Newly diagnosed advanced gastroesophageal adenocarcinoma (GEA) — University of Chicago (academic investigator-initiated; PI Daniel V.T. Catenacci)
Discover KOL Sentiment on PANGEA →Design — Academic Phase 2 (investigator-initiated, U Chicago); prospective serial biomarker-guided targeted-antibody + sequenced chemo strategy in advanced GEA (NCT02213289). (Cancer Discovery 2021)
OS (primary) — Median OS 15.7 mo (95% CI 13.8-20.8); 1-year OS ~69% vs historical control 50% (p<0.001). (Cancer Discovery 2021, page data)
Response — 1L objective response rate 74%; median 1L PFS 8.2 mo. (page data)
Safety — Grade ≥3 adverse events ~32% across 3 sequenced chemotherapy lines. (page data)
Regulatory — Investigational — not an FDA registration trial; no FDA approval. PANGEA-2 platform ongoing. (academic trial)
Sponsor / Strategy — University of Chicago (investigator-initiated, PI Daniel Catenacci); biomarker-guided sequential targeted antibody therapy. (Cancer Discovery 2021)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 20, 2026.







Top tweets by impressions — click to view on X
#ASH24 #mmsm
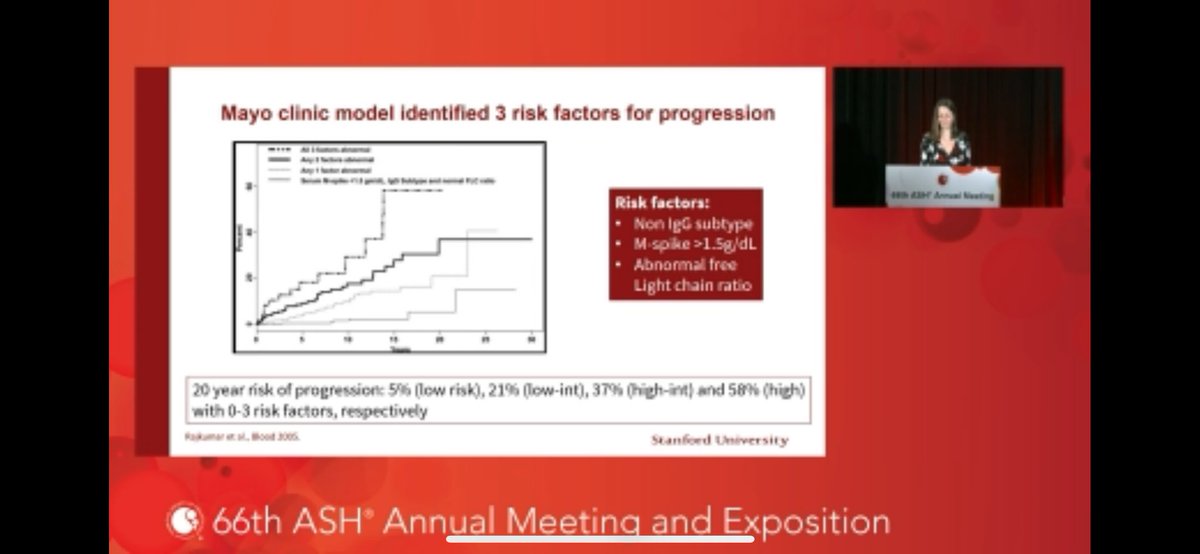
