GMMG-HD6 is a Phase 3, four-arm trial testing whether adding the SLAMF7 antibody elotuzumab (Empliciti) to RVd induction/consolidation and/or lenalidomide maintenance improves outcomes in transplant-eligible newly diagnosed multiple myeloma. It was negative: 3-year PFS was 69/69/66/67% across arms (adjusted P=0.86), with no overall-survival benefit. The frontline elotuzumab-RVd regimen is investigational. Sponsor: GMMG (University Hospital Heidelberg).
Discover KOL Sentiment on GMMG-HD6 →Design — Phase 3, 4-arm randomized (1:1:1:1); elotuzumab (Empliciti) added to RVd induction/consolidation and/or lenalidomide maintenance vs RVd alone, transplant-eligible NDMM, n=555 (NCT02495922). (Lancet Haematol 2024)
PFS (primary) — NEGATIVE — no difference across arms: 3-year PFS 69% (RVd/R) vs 69% (RVd/E-R) vs 66% (E-RVd/R) vs 67% (E-RVd/E-R); adjusted log-rank P=0.86; median follow-up 49.8 mo. (Lancet Haematol 2024)
Overall survival — OS comparable across all four arms; no survival benefit from adding elotuzumab at any phase. (Lancet Haematol 2024)
Safety — Grade >=3 infections (most common AE) 20% (RVd/R) / 23% (RVd/E-R) / 25% (E-RVd/R) / 34% (E-RVd/E-R); serious AEs highest in the elotuzumab quadruplet (48%); 9 treatment-related deaths total. (Lancet Haematol 2024)
Regulatory / conclusion — Elotuzumab-containing therapy should remain reserved for the relapsed/refractory setting (ELOQUENT-2/-3). Frontline elotuzumab-RVd is investigational and NOT FDA approved. (FDA label)
