Transplant-eligible newly diagnosed multiple myeloma (NDMM) — University of Heidelberg Medical Center / German-Speaking Myeloma Multicenter Group (GMMG)
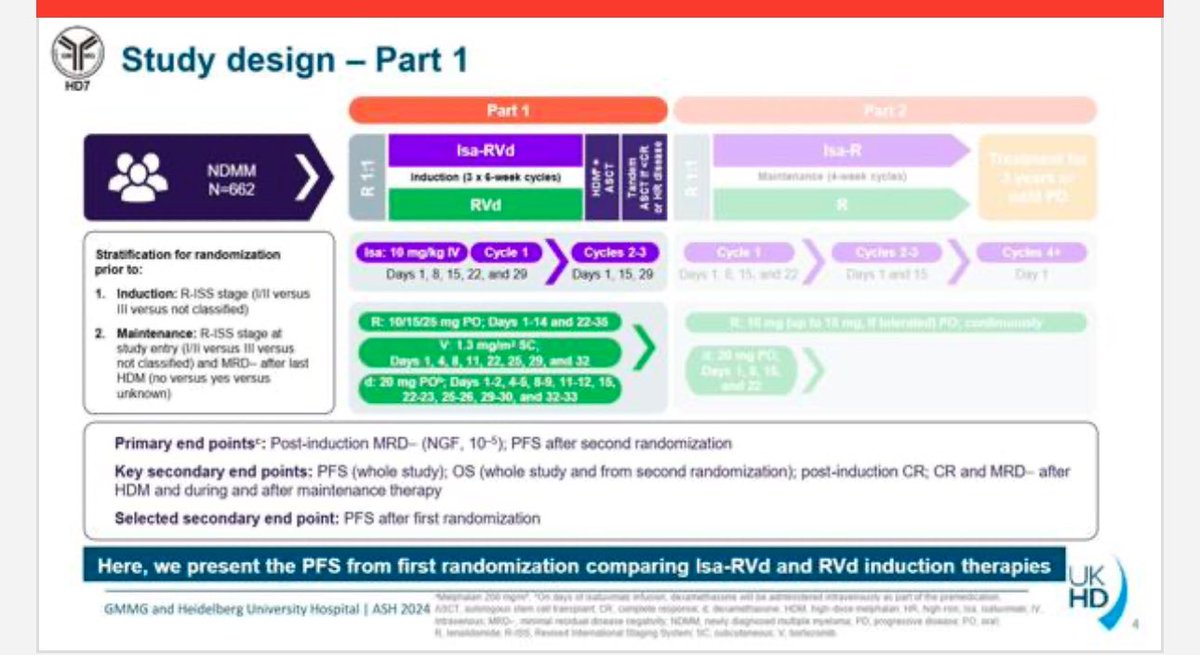
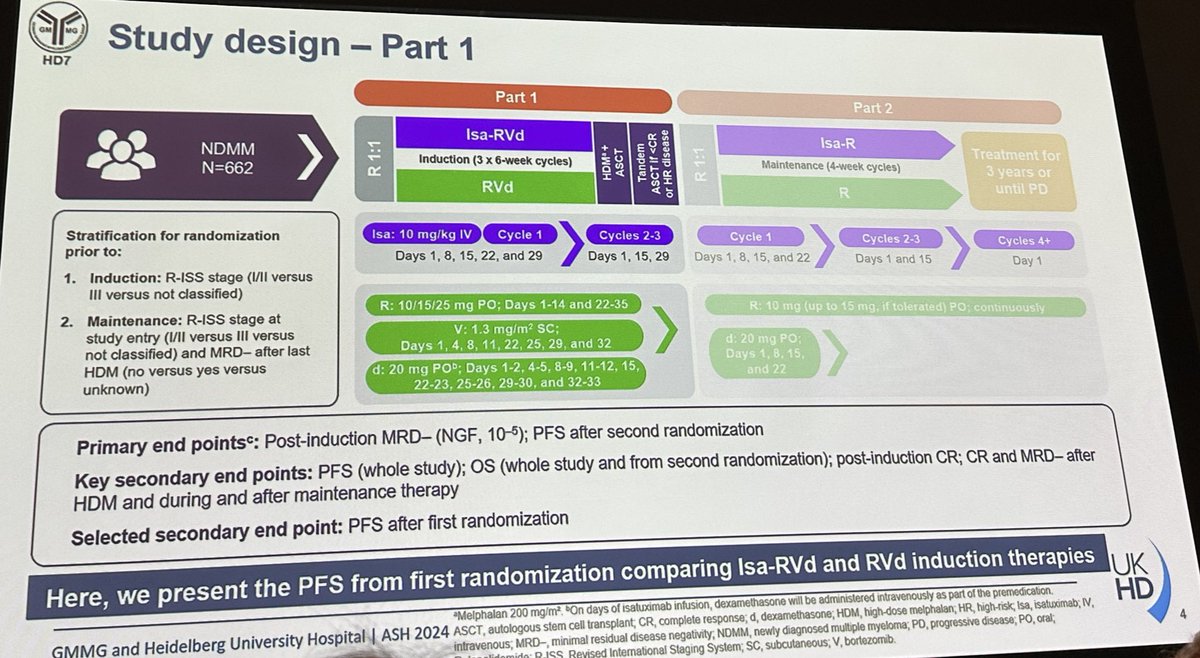
Discover KOL Sentiment on GMMG-HD7 →Design - Phase 3 isatuximab + RVd induction vs RVd induction, transplant-eligible NDMM (NCT03617731).
