Stage I-III TNBC or BRCA-mutated HR+/HER2- breast cancer with ctDNA-positive MRD after curative therapy — GSK
Discover KOL Sentiment on ZEST →Design - Phase 3 niraparib (Zejula, PARP inhibitor) vs placebo in ctDNA-positive molecular residual disease after curative-intent therapy, stage I-III TNBC or BRCA-mutated HR+/HER2- breast cancer (NCT04915755).
Outcome - TERMINATED EARLY - only 40 of 1,901 screened patients were ctDNA-positive and randomized; underpowered for meaningful efficacy assessment.
Efficacy (exploratory, underpowered) - Descriptive median recurrence-free interval 11.4 mo (niraparib) vs 5.4 mo (placebo); not a powered comparison.
OS - Not reported - trial terminated before any overall-survival analysis.
Regulatory - Investigational - niraparib is FDA approved in ovarian cancer; this ctDNA-guided breast maintenance use was not established (trial terminated).
Sponsor / drug - GSK; niraparib (Zejula).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.



















Top tweets by impressions — click to view on X
Presented at #SABCS24 results of the #ZEST trial assessing the impact of #ctDNA surveillance in patients with mostly triple-negative #BreastCancer and molecular residual disease after definitive…
ZEST—a ph3 trial for TNBC w/ ctDNA screening
🛑stopped early due to low randomization
🩻 50% with mets at time ctDNA+
⏲️ ctDNA+ occurred often on 1st test/
≤6 mos from EoT
▫️Recurrence-free interval…
Discussion of ZEST by Ian Krop stating that ctDNA isn't quite ready for prime time
@SABCSSanAntonio #SABCS24 @OncoAlert #bcsm https://t.co/ke9rtHSPRT
Emphasizes importance of designing MRD interception trials with early and frequent ctDNA testing especially in baseline high risk disease!
#bcsm #SABCS24 https://t.co/6NutGXpH7U
#SABCS24 ZEST results w/ 88% TN. 8% who entered surveillance were ctDNA positive, only 4 recurred. 40 rand to nirapirib vs placebo, 15% mutant. 60% TNBC + w/in 6 mo of end of Rx. Fast rise in ctDNA…
