Unresectable or recurrent grade 1/2 gastroenteropancreatic neuroendocrine tumors (GEP-NETs) with poor prognostic factors — Japan Clinical Oncology Group (JCOG) / National Cancer Center; funded by National Cancer Center Research and Development Fund + Japan Agency for Medical Research and Development (AMED)
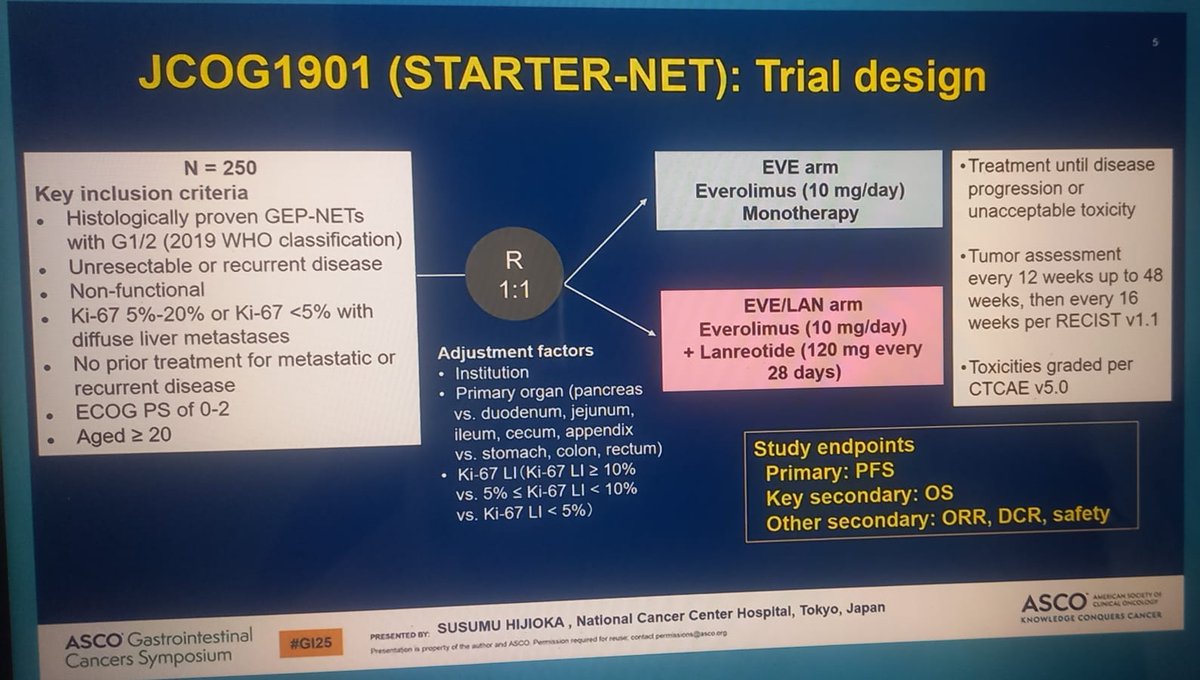
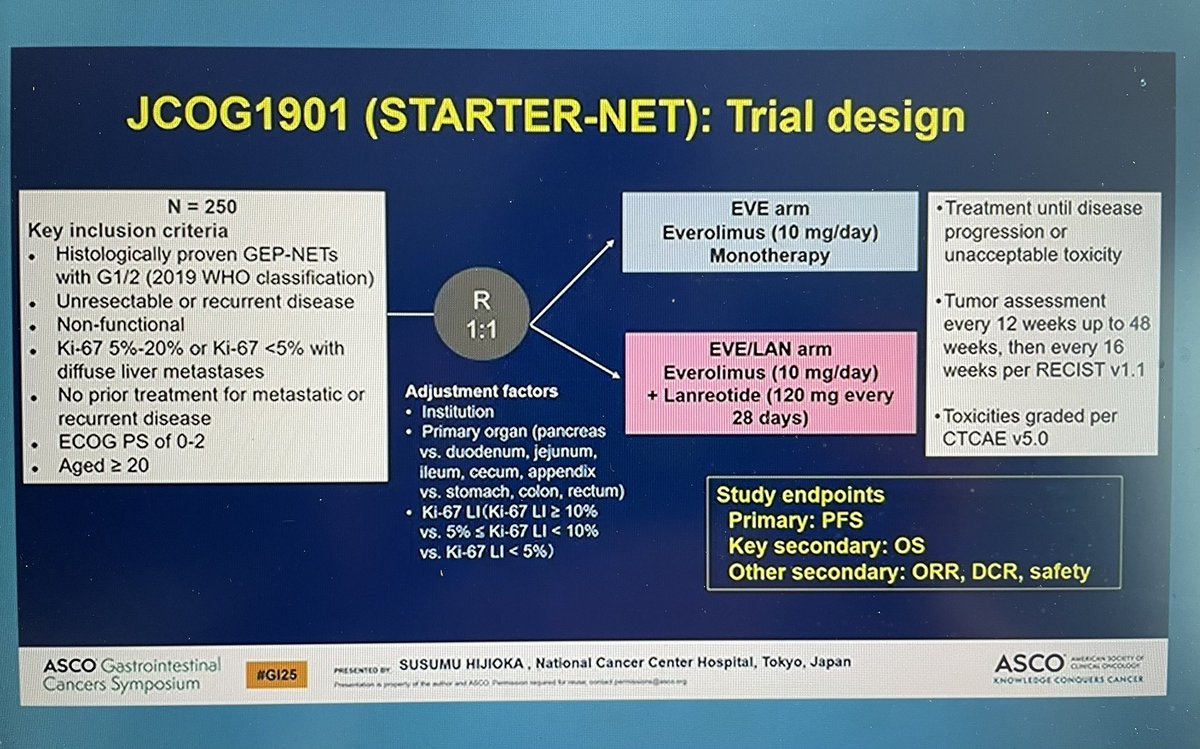
Discover KOL Sentiment on STARTER-NET →Design - Phase 3 randomized trial of