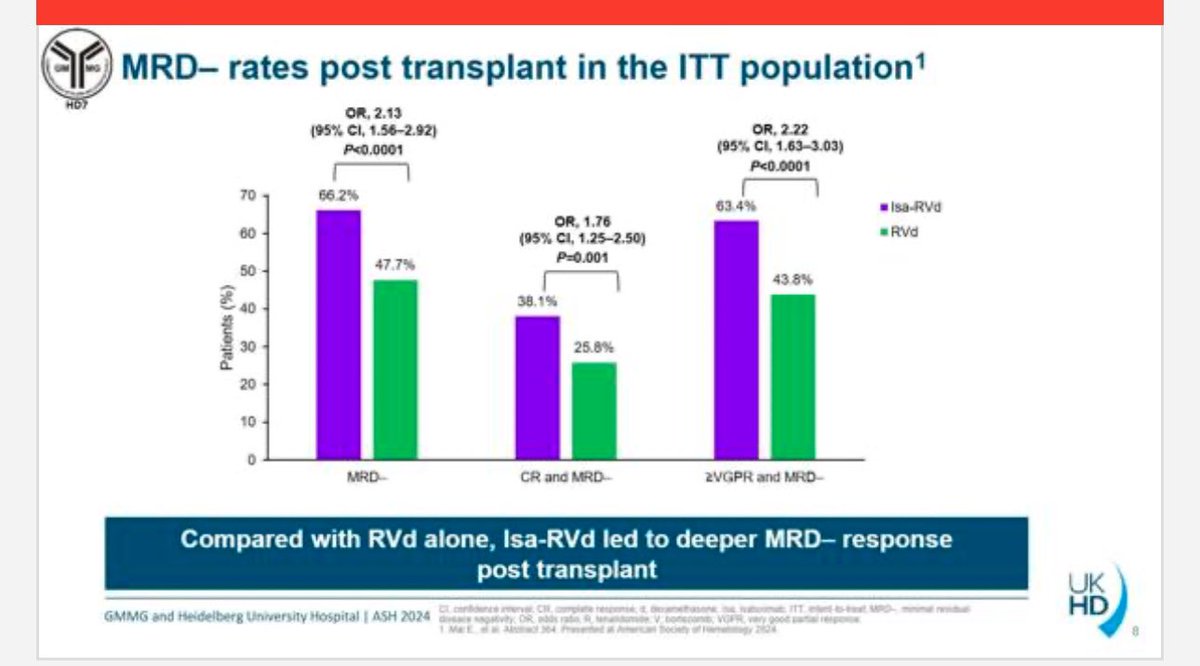
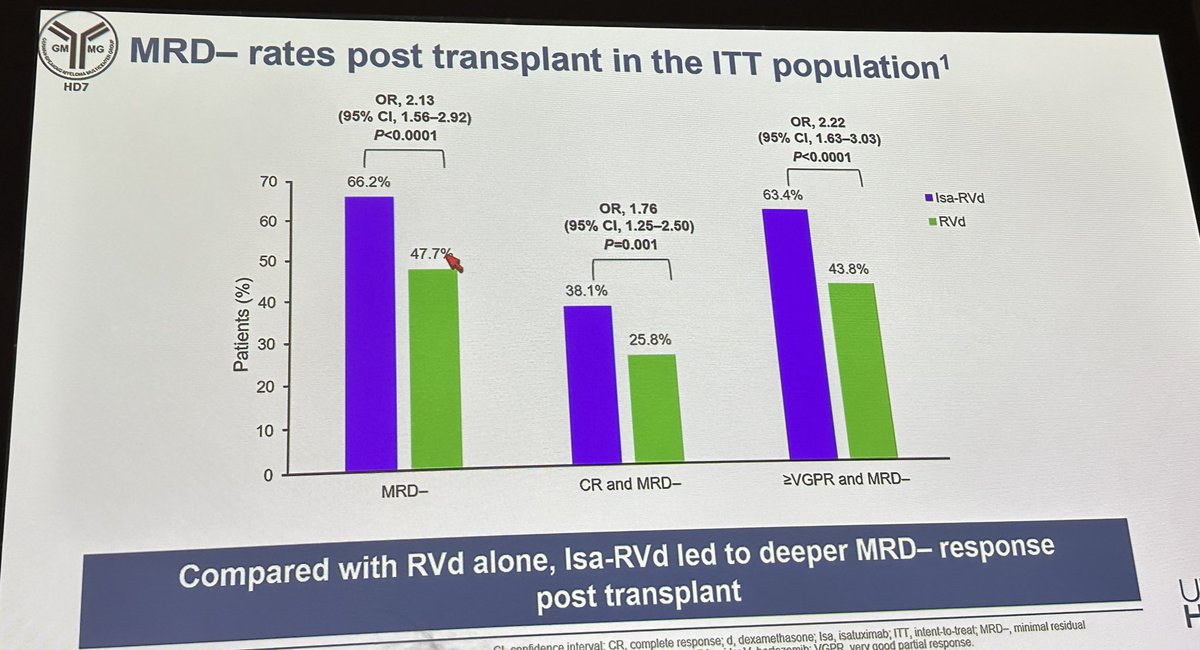
MRD-negativity (co-primary) - End-of-induction 50.1% vs 35.6% (OR 