Sponsor / Drug — GMMG (University Hospital Heidelberg); elotuzumab (Empliciti), an anti-SLAMF7 monoclonal antibody, added to the RVd backbone. (Lancet Haematol 2024)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.




Top tweets by impressions — click to view on X
Save the FISH - still a useful tool in clinal routine! GMMG-HD6 was an excellent trial. I never thought that Elotuzumab had no benefit in any treatment sequence! #ASH24 #mmsm https://t.co/1XxVrFeqMN
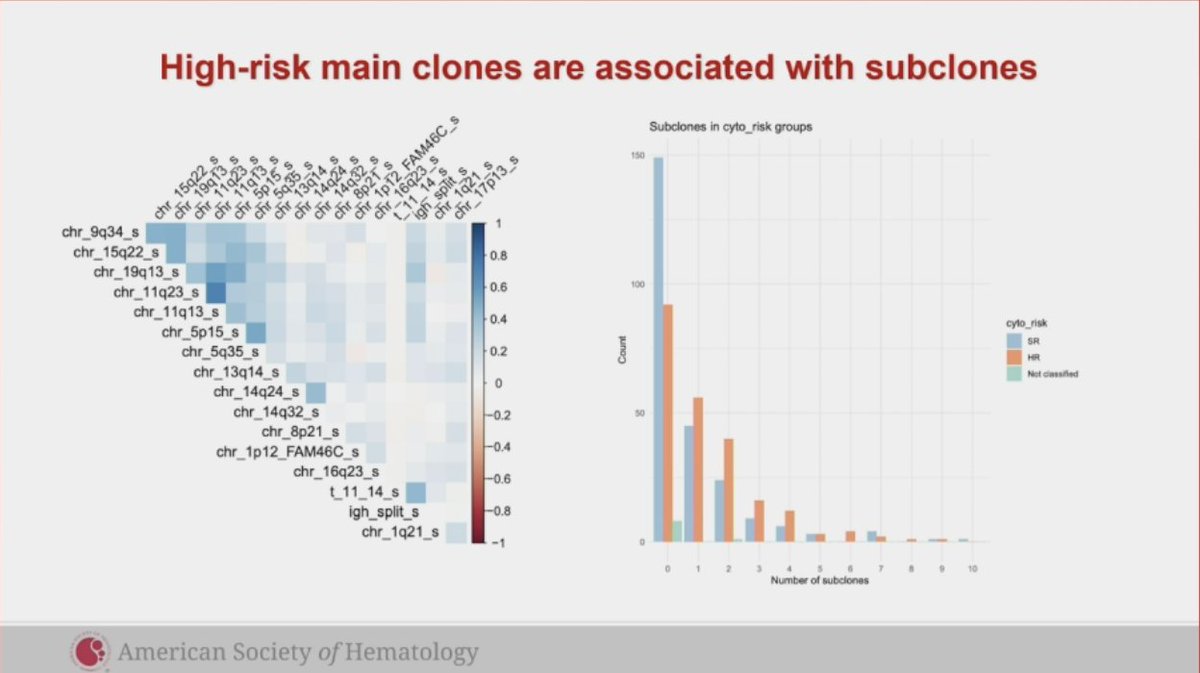
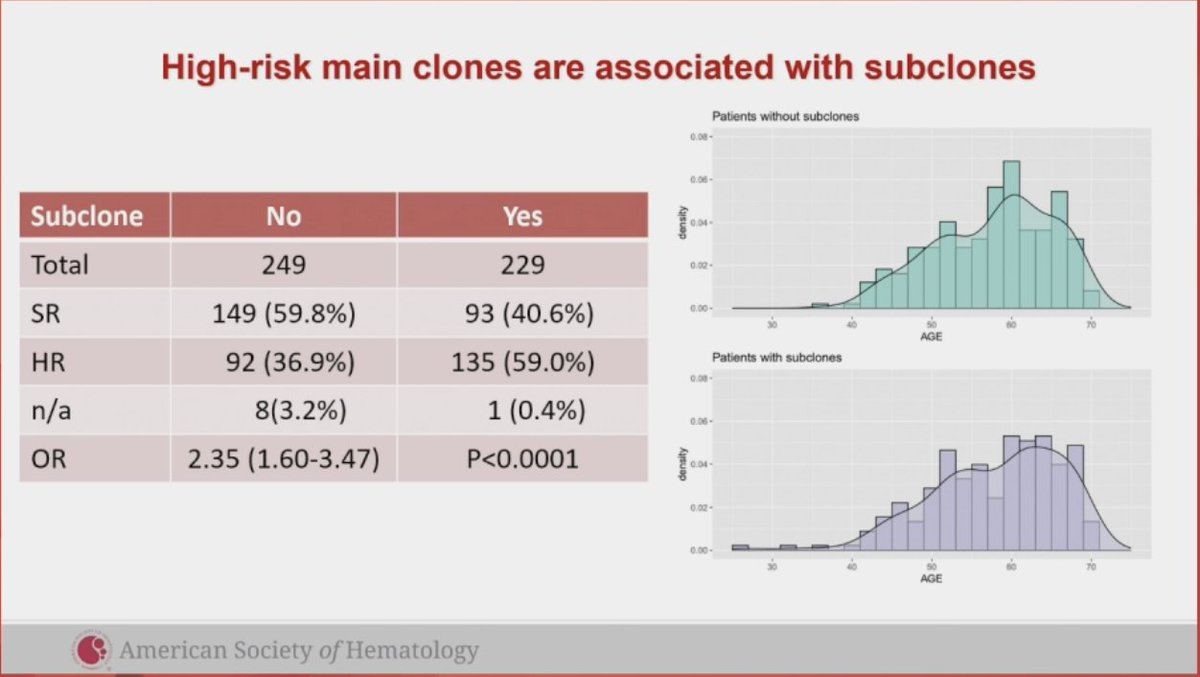
Impact of Clonal Heterogeneity in Newly Diagnosed, Transplant-Eligible Multiple Myeloma -- Subgroup Analysis of the GMMG HD6 Phase III Trial [Dec 7, 2024] Merz et al. #ASH24 Abst 84…
#ASH24 #mmsm
Oral myeloma: Impact of Clonal Heterogeneity in Newly Diagnosed, Transplant-Eligible Multiple Myeloma – Subgroup Analysis of the GMMG HD6 Phase III Trial
Subclones are common in…
GMMG-HD6 is the first and definitive Phase 3 trial showing that adding the SLAMF7 mAb elotuzumab to standard RVd induction/consolidation and lenalidomide maintenance does NOT improve PFS or OS in transplant-eligible NDMM. Results contrast with positive ELOQUENT-2 and ELOQUENT-3 trials in RRMM. Elotuzumab's role in myeloma remains limited to relapsed/refractory settings per ELOQUENT-3 (Elo-Pd) and ELOQUENT-2 (Elo-Rd). For NDMM, the landscape has moved toward anti-CD38 quadruplets: daratumumab-RVd (PERSEUS, GRIFFIN) and isatuximab-RVd (GMMG-HD7) — a stark contrast with GMMG-HD6's negative signal.