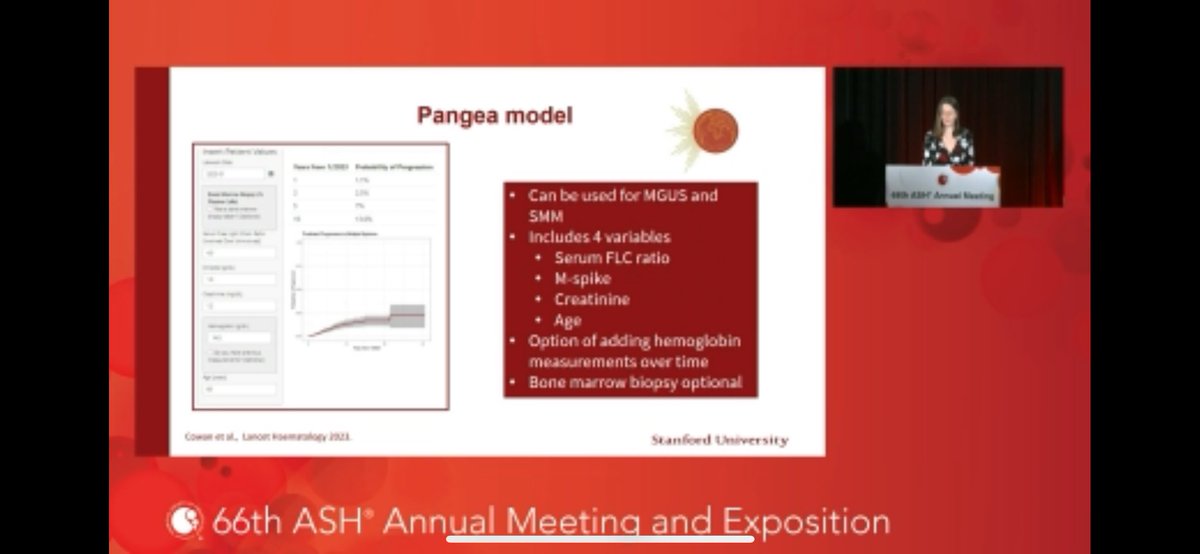
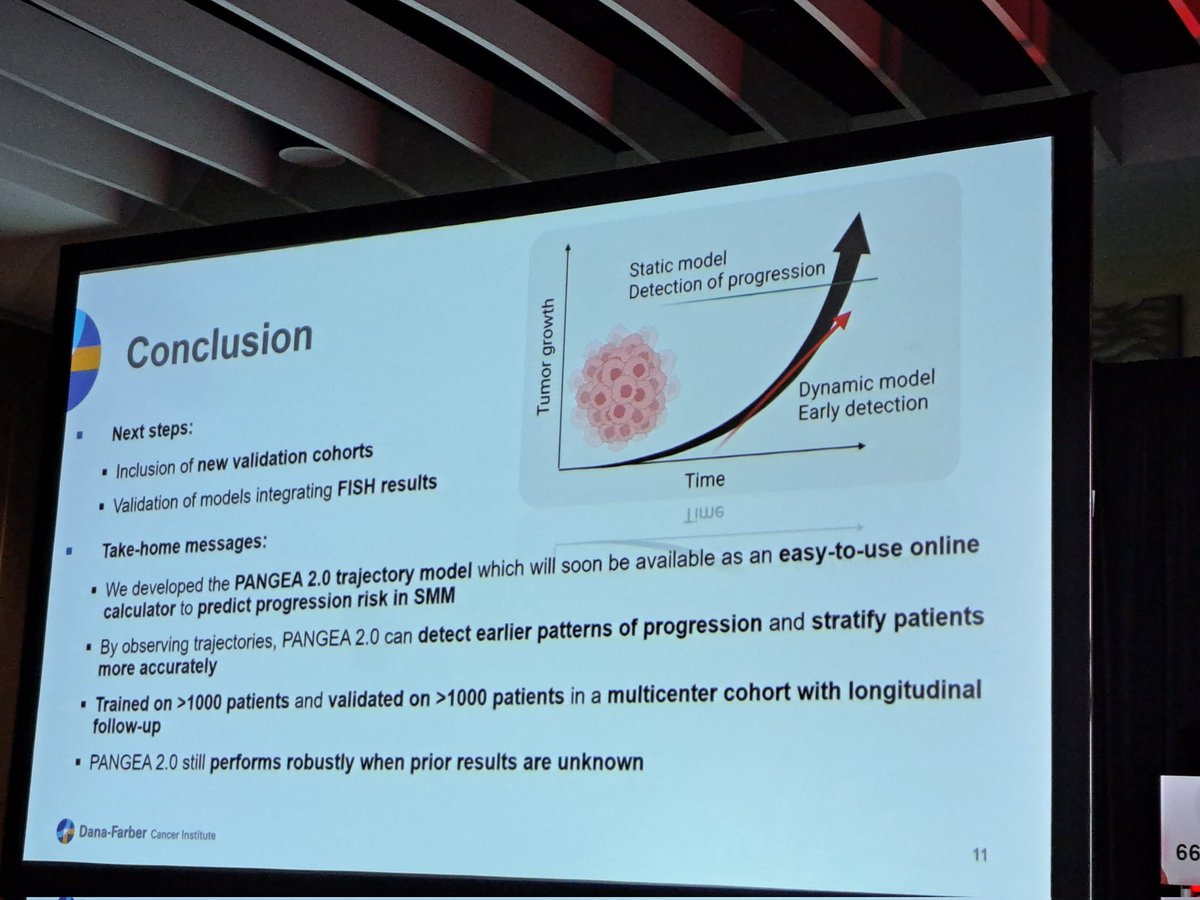
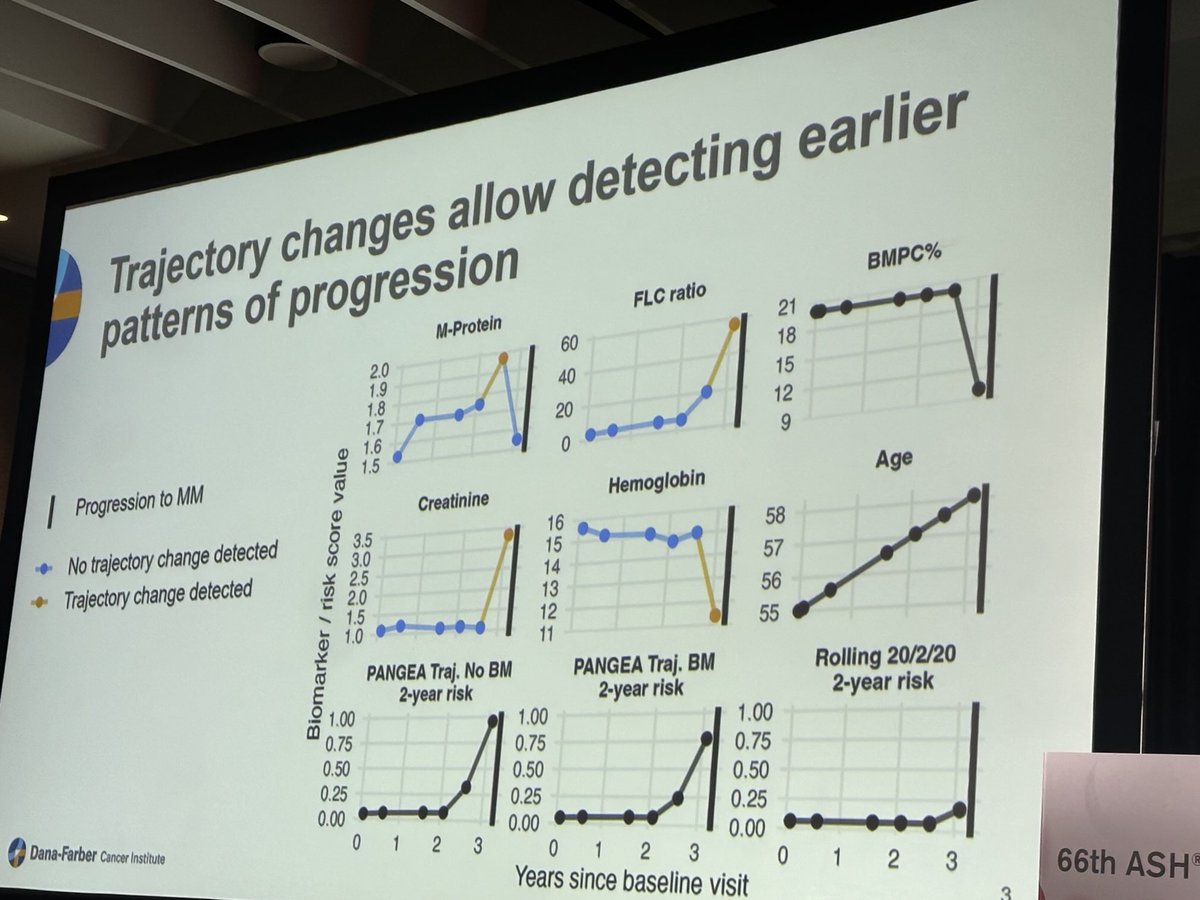
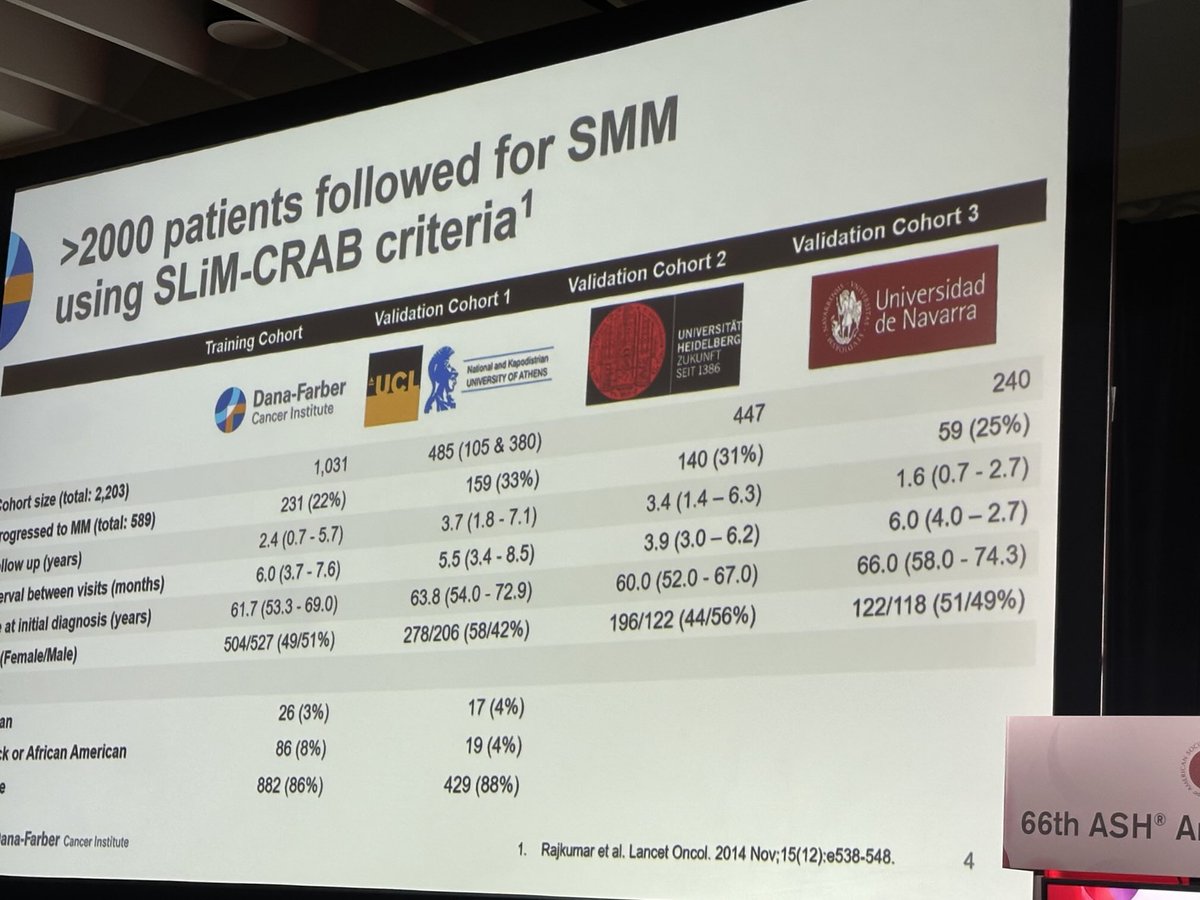
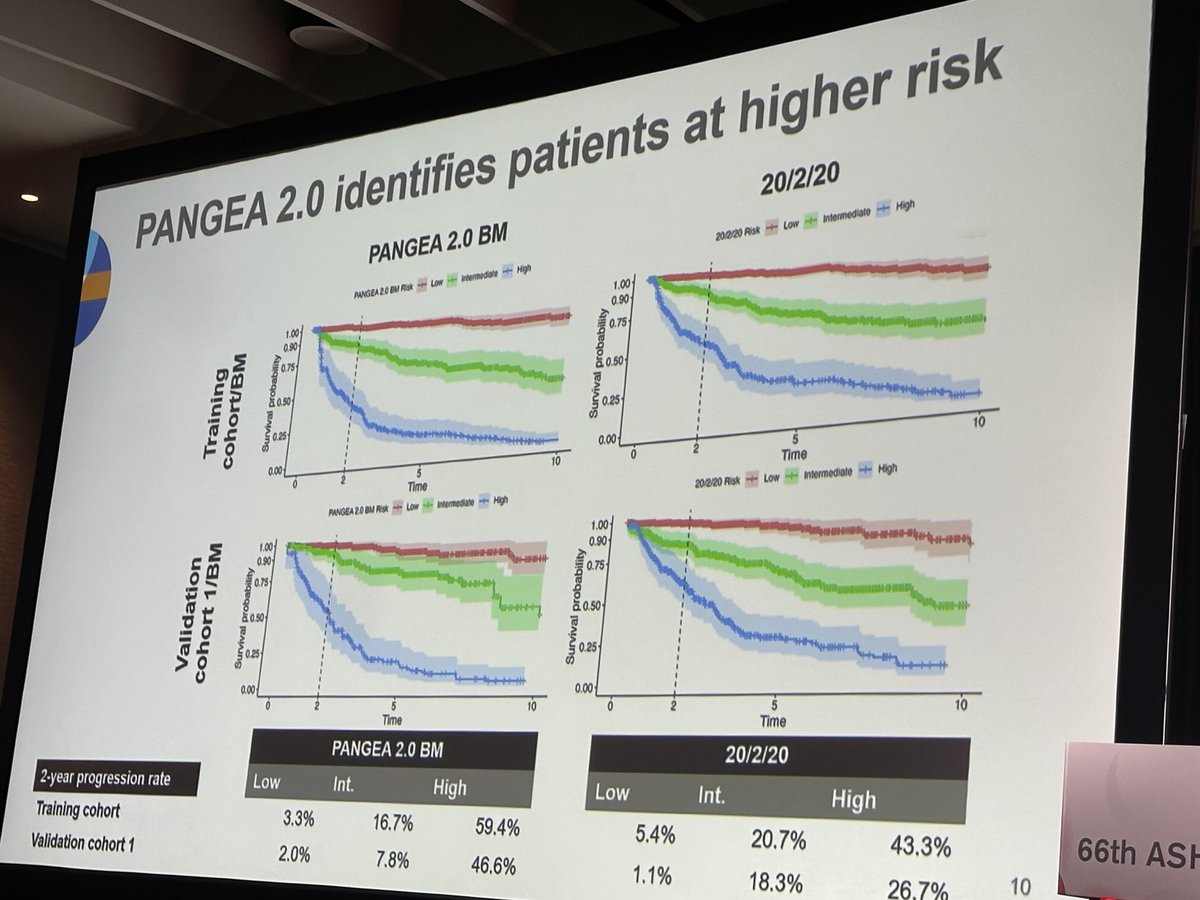
2️⃣ PANGEA- 2 model to predict progression of smoldering myeloma
➡️ https://t.co/gUuWRR59Wc
✅n=1431, longitudinal data on age, M-protein, FLCr, creatinine, and hemoglobin,BM PC…
The old model of categorizing MGUS would drive me crazy! Not all patients with “low risk” were as low risk as others. I’m going to try to use the Pangea model much more often now! #ASH24…