1.83, P<0.0001); post-transplant 66.2% vs 47.7%.
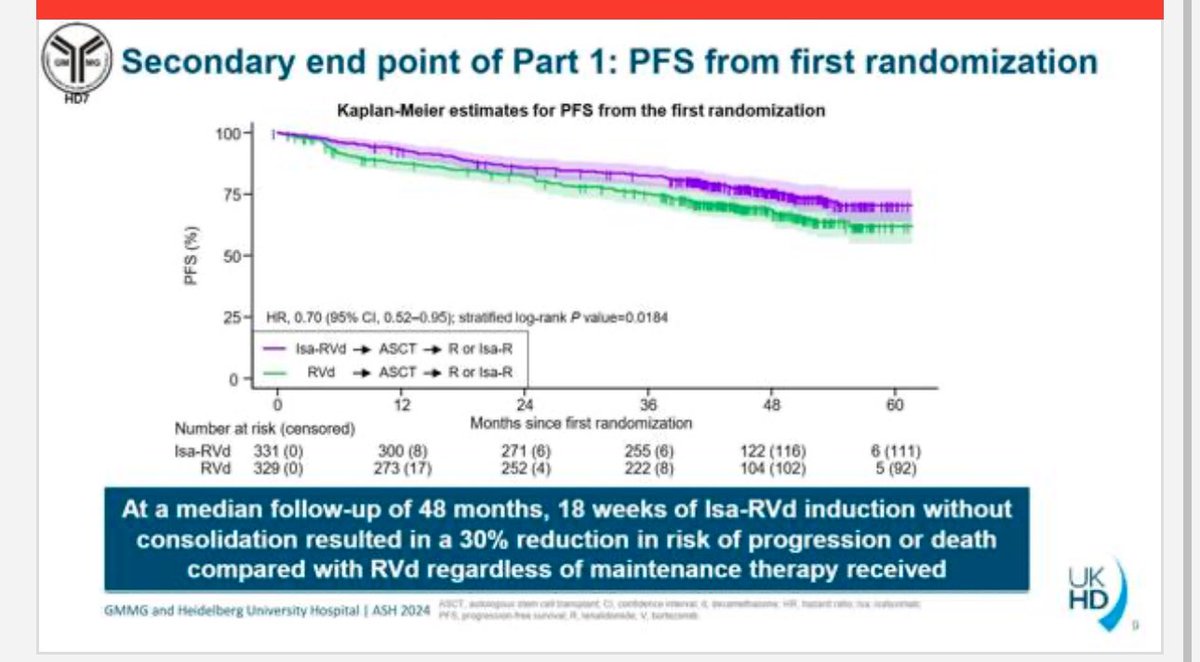
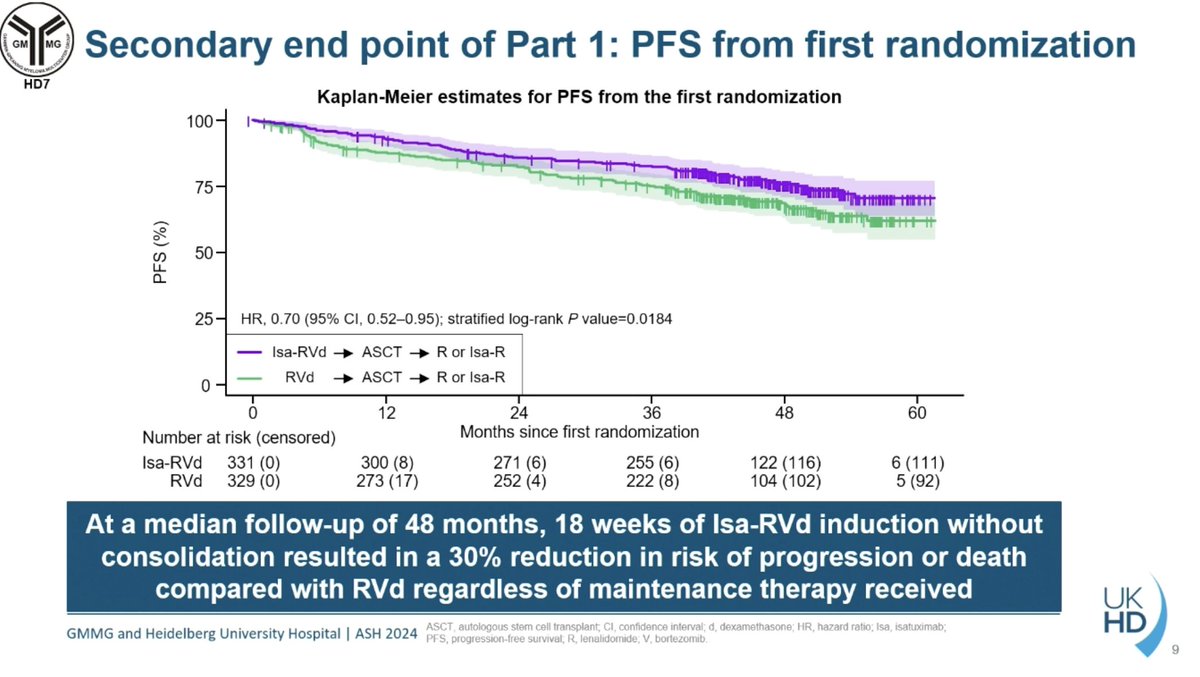
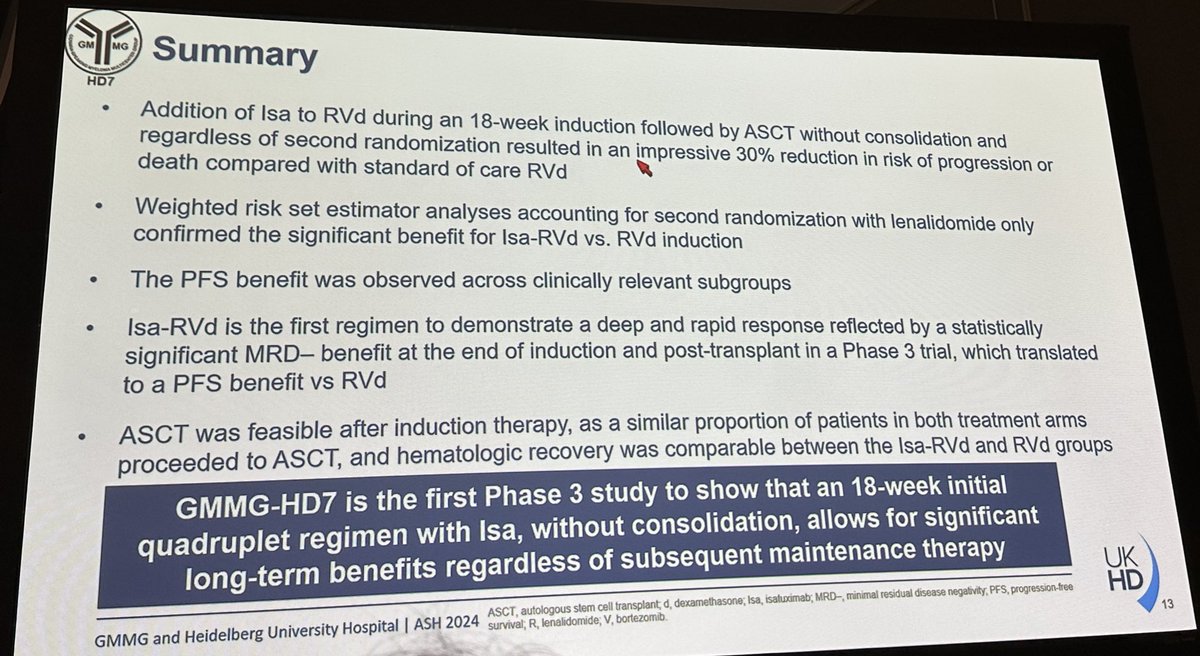
PFS (co-primary) - HR 0.70 (95% CI 0.52-0.95), P=0.0184 at median follow-up 48 months - a 30% reduction in risk of progression or death.
