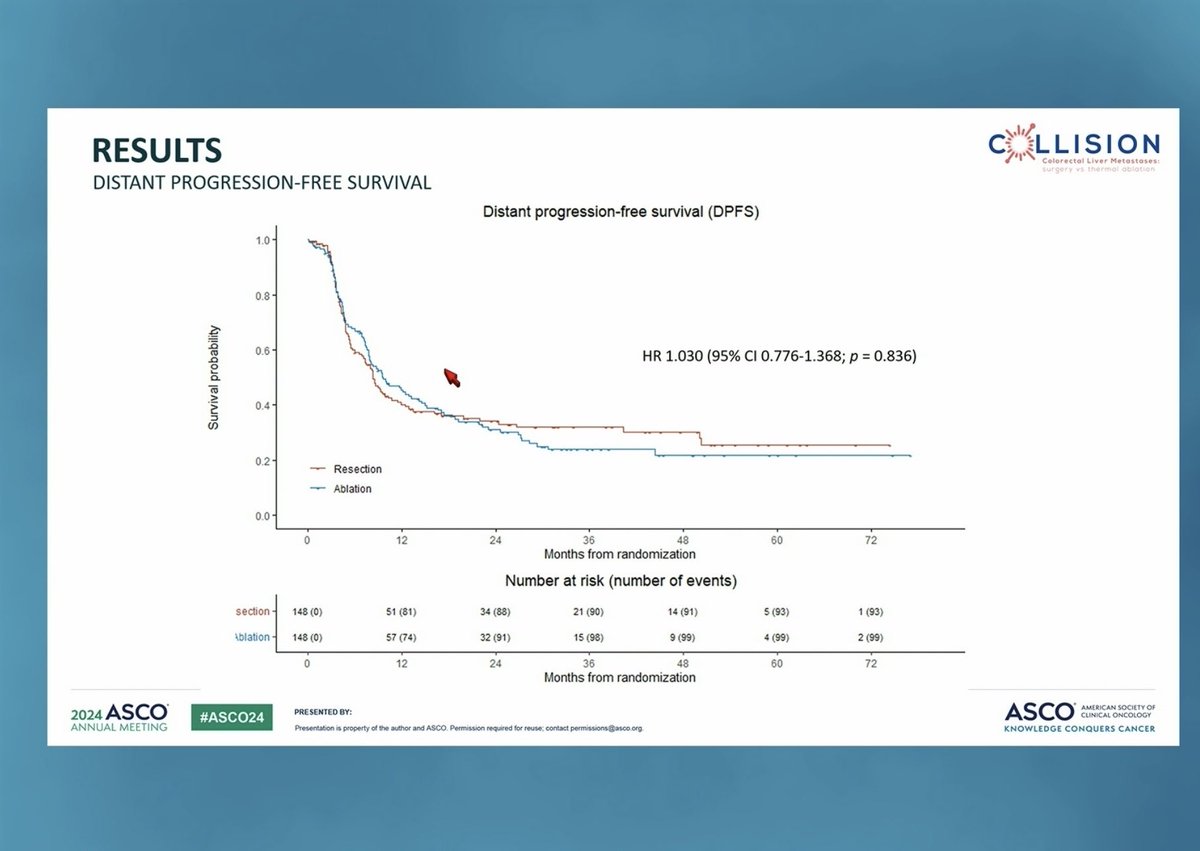
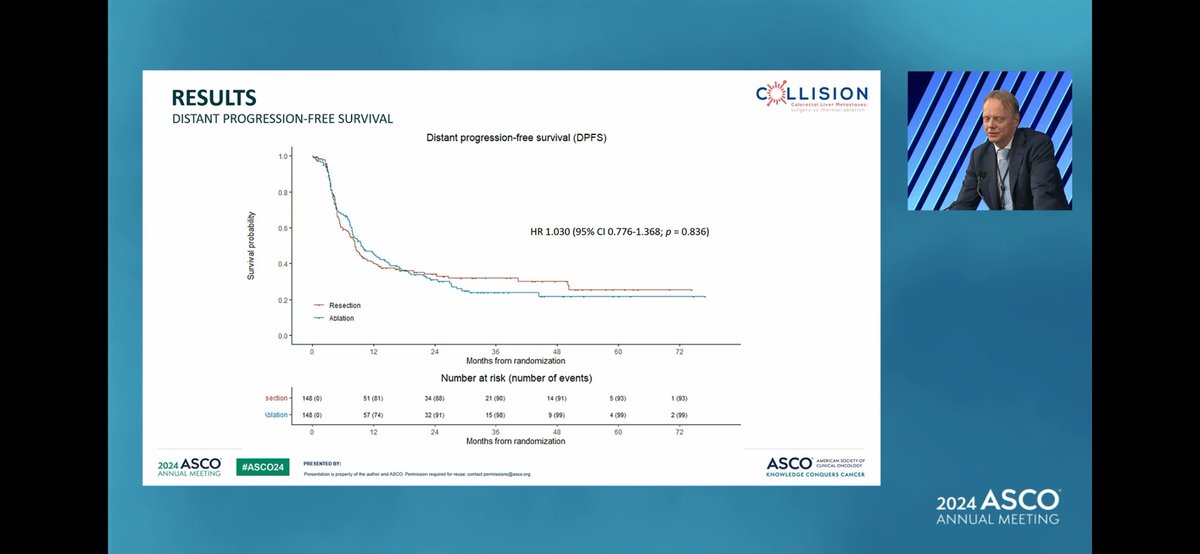
Local control - Favored ablation - HR 0.184 (95% CI 0.040-0.838), P=0.029; no difference in local or distant PFS.