#ASH24 If minimally invasive, go dynamic and do not remain static! Great collaboration with @LabGhobrial @IrenemGhobrial towards the development of PANGEA 2.0 that relies on trajectory data to…
Pangea 2.0 risk stratification in >2000 smoldering MM. thanks to all our collaborators. We can predict progression early with evolving trajectory markers. #mmsm #ash24 https://t.co/2znmM7oqx3
https://t.co/XSdl6VJtkO
•by @IrenemGhobrial the Pangea 2.0 model for smoldering #myeloma risk stratification #ASH24 link to PANGEA 1.o https://t.co/UXwm59eFw5 /2
PANGEA demonstrated that a prospective, serial biomarker-guided strategy of adding targeted antibodies to optimally sequenced chemotherapy outperforms historical controls in advanced gastroesophageal adenocarcinoma. 1-year OS 66-69% with PTS versus ~50% historical (P<0.001), mOS 15.7 months, ORR 74% at 1L. 37% baseline PT/MT biomarker discordance highlights the need for metastatic biopsy. Success merited larger PANGEA-2 trial. Paradigm for future platform trials in GI oncology. Landscape has since evolved with approvals in HER2+ (T-DXd DESTINY-Gastric02), claudin 18.2 (zolbetuximab), and FGFR2b (bemarituzumab-FORTITUDE-101).