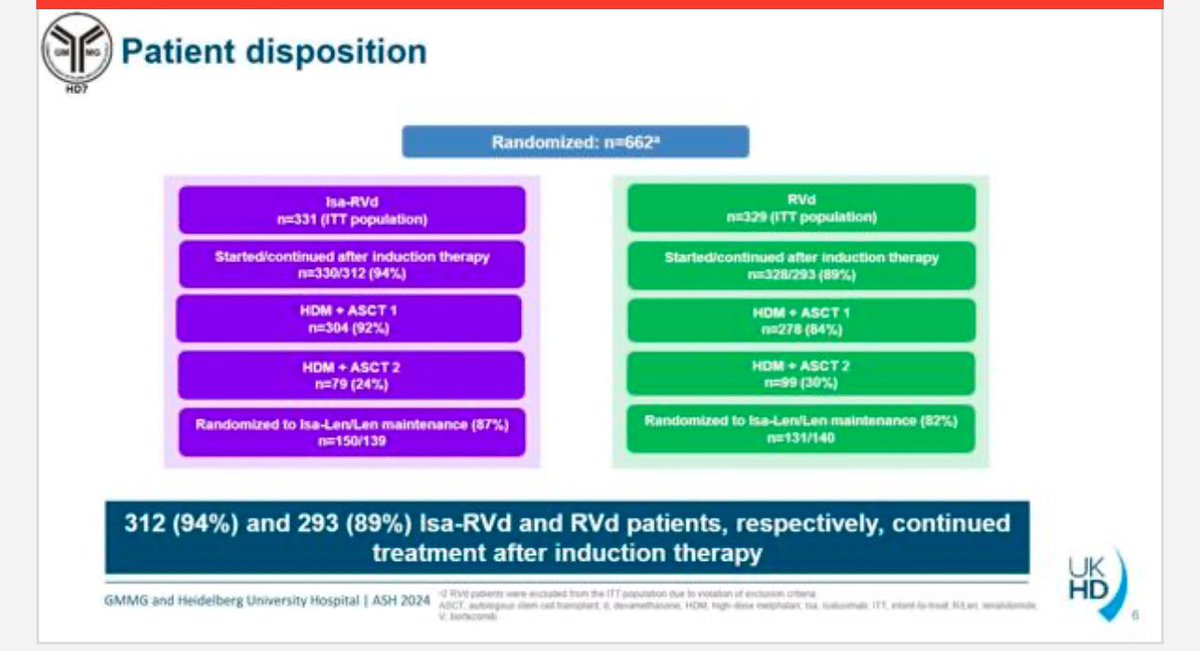
Safety - 94% (Isa-RVd) vs 89% (RVd) continued after induction; detailed Grade >=3 breakdown in the JCO 2025 publication.
Regulatory - Investigational - isatuximab is not FDA approved as frontline induction in transplant-eligible NDMM.
Sponsor / drug - GMMG / University of Heidelberg (Sanofi collaborator); isatuximab (Sarclisa).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.









Top tweets by impressions — click to view on X
Welcome to this @OncoAlert 🚨Session Round Up during #ASH24 in San Diego☀️
Todays Round up is on #MultipleMyeloma focusing on Pharmacologic Therapies: Refining the…
#1 Isatuximab-VRd vs VRd Induction for Newly Diagnosed Myeloma: Phase 3 GMMG-HD7
#HartmutGoldSchmidt @EliasKarlMai #ASH24
Well designed RCT. More to come in Part 2 later. Along with other RCTs,…
#ASH24 #mmsm @ASH_hematology
Oral myeloma: GMMG-HD7 final PFS analysis @EliasKarlMai
Very important to include anti-CD38 upfront for better PFS
second randomization will be very informative…
AEs & QOL
Key takeaway: manageable AE profiles w/ quads → preserved QOL
Safety analysis: Tolerable AE profiles support use of upfront quad tx for appropriate pts w/ TE NDMM
NCCN GLs
#MMBrief…

PFS update from GMMG-HD7 @EliasKarlMai: Despite ~25-30% of pts. receiving response/risk-adapted tandem ASCT, Isa-VRd induction led to a significant PFS benefit over VRd!
3-year PFS: 83% vs 75% (HR…
Open question: what changes once SQ isatuximab approved?