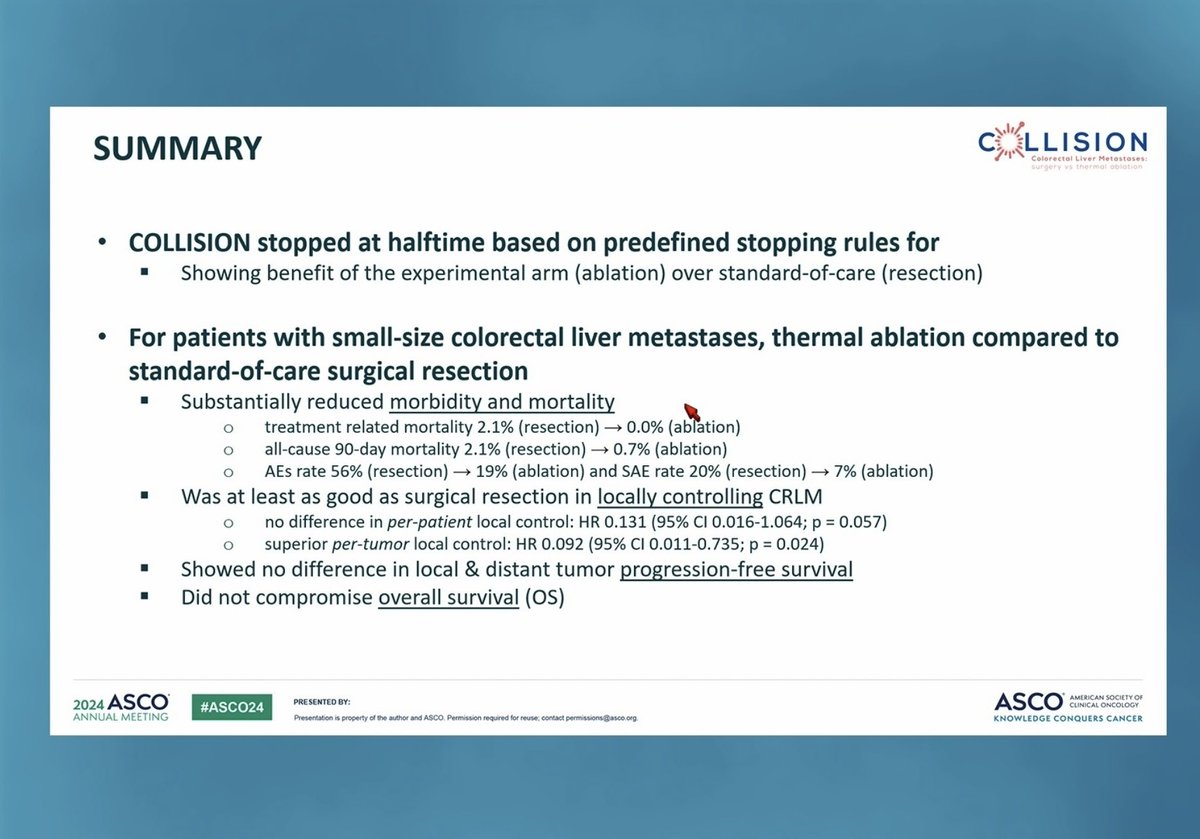
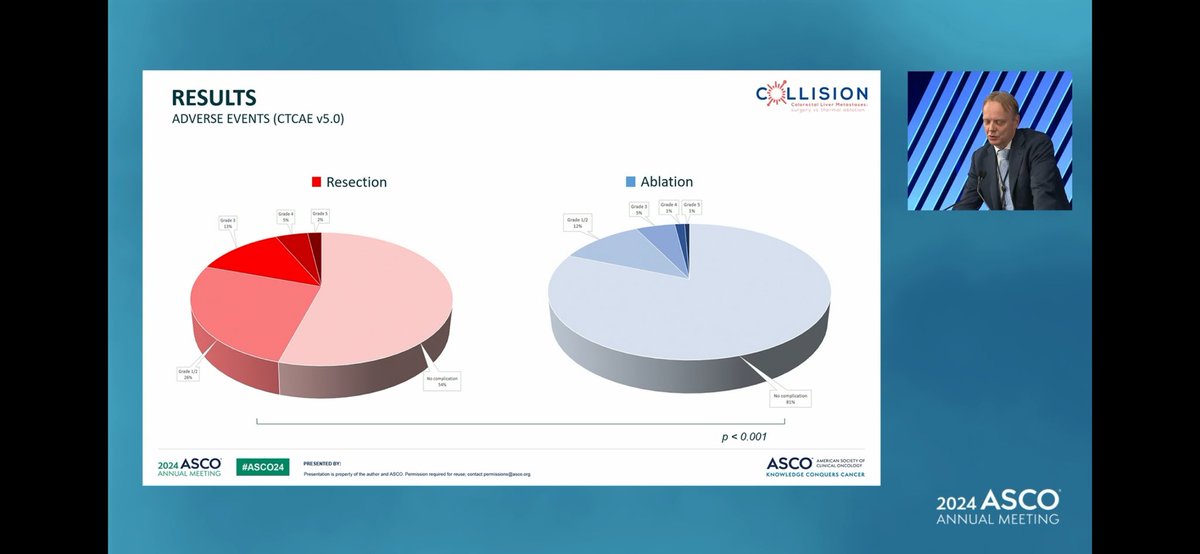
Safety - Procedure-related mortality 0% (0/147 ablation) vs 2.1% (3/148 resection); serious AEs 7.4% vs 19.9%; hospital stay median 1 day vs longer.
Regulatory - Not a drug trial - no FDA drug approval; practice-changing evidence that ablation is a standard option for small CRLM.
Sponsor - Amsterdam UMC (VUmc) / Dutch Colorectal Cancer Group; Medtronic-Covidien investigator-sponsored research grant.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.












Top tweets by impressions — click to view on X
Surgery vs ablation for small-size CRC liver mtes at #ASCO24
🔎COLLISION phase III, 300 pts
👉medien size 14mm, 2mets
👉mOS: no difference
👉similar local control
👉reduced morbidity & mortality in…
#ASCO24 @OncoAlert
No difference seen in ablation 🆚 surgery for small sized liver metastases from #colorectalcancer.
Even though it’s reserved as a backup to surgery, trial had to be stopped half…
With a truly commendable methodology the Dutch COLLISION trial shows non-inferiority of thermal ablation to resection for small (<3cm) colorectal cancer liver metastases #ASCO24 #crcsm…
Is RFA as good as resection for small colorectal metastases? Results of the Collision Study presented at @ASCO #ASCO24
@kharofaJ @shimulshah73 @FlavioRochaMD @drymtn @HopSTranCao …
Great recap of key GI studies from #ASCO24!
Adding to the COLLISION debate, here's an insightful multi-disciplinary look at liver metastases management.
COLLISION hints that patients 'favorable…