3-year PFS by arm rate: 69% (RVd/R) vs. 69% (RVd/E-R) vs. 66% (E-RVd/R) vs. 67% (E-RVd/E-R). Phase 3 4-arm randomized trial (N=555, randomized 1:1:1:1). Median follow-up 49.8 months (IQR 43.7-55.5). NO DIFFERENCE in PFS between the four arms: 3-year PFS rates 69% (RVd/R), 69% (RVd/E-R), 66% (E-RVd/R), 67% (E-RVd/E-R). Adjusted log-rank P=0.86. Adding elotuzumab to RVd induction/consolidation OR lenalidomide maintenance did NOT provide clinical benefit. Mai et al., Lancet Haematol 2024;11(2):e101-e113.
OS comparable across all 4 arms; no survival benefit from adding elotuzumab to any treatment phase. Trial concluded elotuzumab-containing therapies should be reserved for the relapsed/refractory setting (per ELOQUENT-2 and ELOQUENT-3).
Grade ≥3 infections (most common AE): 20% (RVd_R) vs. 23% (RVd_E_R) vs. 25% (E_RVd_R) vs. 34% (E_RVd_E_R) — highest in the E-RVd/E-R quadruplet, lowest in standard RVd/R. Serious AEs (Grade ≥3): up to 48%, highest in the four-drug E-RVd/E-R arm. Nine treatment-related deaths total: RVd/R 2 (sepsis, toxic colitis); RVd/E-R 1 (meningoencephalitis); E-RVd/R 4 (pulmonary embolism, septic shock, atypical pneumonia, cardiovascular failure); E-RVd/E-R 2 (sepsis, pneumonia/pulmonary fibrosis).
❌ Negative Phase 3: Elotuzumab adds no benefit to RVd in transplant-eligible NDMM. GMMG-HD6 is the first and definitive Phase 3 trial showing that adding the SLAMF7 mAb elotuzumab to standard RVd induction/consolidation and lenalidomide maintenance does NOT improve PFS or OS in transplant-eligible NDMM. Results contrast with positive ELOQUENT-2 and ELOQUENT-3 trials in RRMM. Elotuzumab's role in myeloma remains limited to relapsed/refractory settings per ELOQUENT-3 (Elo-Pd) and ELOQUENT-2 (Elo-Rd). For NDMM, the landscape has moved toward anti-CD38 quadruplets: daratumumab-RVd (PERSEUS, GRIFFIN) and isatuximab-RVd (GMMG-HD7) — a stark contrast with GMMG-HD6's negative signal.
GMMG-HD6 is a Phase 3, randomized (1:1:1:1) investigator-initiated trial (NCT02495922) of 555 transplant-eligible patients with newly diagnosed multiple myeloma, testing whether adding the anti-SLAMF7 antibody elotuzumab (Empliciti) to RVd (lenalidomide, bortezomib, dexamethasone) induction/consolidation and/or to lenalidomide maintenance improves outcomes. It was conducted by the German-Speaking Myeloma Multicenter Group (GMMG).
No. GMMG-HD6 was a negative trial. At a median follow-up of 49.8 months, 3-year progression-free survival was essentially identical across the four arms (69%/69%/66%/67%; adjusted log-rank P=0.86), and overall survival was comparable, so adding elotuzumab at any treatment phase provided no clinical benefit.
No. The frontline elotuzumab (Empliciti) + RVd regimen studied in GMMG-HD6 is investigational and is not FDA approved. Elotuzumab is FDA approved only for relapsed/refractory multiple myeloma — with lenalidomide-dexamethasone (ELOQUENT-2) and with pomalidomide-dexamethasone (ELOQUENT-3).
GMMG-HD6's negative signal for elotuzumab contrasts with the positive results for anti-CD38 antibody quadruplets in newly diagnosed myeloma — daratumumab-RVd (PERSEUS, GRIFFIN) and isatuximab-RVd (GMMG-HD7) — which have driven the field toward CD38-based induction rather than SLAMF7-directed therapy in the frontline setting.
Grade >=3 infections (the most common adverse event) increased with elotuzumab intensity: 20% (RVd/R), 23% (RVd/E-R), 25% (E-RVd/R) and 34% (E-RVd/E-R), with serious adverse events highest (48%) in the four-drug elotuzumab arm. There were nine treatment-related deaths overall, several infection-related, without any offsetting efficacy benefit.