everolimus (Afinitor) + lanreotide (Somatuline) vs everolimus alone in unresectable/recurrent grade 1/2 GEP-NETs with poor prognostic factors (JCOG1901; Japan Clinical Oncology Group / National Cancer Center).
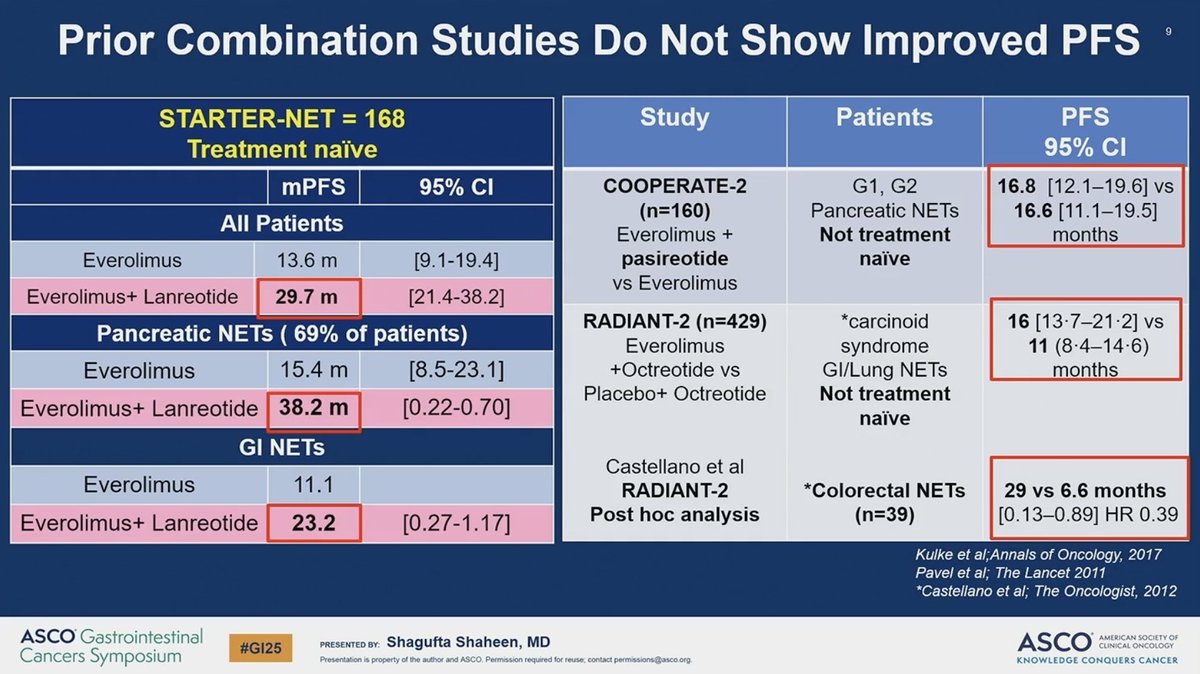
PFS (primary) - Median PFS 29.7 months (everolimus + lanreotide) vs 11.5 months (everolimus alone); stratified HR 0.38 (95% CI 0.15-0.96), P=0.00017 - more than a doubling of PFS; trial stopped early for efficacy.