🚨COLLISION🚨
RCT Pts with <= 10 resectable CRC liver-only metastases measuring <=3 cm in size
*resection allowed for tumors > 3 cm
Randomized
Surgical Resection
Vs
Percutaneous thermal…

Is thermal ablation 🔥 equivalent to
resection🔪for <3cm, well-located #CRLM
Results of the 🇳🇱 COLLISION suggests so
@ASCO #ASCO24 @OncoAlert
@OHSUsurgery @OHSUKnight @dotter_IR…

Live from #ASCO24 #CRC Track ❤️🔥❤️🔥
COLLISION Study by Martijn Ruben Meijerink
☑️Surgery vs Thermal Ablation for Small-Size CRC Liver Mets
☑️Over 600 patients with ≤3 cm liver mets/Maximum of ten…

Dr. Meijerink PhIII COLLISION trial <10 #CRLMs 1:1 resection vs ablation ➡️ similar OS, not diff in local and distant recurrence
Both arms got 20-23% chemo, mean tumor size < 20 mm, low tumor…

@GIMedOnc I would be very careful with COLLISION- they have a ridiculous NI margin, allowed crossover, and counted local control differently for TA than surgery. I posted a 🧵 on this a while…
COLLISION is the first Phase 3 non-inferiority RCT directly comparing thermal ablation vs. surgical resection in resectable small CRLM. Ablation was NON-INFERIOR on OS while offering lower procedural mortality (0% vs. 2.1%), lower AE burden, shorter hospital stay, and — unexpectedly — BETTER local control (HR 0.184). Stopped early at halftime for meeting stopping rules. Challenges the long-held assumption that resection is the default for small CRLM when both modalities are feasible. COLLISION XL (3-5cm CRLM, thermal ablation vs. SBRT) and COLLISION RELAPSE are ongoing.