Median: 66 % 1-year OS (Cancer Discovery final) (Personalized Treatment Strategy (PTS)) vs. 50 % 1-year OS (Historical control). 1-year OS (Cancer Discovery 2021 final) rate: 66% (PTS) vs. 50% (historical control). 1L response rate rate: 74% (PTS). 1L disease control rate rate: 99% (PTS). Phase 2 platform trial (novel clinical expansion-platform type II design, survival primary endpoint). 80 patients enrolled (68 per-protocol ITT), 3 sites. Personalized Treatment Strategy: baseline biomarker profiling on primary + metastatic tumors + progression points (PD1, PD2), assigned antibody per prioritized algorithm (PTA). 1L FOLFOX + AN, 2L FOLFIRI + AN, 3L docetaxel + AN. 1L antibodies: HER2 amp → trastuzumab (n=16, 79% 1-yr OS); EGFR amp → ABT-806 (n=8, 75%); Immune (PDL1 CPS>10, MSI, TMB>15, EBV) → nivolumab (n=5, 75%); FGFR2 amp → none available (n=4, 50%); all-negative → ramucirumab (n=43, 75%). PT/MT discordance 37%. Met primary endpoint: 1-yr OS 69.4% (ASCO GI 2020) / 66% (Cancer Discovery final) vs. historical 50% (one-sided P<0.001 / P=0.0024). Median OS 15.7 months; median PFS 8.2 months.
Median OS 15.7 months (95% CI 13.8-20.8) per primary analysis; 1-year OS 69.4% ITT (P<0.001 vs historical 50%). Median PFS 8.2 months at 1L; ORR 74% 1L. These outcomes SUPERIOR to historical controls. Warranted larger PANGEA-2 platform. Supports biomarker-guided mAb sequencing over static 1L paradigm. Therapeutic resistance observed in correlative analyses suggests dual targeted inhibition may be beneficial.
Grade ≥3 adverse events: 32% (pts). Any Grade >3 toxicity through all 3 chemotherapy lines observed in 32% of patients. Safety profile consistent with sequenced chemo + targeted antibody combinations.
🔄 First successful biomarker-guided platform trial in GEA. PANGEA-2 larger Phase 3 warranted. PANGEA demonstrated that a prospective, serial biomarker-guided strategy of adding targeted antibodies to optimally sequenced chemotherapy outperforms historical controls in advanced gastroesophageal adenocarcinoma. 1-year OS 66-69% with PTS versus ~50% historical (P<0.001), mOS 15.7 months, ORR 74% at 1L. 37% baseline PT/MT biomarker discordance highlights the need for metastatic biopsy. Success merited larger PANGEA-2 trial. Paradigm for future platform trials in GI oncology. Landscape has since evolved with approvals in HER2+ (T-DXd DESTINY-Gastric02), claudin 18.2 (zolbetuximab), and FGFR2b (bemarituzumab-FORTITUDE-101).
PANGEA is an academic, investigator-initiated Phase 2 trial from the University of Chicago that tests a prospective, serial biomarker-guided personalized treatment strategy — adding targeted antibodies to optimally sequenced chemotherapy — in newly diagnosed advanced gastroesophageal adenocarcinoma (NCT02213289). PANGEA-2 is the larger follow-on platform trial.
No. PANGEA is an investigator-initiated academic strategy trial, not an FDA registration trial, and it did not lead to an FDA approval. It was designed to test whether a biomarker-guided sequencing strategy outperforms a static first-line paradigm.
The personalized, biomarker-guided treatment strategy achieved a median overall survival of 15.7 months (95% CI 13.8-20.8) and a 1-year overall survival of about 69% versus a historical control of 50% (p<0.001). The first-line objective response rate was 74%. These outcomes were superior to historical controls and supported the larger PANGEA-2 platform.
PANGEA was the first successful biomarker-guided platform trial in gastroesophageal adenocarcinoma, providing evidence that prospectively matching targeted antibodies to a tumor's evolving biomarkers across lines of therapy can outperform a fixed first-line regimen. It is hypothesis-supporting and motivated the larger PANGEA-2 platform.
PANGEA is an investigator-initiated program led by Daniel V.T. Catenacci and colleagues at the University of Chicago.