Overall survival - Immature - median OS not reached in either arm; 1-year OS 96.2% vs 97.0%; OS HR 0.74 (95% CI 0.25-2.24, 13 events).
Response - Objective response rate approximately 23% (secondary endpoint).
Safety - Grade >=3 adverse events 35.6% (everolimus + lanreotide) vs 14.9% (everolimus alone); key events hyperglycemia, oral mucositis, fatigue and anorexia - consistent with the everolimus backbone.
Regulatory / sponsor - Investigational combination; everolimus and lanreotide each separately approved in GEP-NET. Sponsor JCOG/NCC Japan. ASCO GI 2025 (Abstract 652).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.









Top tweets by impressions — click to view on X
Good takeaways from Dr. Shaheen #GI25 https://t.co/qkB3lxb5Kp
✅First line treatment of GEP-NETs are evolving
➡️STARTER-NET trial shows PFS benefit of Everolimus Plus Lanreotide #GI25 @ASCO
Surveilance without teeatment?
SSA monotherapy?
Lutetium plus SSA?…
If you had "these are cross-trial comparisons, which we shouldn't do, but we do anyway!" on your bingo board, you win! #GI25 https://t.co/paUnOt5bEF
STARTER NET trial . Probably will not change the practice. Discussion is spot on @ASCO @OncoThor @5_utr #GI25 https://t.co/NAIEYukZKT
New research just presented at #GI25: STARTER-NET trial shows everolimus + lanreotide more than doubles PFS vs everolimus monotherapy among pts w/ aggressive GEP-NETs: https://t.co/LyF50SL8UI…
STARTER-NET rand PhIII of 1:1 everolimus + lanreotide vs evero alone in #1L G1/2 adv #GEP-NET ➡️ sig improved median PFS (29.7 mos vs 11.5 mos), higher ORR (23% vs 8.3%), more G3 tox w/combo. No sig…
Dr. Hijioka presents P3 JCOG1901, STARTER-NET: everolimus +/- lanreotide for unresectable/recurrent GEP NET. PFS 29.7 vs 11.5 months (HR 0.38). mOS not reached in either arm. #GI25…
Susumu Hijioka, MD, PhD, stopped in for an interview to discuss the phase 3 STARTER-NET study of everolimus plus lanreotide in gastroenteropancreatic neuroendocrine tumors. Stay tuned to…