Dr. Turner presents #ZEST adj study of MRD in pts with HR + w/ BRCA & TNBC all comers w/ niraparib as intervention
147 had ctDNA+, only 40 randomized
Rad recurrence assoc w/ ⬆️ ctDNA level…

Takeaways from ZEST
📌short lead time between det of ctDNA and recurrence ~5mos
📌Pts who had ➖ ctDNA conv to➕within 3mos with MBC on imaging.
📌 pts with ctDNA have💯recurrence
📌 no data yet that…
ZEST: MRD guided tx
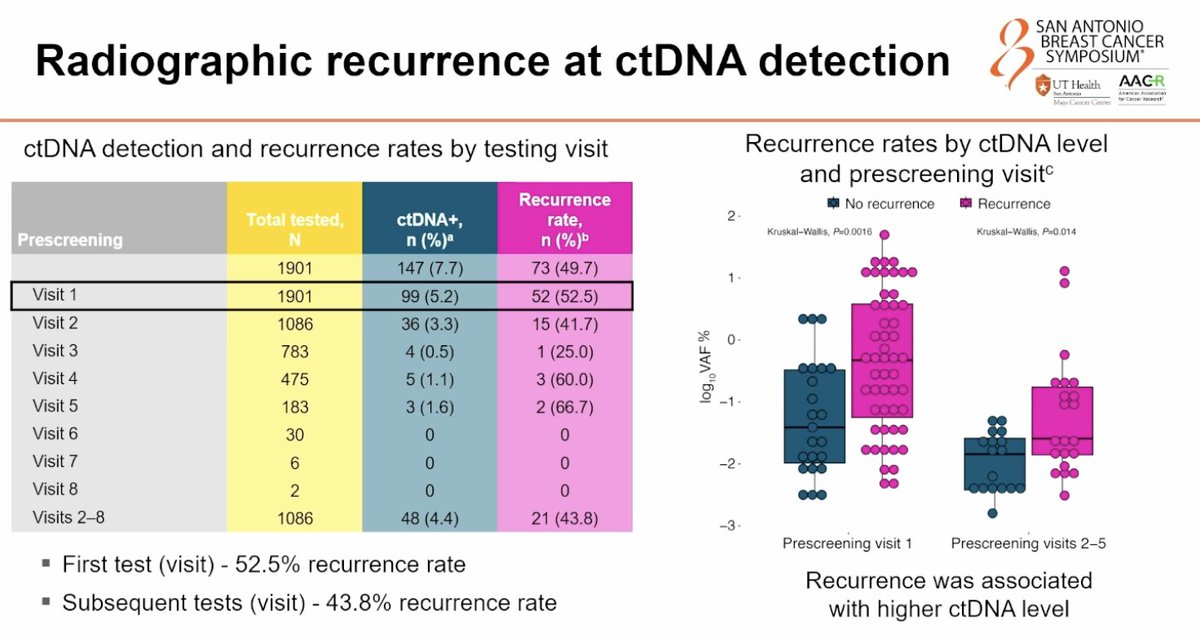
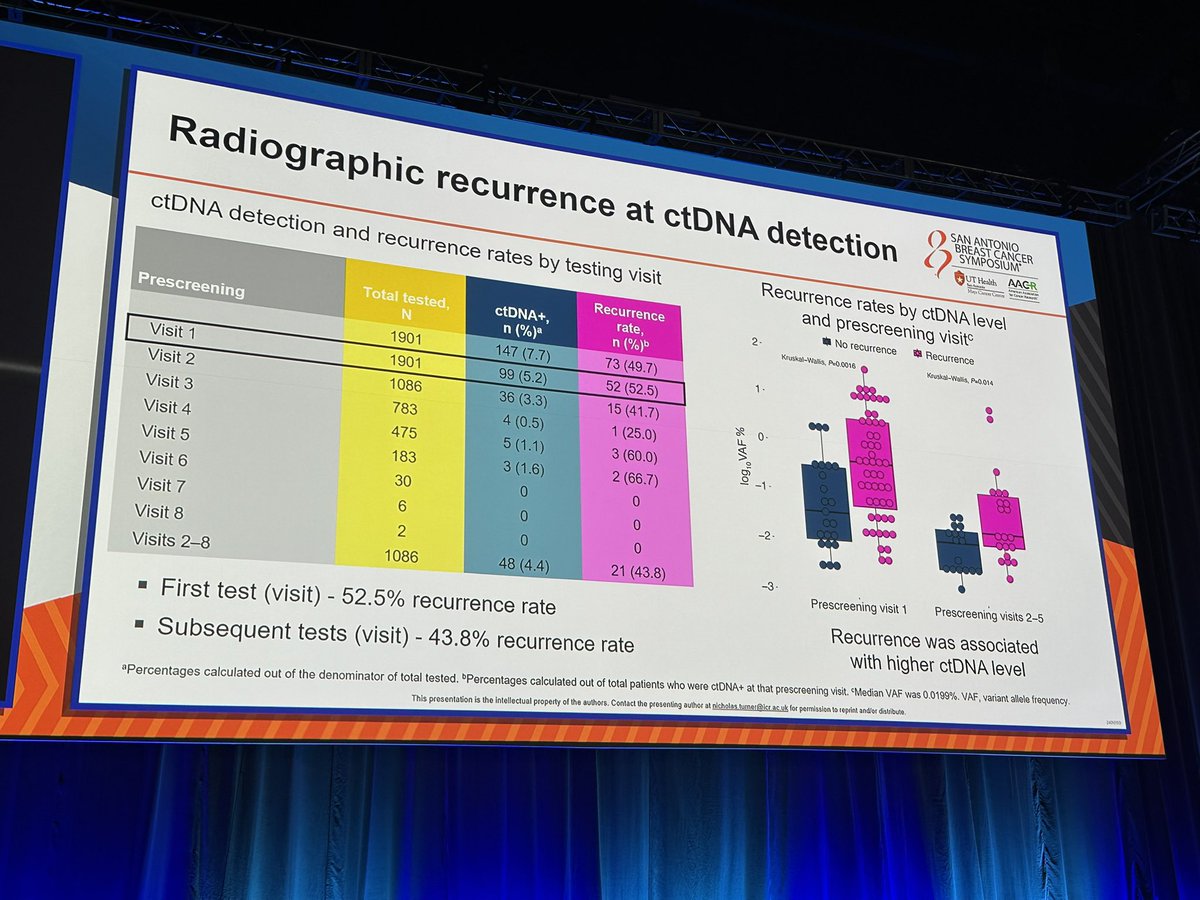
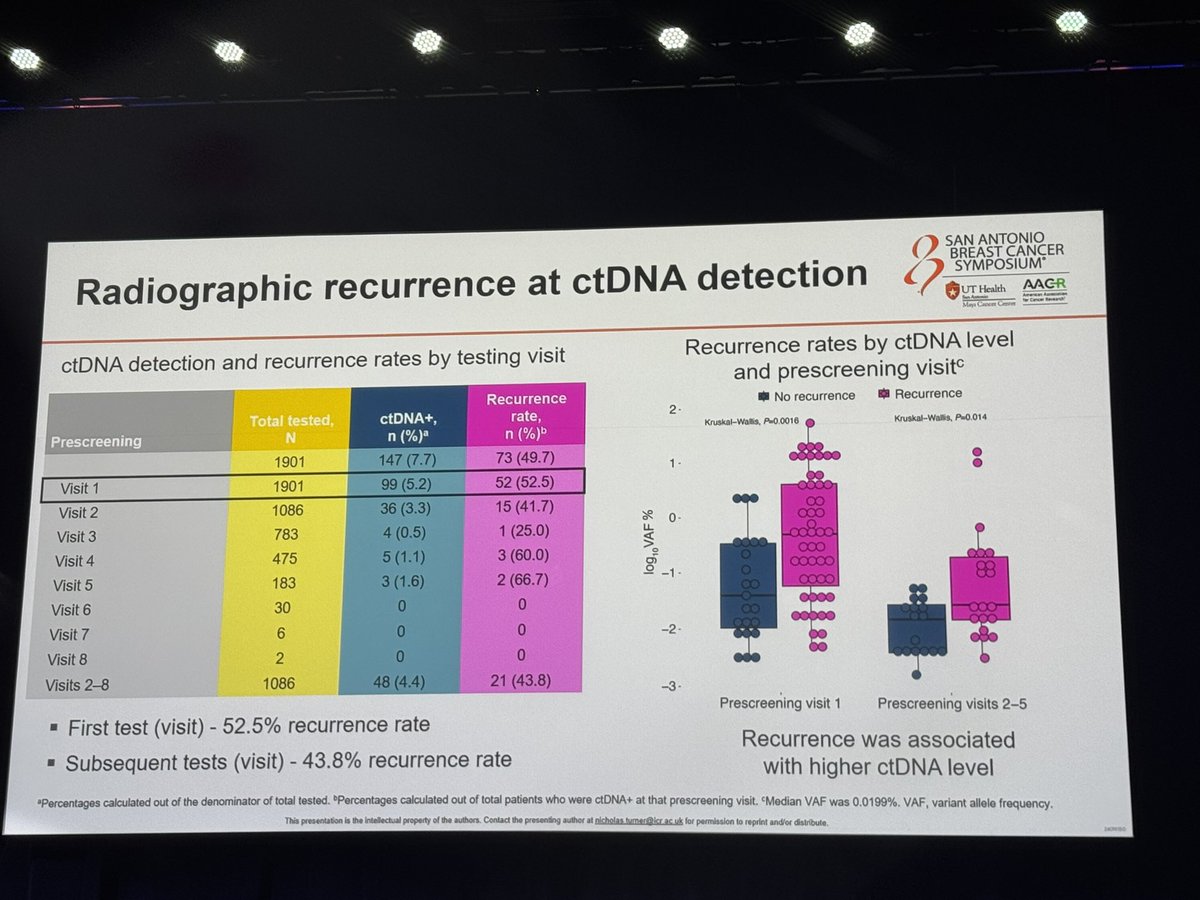
n=1901 surveillance (88% TNBC), 147 (8% ctDNA+, highest w/i first 3 mo; 60% w/i 6mo)
ctDNA+: 50% radiologic recurrence, subsequent test 43.8% recurrence
40 pts randomized: HR…
#SABCS24 Ian Krop discusses Zest. As an investigator & provider, frustrated by low ctDNA+ rates, Mets at 1st detection in TNBC. Longer lead time for HR+. My take: we need to direct Rx B4 surgery…
My takeaways- MRD intervention remains hard.
