ER+/HER2- advanced or metastatic breast cancer with ESR1 mutation, after prior ET + CDK4/6 inhibitor — Menarini / Stemline Therapeutics (Radius Health co-developer)
Discover KOL Sentiment on EMERALD →Design - Phase 3 elacestrant (oral SERD) vs standard-of-care endocrine therapy (fulvestrant or AI), ER+/HER2- advanced/mBC after prior ET + CDK4/6i (NCT03778931).
PFS - ITT - Median 3.8 vs 1.9 mo, HR 0.55 (95% CI 0.39-0.77), P=0.0005.
PFS - ESR1-mutated, >=12 mo prior ET+CDK4/6i - Median 8.6 vs 1.9 mo - the enriched, most-benefiting subgroup.
OS - Immature at primary analysis and subsequent updates; approval was based on the PFS benefit in the ESR1-mutated population.
Regulatory - FDA approved January 27, 2023 - first oral SERD for ESR1-mutated ER+/HER2- advanced breast cancer (companion diagnostic Guardant360 CDx).
Sponsor / drug - Menarini / Stemline Therapeutics; elacestrant (Orserdu).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.







Top tweets by impressions — click to view on X
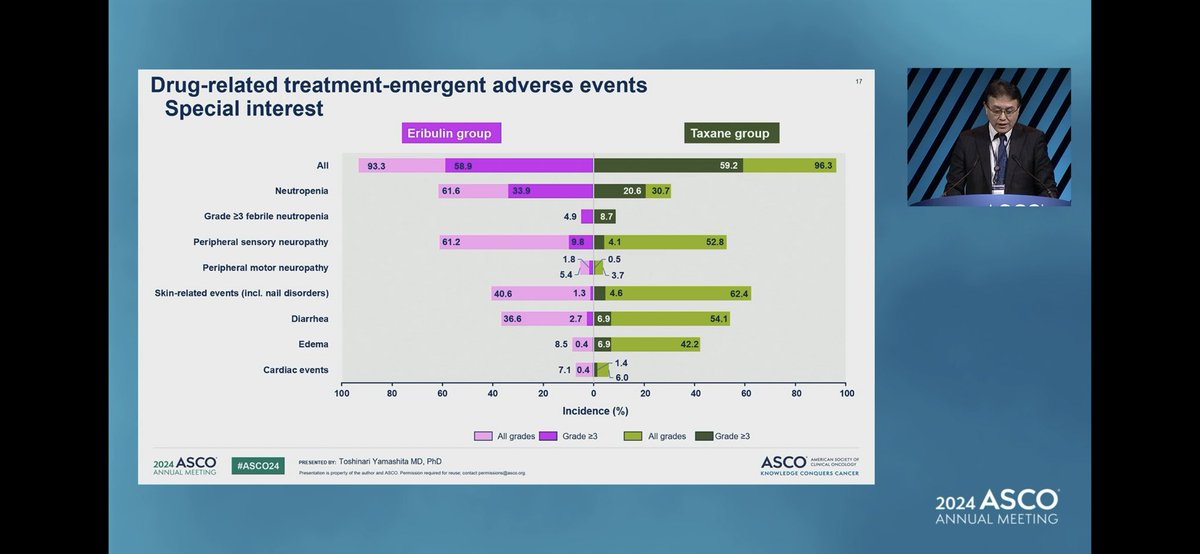
Toshinari Yamashita presents their Emerald trial #ASCO24 58% de novo HER2+ MBC. Eribulin non inferior to taxane with HP but more neutropenia and peripheral neuropathy. An alternative to taxane in…
Breast Cancer Highlights from #ASCO24 w/ @ErikaHamilton9
- #RxPonder
- #postMONARCH
- #INAVO120
- #DB06
- #EMERALD
Full Int:
- https://t.co/ukNyzlPC8Y
- https://t.co/Q0WZyfiGBl
- Also on the…
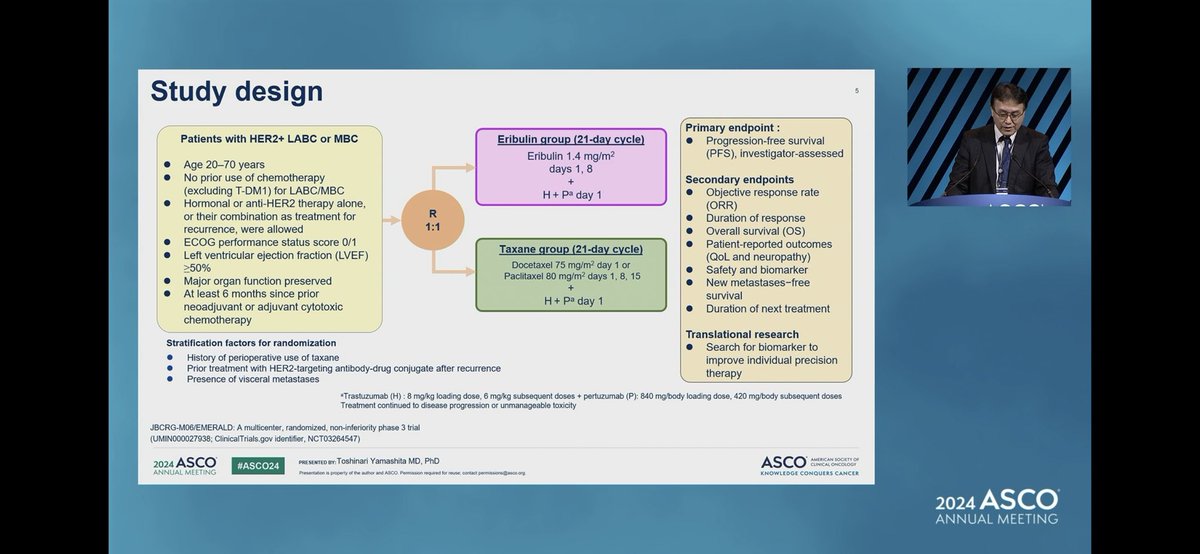
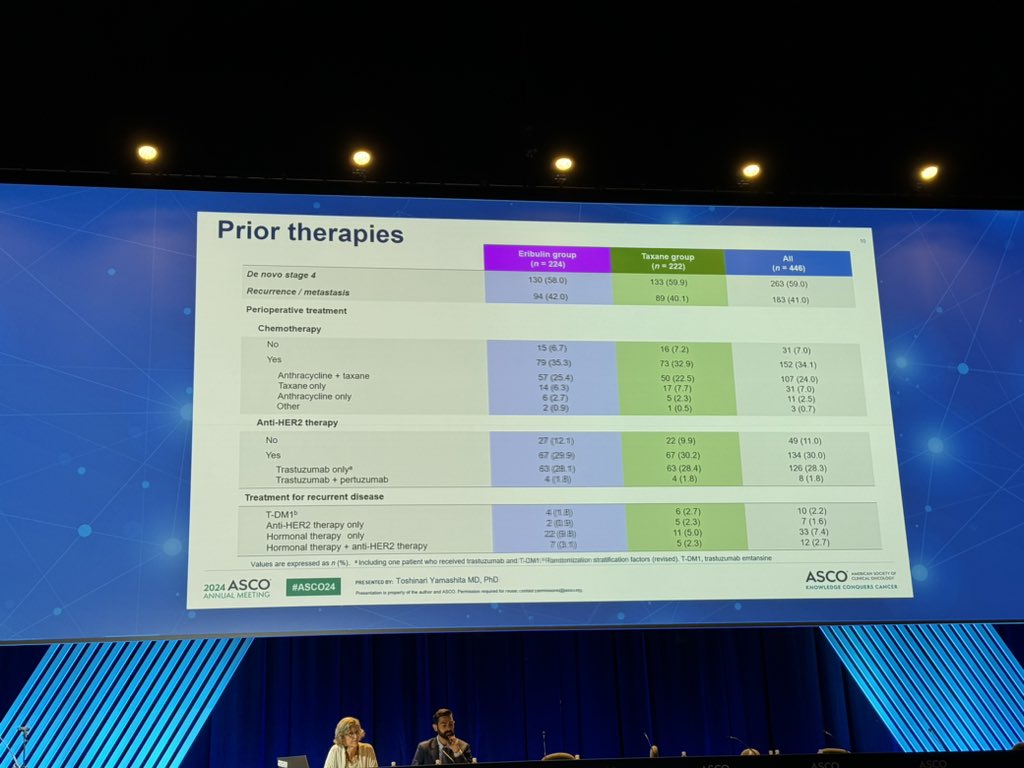
Eribulin + HP vs THP in 1L HER2+ MBC (JBCRG-M06/EMERALD Study)
n=446 (57% HR+, ~60% de novo, ~30% prior HER2-directed tx in early stage)
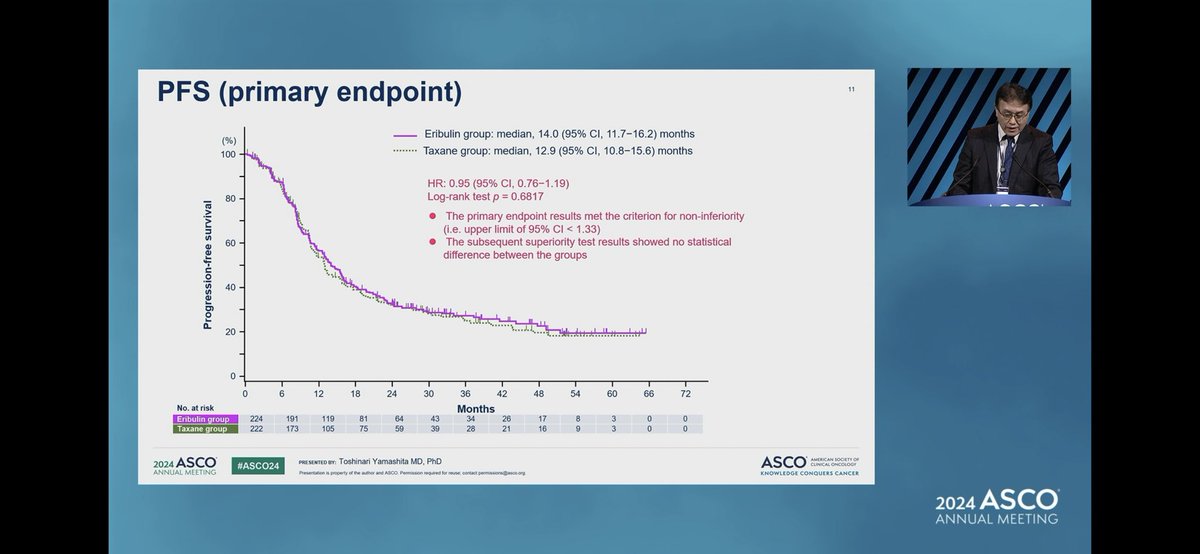
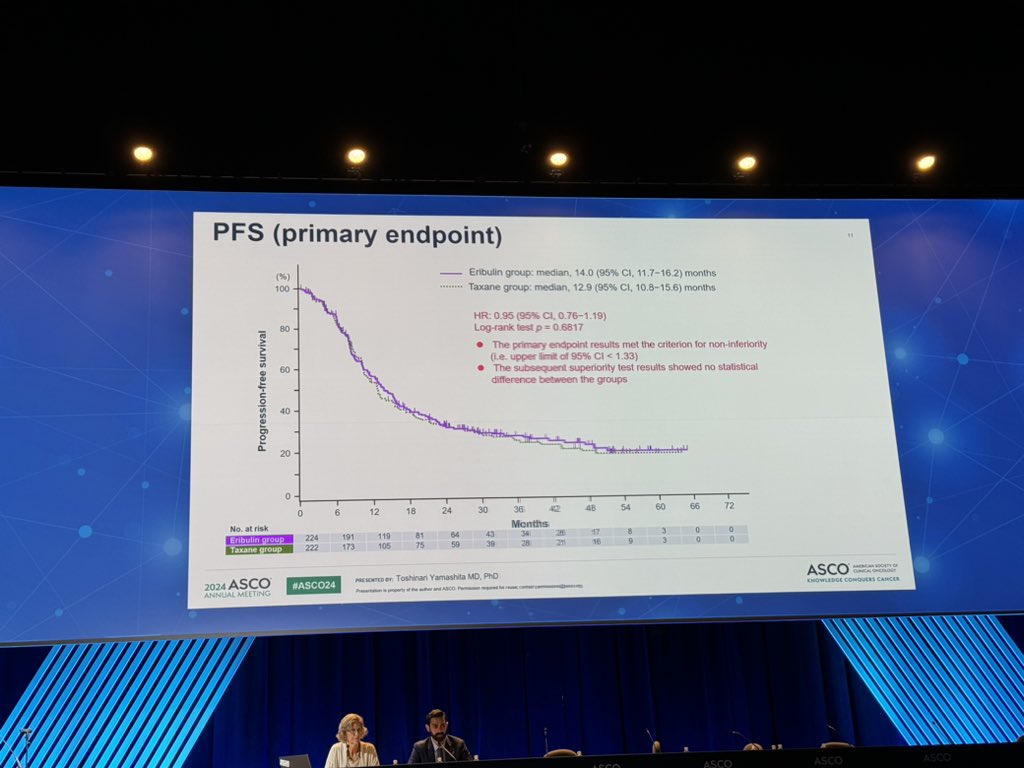
12.9 mo vs 14.0 mo HR 0.95 p=0.6817
ORR ~76% in both groups.…
Just presented at #ASCO24 the results of the phase 3 EMERALD trial showing the non-inferiority of #eribulin vs. docetaxel/paclitaxel together with #trastuzumab plus #pertuzumab as first-line therapy…