Comparing CD38-VRd between GMMG-HD7 ( @RaabMarc @EliasKarlMai et al) & PERSEUS, one difference is no post-ASCT consolidation in HD7 -…
#ASH25 #mmsm
@ASH_hematology
Friday satellite program
Summary table to induction regiments in transplant eligible myeloma patients https://t.co/GYjQEQ3RAJ

GMMG-HD7 (@EliasKarlMai) : Isa-VRd vs VRd induction --> ASCT x1-2--> Isa-R vs R (second randomization)
Isa-VRd > VRd induction with respect to PFS, even when accounting for second…

CONGRESS | #ASH24 | PRESENTATION
@EliasKarlMai @uniklinik_hd presents results from a landmark analysis of phase III GMMG-HD7 trial assessing the impact of induction regimen and post-induction and…
#ASH24 #ASHkudos to @EliasKarlMai for so many orals this year!
Paraphrasing - benefit of Isa-VRd quad over triplet most relevant in #MMsm pts who don’t achieve MRD negativity.
So maybe we should…
GMMG-HD7 is the first Phase 3 trial to show that an 18-week Isa-RVd induction followed by transplant (no consolidation) significantly improves both MRD-negativity and PFS vs. RVd in transplant-eligible NDMM, regardless of subsequent maintenance. Complements IMROZ (transplant-ineligible, FDA approved September 2024). Establishes Isa-RVd as the leading contender for new front-line SOC alongside Dara-VRd (PERSEUS, GRIFFIN, CASSIOPEIA). MRD-guided decision-making and 2nd randomization data awaiting maturation.
Median: 50.1 % MRD-neg (Isa-RVd (induction)) vs. 35.6 % MRD-neg (RVd (induction)). Post-transplant MRD negativity rate: 66.2% (Isa-RVd) vs. 47.7% (RVd). CR + MRD-neg post-transplant rate: 38.1% (Isa-RVd) vs. 25.8% (RVd). First co-primary endpoint met: MRD-negativity at end of 18-week induction was 50.1% with Isa-RVd vs. 35.6% with RVd (OR 1.83, 95% CI 1.34-2.51, P<0.0001). Post-transplant MRD-negativity deepened to 66.2% vs. 47.7% (OR 2.13, 95% CI 1.56-2.92, P<0.0001). 662 patients randomized 1:1. Second primary endpoint (PFS from 2nd randomization) awaiting data maturity. Mai et al., JCO 2025;43(11):1279-1288.