Median: not reached (thermal ablation (RFA/MWA)) vs. not reached (surgical resection). HR 1.042 (95% CI 0.689-1.576), P=0.846 Phase 3 non-inferiority trial enrolled 341 patients (299 randomized: 147 ablation, 148 resection; 4 excluded post-randomization). At median follow-up 28.8 months, no OS difference: HR 1.042 (95% CI 0.689-1.576, P=0.846) — conditional probability >90% to prove non-inferiority. Trial stopped early (halftime) for meeting predefined halting criteria / early benefit. Published Lancet Oncology 2025;26(2):187-199.
HR 1.042 (95% CI 0.689-1.576), P=0.846 Primary OS met non-inferiority (see above). Local control FAVORED thermal ablation: HR 0.184 (95% CI 0.040-0.838, P=0.029). No differences in local PFS (HR 0.833, P=0.528) or distant PFS (HR 0.982, P=0.898). Practice-changing finding: local control comparable/better with ablation.
Strong safety and logistics advantage for thermal ablation: Procedure-related mortality 0% (0/147 ablation) vs. 2.1% (3/148 resection). Serious adverse events 7.4% vs. 19.9%. Total AEs significantly favored ablation (P<0.001). Hospital stay: median 1 day (range 1-44) ablation vs. 4 days (1-36) surgery, P<0.001. Bleeding requiring intervention: 1% vs. 5.5%. Infections requiring treatment: 4% vs. 7.5%.
✅ Practice-changing: thermal ablation is non-inferior to surgery for CRLM ≤3 cm with better safety, shorter stay, and improved local control. COLLISION is the first Phase 3 non-inferiority RCT directly comparing thermal ablation vs. surgical resection in resectable small CRLM. Ablation was NON-INFERIOR on OS while offering lower procedural mortality (0% vs. 2.1%), lower AE burden, shorter hospital stay, and — unexpectedly — BETTER local control (HR 0.184). Stopped early at halftime for meeting stopping rules. Challenges the long-held assumption that resection is the default for small CRLM when both modalities are feasible. COLLISION XL (3-5cm CRLM, thermal ablation vs. SBRT) and COLLISION RELAPSE are ongoing.
COLLISION is a Phase 3 randomized non-inferiority trial (NCT03088150) comparing image-guided thermal ablation (radiofrequency or microwave ablation) with surgical resection for patients with resectable small (<=3 cm) colorectal liver metastases (up to 10 lesions and no extrahepatic disease). It was run by Amsterdam UMC and the Dutch Colorectal Cancer Group.
Thermal ablation was non-inferior to surgical resection for overall survival: medians were not reached in either arm, with a hazard ratio of 1.042 (95% CI 0.689-1.576; P=0.846). Local control actually favored ablation (HR 0.184; 95% CI 0.040-0.838; P=0.029), with no differences in local or distant progression-free survival.
COLLISION provides the first Phase 3 randomized evidence that, for small (<=3 cm) resectable colorectal liver metastases, thermal ablation is non-inferior to surgery with better safety and comparable-to-better local control - supporting ablation as a standard option in this setting. There is no drug and no FDA drug approval involved; this is a surgical/interventional treatment decision.
Ablation had a strong safety and logistics advantage: procedure-related mortality was 0% (0/147) with ablation versus 2.1% (3/148) with resection, serious adverse events were 7.4% versus 19.9%, total adverse events significantly favored ablation, and median hospital stay was 1 day with ablation versus a longer stay with surgery.
COLLISION applies to patients with resectable colorectal liver metastases that are small (<=3 cm), up to 10 in number, with no extrahepatic disease. The findings should not be extrapolated to larger metastases or patients with extrahepatic disease, where resection or other strategies may be preferred.