The EMERALD trial shows eribulin + dual HER2 blockade (HP) is non-inferior to taxane + HP for 1st line treatment of HER2+ metastatic breast cancer.
Eribulin improves patient quality of life with…
@hoperugo However, in the clinics, we usually see more robust responses with taxanes. Having had prior taxanes might have affected the results and some tilt in favor of eribulin?!

@SuyogCancer Think EMERALD study post ASCO24 might change the 1st line HER2+ MBC

@stolaney1 @OncoAlert Thanks for checking our study.
EMERALD established elacestrant (Orserdu) as the first oral SERD approved (January 27, 2023) for ESR1-mutated ER+/HER2- advanced/mBC after at least one line of ET. Benefit is strongest in patients with prior ET+CDK4/6i ≥12 months (mPFS 8.6 vs. 1.9 mo), supporting its role in endocrine-sensitive tumors that acquired ESR1 resistance. Real-world outcomes exceed trial efficacy. Competes with camizestrant (SERENA-6), imlunestrant (EMBER-3), and vepdegestrant (VERITAC-2) — the latter two both with pivotal 2024/2025 readouts. EMERALD's 12+ mo prior-CDK4/6i subgroup defines the ideal real-world use.
Median: 3.8 months (elacestrant 345 mg daily) vs. 1.9 months (SOC endocrine therapy (AI or fulvestrant)). HR 0.55 (95% CI 0.39-0.77), P=0.0005 ESR1m + prior ET+CDK4/6i ≥12 mo median PFS: 8.6 months (elacestrant) vs. 1.9 months (SOC). In ESR1-mutated ER+/HER2- mBC: median PFS 3.8 months (elacestrant) vs. 1.9 months (SOC); HR 0.55 (95% CI 0.39-0.77, P=0.0005) — 45% reduction in risk of progression/death. Subgroup with prior ET+CDK4/6i ≥12 months (n=222): median PFS 8.6 vs. 1.9 months (HR 0.41, 95% CI 0.26-0.63). Overall population (N=478): mPFS 2.8 vs. 1.9 months (HR 0.70). Consistent benefit across subgroups (bone mets, liver/lung mets, ≥3 metastatic sites, PIK3CA mut, HER2-low, ESR1 variant D538G/Y537S/N). Bidard et al., JCO 2022.