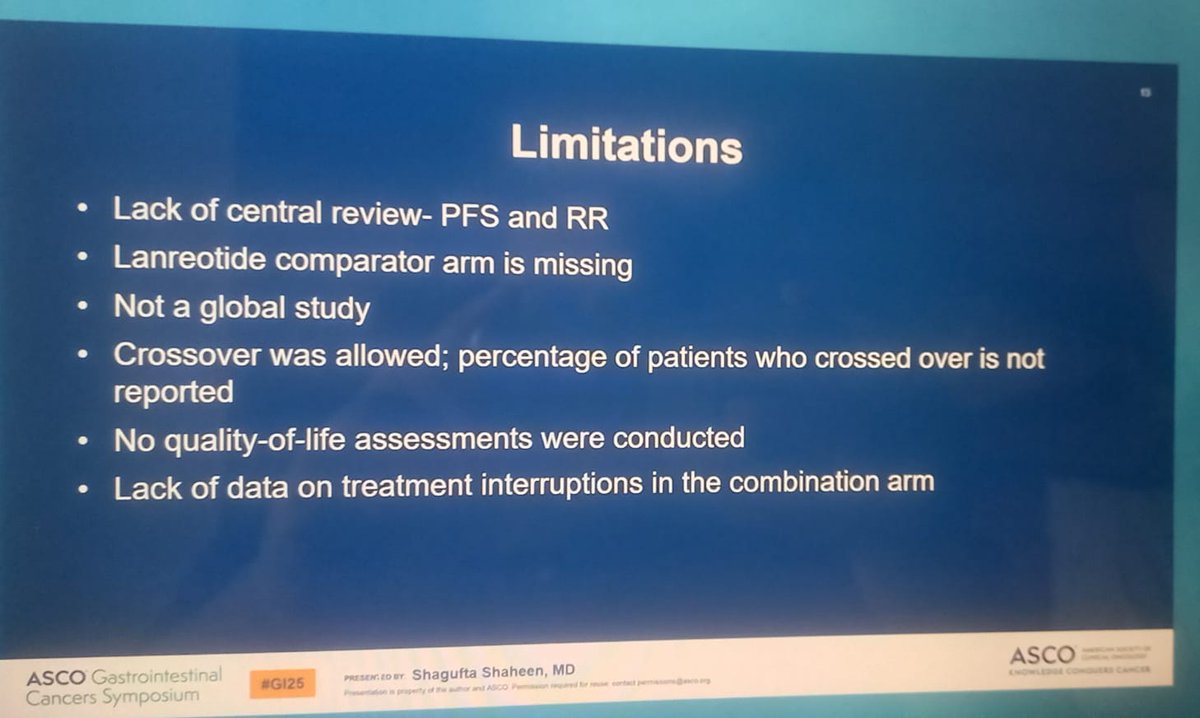
Agree, lack of 1L SSA -> 2L evero as a control arm may have been a missed opportunity here. #GI25 https://t.co/8CFmeWXpao

Elegant discussion of the STARTER NET trial by @SShaheenMD at #GI25 @ASCO . Unfortunately, despite positive results, this is not a practice-changing trial for most patients with WD GI-GEP-NETs.…
STARTER-NET (JCOG1901) is the first Phase 3 to demonstrate that adding lanreotide to everolimus more than DOUBLES PFS (29.7 vs. 11.5 months, HR 0.38, one-sided P=0.00017) in patients with unresectable or recurrent GEP-NETs and poor prognostic factors (Ki-67 5-20% or diffuse liver mets). Benefit is strongest in Ki-67 >10% subgroup (HR 0.32, 95% CI 0.15-0.69). Trial was terminated early for overwhelming efficacy. Establishes combination as potential new first-line SOC for this poor-prognosis subset. Open questions: PRRT (177Lu-DOTATATE) comparison, QoL impact of hyperglycemia/mucositis, immature OS.
Median: 29.7 months (everolimus + lanreotide) vs. 11.5 months (everolimus monotherapy). HR 0.38 (95% CI 0.15-0.96), P=0.00017 PFS: 29.7 mo (EVE+LAN) vs. 11.5 mo (EVE alone); stratified HR 0.38 (99.91% CI 0.15-0.96); one-sided P=0.00017. Phase 3 Japanese multicenter trial (N=178 enrolled of planned 250). Trial TERMINATED EARLY at planned interim analysis (June 2024) due to overwhelming efficacy. Interim analysis (n=145): median PFS 29.7 months (EVE+LAN) vs. 11.5 months (EVE); HR 0.38 (99.91% CI 0.15-0.96, P=0.00017 vs. prespecified 0.00046). Interim analysis (June 2024; presented ASCO GI 2025, Abstract 652): mPFS 29.7 vs. 11.5 months; stratified HR 0.38 (99.91% CI 0.15-0.96); one-sided P=0.00017. Trial stopped early for efficacy. Benefit consistent across subgroups: primary tumor site (pancreatic vs. GI), age, Ki-67 index. Greatest effect in Ki-67 >10% subgroup. Hijioka et al., JCO 43:652 (2025).