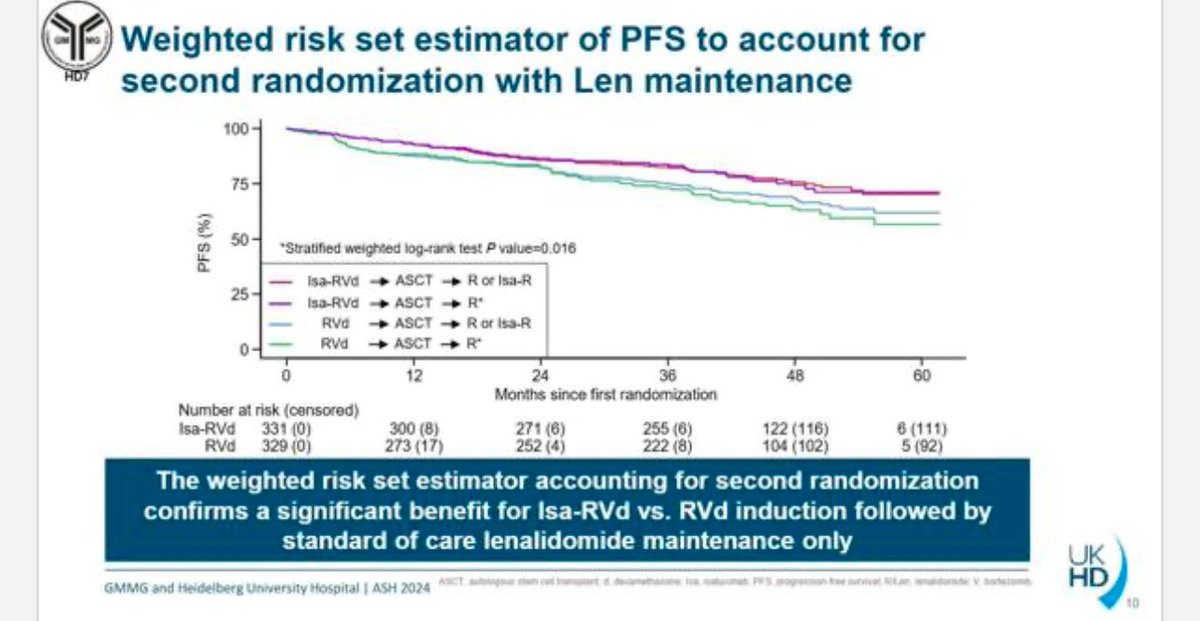
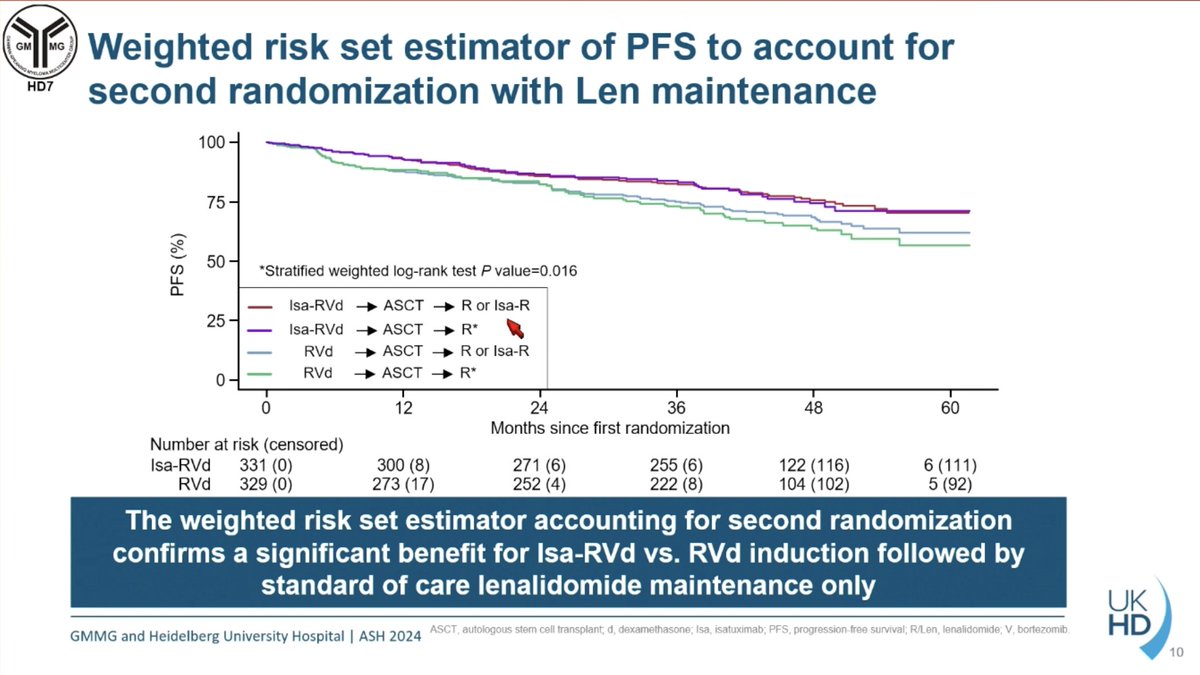
HR 0.7 (95% CI 0.52-0.95), P=0.0184 PFS from first randomization (secondary endpoint; see note below): HR 0.70 (95% CI 0.52-0.95, P=0.0184, stratified log-rank) at median follow-up 48 months — 30% reduction in risk of progression or death with Isa-RVd induction regardless of maintenance. Weighted risk set analysis accounting for 2nd randomization confirmed benefit when followed by lenalidomide-only maintenance (P=0.016). PFS in MRD-positive patients: HR 0.64 (95% CI 0.43-0.96, P=0.03) favoring Isa-RVd. OS data not yet reported (trial ongoing). Note: PFS from 1st randomization is a SECONDARY endpoint; PFS from 2nd randomization is the co-primary.
Full Grade ≥3 TRAE breakdown not in summary sources (detailed in JCO 2025 publication). 94% of Isa-RVd arm and 89% of RVd arm continued after induction. First transplant: 92% (Isa-RVd) vs. 84% (RVd). Tandem transplant: 24% vs. 30%. Safety profile consistent with established Isa + VRd combination.
🔄 First Phase 3 quadruplet trial showing deep MRD-negativity + PFS benefit in transplant-eligible NDMM. Potential label extension from IMROZ. GMMG-HD7 is the first Phase 3 trial to show that an 18-week Isa-RVd induction followed by transplant (no consolidation) significantly improves both MRD-negativity and PFS vs. RVd in transplant-eligible NDMM, regardless of subsequent maintenance. Complements IMROZ (transplant-ineligible, FDA approved September 2024). Establishes Isa-RVd as the leading contender for new front-line SOC alongside Dara-VRd (PERSEUS, GRIFFIN, CASSIOPEIA). MRD-guided decision-making and 2nd randomization data awaiting maturation.