Overall survival data were immature at primary analysis and in subsequent updates. FDA approval (January 2023) was based on PFS benefit in ESR1m population. Patient-reported outcomes (PROs) from QLQ-C30, PRO-CTCAE, and EQ-5D-5L tools showed QoL was MAINTAINED between treatment groups with no clinically meaningful differences in adverse effects of interest (nausea, vomiting, fatigue, joint/muscle pain, hot flashes).
Key AEs: nausea (most common with elacestrant), vomiting, fatigue, joint and muscle pain, hot flashes. Grade ≥3 TRAE rates per Bidard 2022 JCO: nausea Grade ≥3 was 2.5% (elacestrant). Overall manageable safety profile, oral once-daily dosing. Discontinuation rate low. No dose-limiting cardiac/hepatic signals. Full safety detailed in JCO 2022 primary publication.
✅ FDA-approved (Jan 2023): first oral SERD for ESR1m ER+/HER2- advanced BC post-ET+CDK4/6i. EMERALD established elacestrant (Orserdu) as the first oral SERD approved (January 27, 2023) for ESR1-mutated ER+/HER2- advanced/mBC after at least one line of ET. Benefit is strongest in patients with prior ET+CDK4/6i ≥12 months (mPFS 8.6 vs. 1.9 mo), supporting its role in endocrine-sensitive tumors that acquired ESR1 resistance. Real-world outcomes exceed trial efficacy. Competes with camizestrant (SERENA-6), imlunestrant (EMBER-3), and vepdegestrant (VERITAC-2) — the latter two both with pivotal 2024/2025 readouts. EMERALD's 12+ mo prior-CDK4/6i subgroup defines the ideal real-world use.
EMERALD is a Phase 3 randomized trial (NCT03778931) of the oral selective estrogen receptor degrader (SERD) elacestrant (Orserdu) versus standard-of-care endocrine therapy - fulvestrant or an aromatase inhibitor - in ER-positive, HER2-negative advanced or metastatic breast cancer that progressed after prior endocrine therapy plus a CDK4/6 inhibitor. Progression-free survival in the ITT and ESR1-mutated populations were dual primary endpoints.
Elacestrant improved progression-free survival in the ESR1-mutated population (median 3.8 vs 1.9 months; HR 0.55; 95% CI 0.39-0.77; P=0.0005), and the benefit was greatest in ESR1-mutated patients with at least 12 months of prior endocrine therapy plus a CDK4/6 inhibitor, where median PFS was 8.6 versus 1.9 months. Overall survival was immature.
Yes. On January 27, 2023 the FDA approved elacestrant (Orserdu) for postmenopausal women or adult men with ER-positive, HER2-negative, ESR1-mutated advanced or metastatic breast cancer whose disease progressed after at least one line of endocrine therapy. It was the first oral SERD approved for this population, with the Guardant360 CDx test used to identify ESR1 mutations.
The greatest benefit is in patients with ESR1 mutations, particularly those who had at least 12 months of prior endocrine therapy plus a CDK4/6 inhibitor before progression. Patients are selected using an FDA-approved test for ESR1 mutations (Guardant360 CDx), so ESR1 mutation testing is required to identify candidates for elacestrant.
Elacestrant is an oral once-daily therapy with a generally manageable safety profile. The most common adverse events were nausea (the most frequent), vomiting, fatigue, joint and muscle pain, and hot flashes; Grade 3 or higher nausea was uncommon (about 2.5%). The overall tolerability supported its use as an oral single-agent endocrine option.