HR 0.74 (95% CI 0.25-2.24) OS immature. Median OS not reached in either arm. 1-year OS 96.2% (EVE+LAN) vs. 97.0% (EVE alone); OS HR 0.74 (95% CI 0.25-2.24, 13 events observed). Long-term OS maturation pending. Secondary endpoints: ORR 23.0% vs. 8.3% (P=0.011); DCR 92.0% vs. 84.5% (P=0.16).
Grade ≥3 adverse events: 35.6% (eve_lan) vs. 14.9% (eve). Key AEs: hyperglycemia (Grade ≥3: 9.1% EVE+LAN vs. 1.1% EVE), oral mucositis (Grade ≥3: 8.0% vs. 4.6%), fatigue (Grade ≥3: 5.7% vs. 1.1%), anorexia (Grade ≥3: EVE arm 3.4%), diarrhea (Grade ≥3: EVE arm 3.4%), pneumonitis (Grade ≥3: 3% vs. 1%). Combination associated with more adverse events: Grade ≥3 non-hematologic toxicity 35.6% (EVE+LAN) vs. 14.9% (EVE alone). Hyperglycemia particularly elevated (all-grade 62.1% vs. 33.3%). ILD occurred in 5% vs. 3%. No treatment-related deaths in either arm. Per discussant (Shagufta Shaheen, Stanford), tolerability + missing QoL data are considerations; toxicities deemed manageable by investigators.
✅ Practice-changing in Japan: everolimus + lanreotide more than doubles PFS vs. everolimus alone in poor-prognosis GEP-NETs. STARTER-NET (JCOG1901) is the first Phase 3 to demonstrate that adding lanreotide to everolimus more than DOUBLES PFS (29.7 vs. 11.5 months, HR 0.38, one-sided P=0.00017) in patients with unresectable or recurrent GEP-NETs and poor prognostic factors (Ki-67 5-20% or diffuse liver mets). Benefit is strongest in Ki-67 >10% subgroup (HR 0.32, 95% CI 0.15-0.69). Trial was terminated early for overwhelming efficacy. Establishes combination as potential new first-line SOC for this poor-prognosis subset. Open questions: PRRT (177Lu-DOTATATE) comparison, QoL impact of hyperglycemia/mucositis, immature OS.
STARTER-NET (JCOG1901) is a Phase 3 trial conducted by the Japan Clinical Oncology Group and the National Cancer Center, Japan. It compared everolimus (Afinitor) plus lanreotide (Somatuline) against everolimus alone in patients with unresectable or recurrent grade 1/2 gastroenteropancreatic neuroendocrine tumors (GEP-NETs) who had poor prognostic factors.
Adding lanreotide to everolimus more than doubled progression-free survival: median PFS was 29.7 months with the combination versus 11.5 months with everolimus alone (hazard ratio 0.38, P=0.00017), and the trial was stopped early for efficacy. Overall survival was immature with median not reached in either arm, and the objective response rate was approximately 23%.
Everolimus (Afinitor) and lanreotide (Somatuline) are each separately FDA-approved in gastroenteropancreatic neuroendocrine tumors, but the specific first-line combination regimen tested in STARTER-NET is investigational and not an FDA-approved regimen. STARTER-NET (JCOG1901) was conducted in Japan and its combination strategy is not an FDA approval.
Grade 3 or higher adverse events were more frequent with the combination (35.6%) than with everolimus alone (14.9%), driven by known everolimus toxicities such as hyperglycemia (grade >=3 9.1% vs 1.1%), oral mucositis, fatigue and anorexia. The added toxicity reflects the everolimus backbone rather than a new safety signal from lanreotide.
STARTER-NET is the first Phase 3 trial to show that adding a somatostatin analog (lanreotide) to everolimus more than doubles progression-free survival in poor-prognosis grade 1/2 GEP-NETs, and it is considered practice-changing in Japan. It provides high-level evidence for a combination approach in a setting where the optimal sequencing and combination of targeted and somatostatin-analog therapy has been debated.