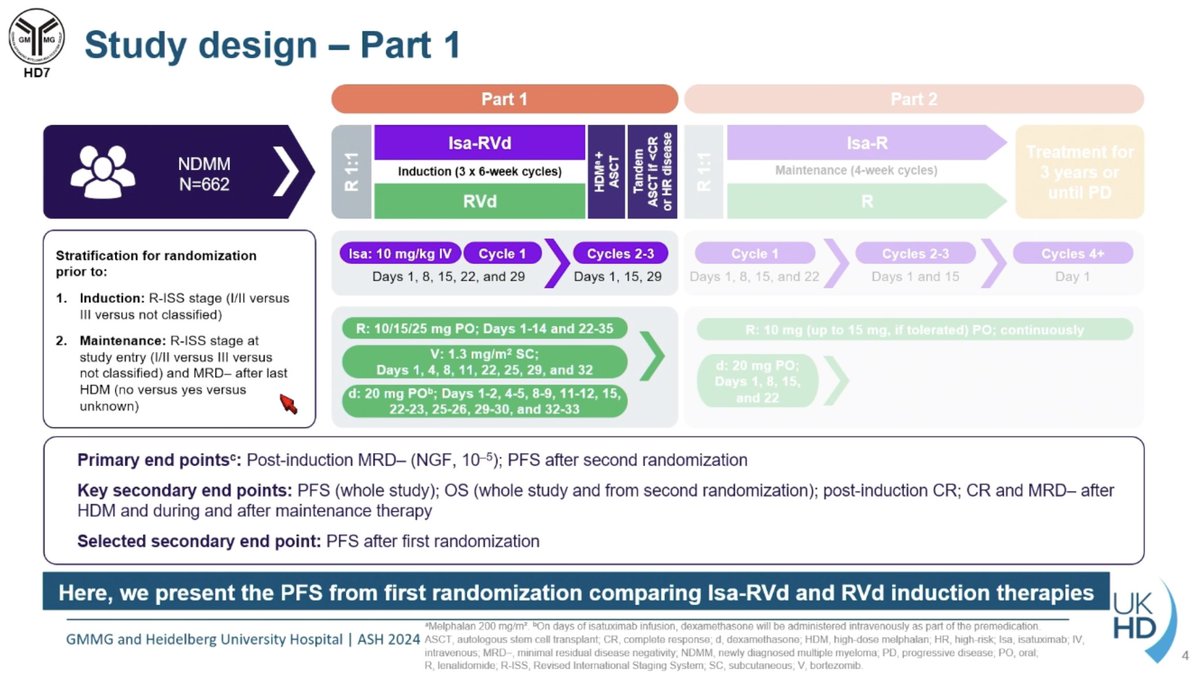
GMMG-HD7 is a Phase 3 randomized trial (NCT03617731) run by the German-Speaking Myeloma Multicenter Group testing isatuximab (Sarclisa) added to RVd (lenalidomide, bortezomib, dexamethasone) induction versus RVd induction alone in transplant-eligible newly diagnosed multiple myeloma. MRD negativity at end of induction and progression-free survival were dual primary endpoints.
Adding isatuximab to RVd induction significantly increased MRD-negativity at the end of induction (50.1% vs 35.6%; odds ratio 1.83; P<0.0001), a benefit that carried through after transplant (66.2% vs 47.7%). Progression-free survival also favored the isatuximab arm (HR 0.70; 95% CI 0.52-0.95; P=0.0184 at a median follow-up of 48 months), a 30% reduction in the risk of progression or death.
No. Isatuximab (Sarclisa) added to RVd induction for transplant-eligible newly diagnosed multiple myeloma, as studied in GMMG-HD7, is not FDA approved. Isatuximab is FDA approved in other multiple myeloma settings, including relapsed/refractory combinations and frontline with VRd in transplant-ineligible newly diagnosed myeloma (based on the IMROZ trial).
Treatment continuation after induction was high in both arms (94% with Isa-RVd versus 89% with RVd), and the addition of the anti-CD38 antibody isatuximab was generally consistent with the known safety profile of RVd plus an anti-CD38 agent. The full Grade 3 or higher adverse-event breakdown is detailed in the JCO 2025 publication.
GMMG-HD7 is one of the first Phase 3 trials to show that adding an anti-CD38 antibody (isatuximab) to a triplet induction deepens MRD-negativity and improves progression-free survival in transplant-eligible newly diagnosed myeloma, supporting the broader shift toward anti-CD38-containing quadruplet induction and providing rationale for potential label extension from the transplant-ineligible IMROZ data.