Low yield ⚠️
High metastatic disease rates at ctDNA detection ⚠️
#SABCS24
@OncoAlert
@SABCSSanAntonio
ZEST is a cautionary tale in MRD-guided therapy trial design. Only 7.7% of screened patients were ctDNA-positive after completing curative-intent therapy, and 55% of those already had imaging-detectable disease — meaning ctDNA testing post-treatment was too late. Turner et al. recommend future MRD trials test during neoadjuvant therapy and target higher-risk subsets (stage 2B+ non-pCR). ctDNA assay was personalized tumor-informed test (16 tumor-specific mutations per patient).
Median: 11.4 months (niraparib) vs. 5.4 months (placebo). Trial terminated early due to low ctDNA-positive enrollment. Only 40 of 1,901 screened patients were randomized — insufficient for meaningful efficacy assessment. Descriptive median recurrence-free interval 11.4 months (niraparib) vs. 5.4 months (placebo). 6 niraparib vs. 4 placebo patients remained recurrence-free at data cutoff. HR, CI, and P-value NOT in published sources (underpowered). Turner et al. emphasized that 55% of ctDNA-positive patients already had imaging-detectable recurrence at first positive test — a critical design lesson.
Grade ≥3 TRAE rates NOT in published sources for this terminated trial. Niraparib safety profile well-established from OlympiA/OVA trials — hematologic toxicities (anemia, thrombocytopenia, neutropenia) are class effects.
❌ Negative trial: terminated early for low enrollment; no practice-changing efficacy signal. ZEST is a cautionary tale in MRD-guided therapy trial design. Only 7.7% of screened patients were ctDNA-positive after completing curative-intent therapy, and 55% of those already had imaging-detectable disease — meaning ctDNA testing post-treatment was too late. Turner et al. recommend future MRD trials test during neoadjuvant therapy and target higher-risk subsets (stage 2B+ non-pCR). ctDNA assay was personalized tumor-informed test (16 tumor-specific mutations per patient).
ZEST is a Phase 3 randomized trial (NCT04915755) that tested niraparib (Zejula, a PARP inhibitor) versus placebo in patients with stage I-III triple-negative or BRCA-mutated HR-positive/HER2-negative breast cancer who became ctDNA-positive - indicating molecular residual disease - after completing curative-intent therapy. The goal was to see whether starting therapy at molecular relapse could prevent overt recurrence.
ZEST was terminated early because of low ctDNA-positive enrollment. Only about 7.7% of screened patients were ctDNA-positive after curative-intent therapy, and roughly 55% of those already had overt imaging recurrence, so only 40 of 1,901 screened patients were randomized - far too few for a meaningful efficacy assessment.
Because it was terminated early and underpowered, ZEST provides no practice-changing efficacy signal. An exploratory, descriptive median recurrence-free interval was 11.4 months with niraparib versus 5.4 months with placebo, but this was not a powered comparison. Overall survival was not reported, as the trial ended before any survival analysis.
No. Niraparib (Zejula) is FDA approved in ovarian cancer, but the ctDNA-guided molecular-residual-disease maintenance strategy in breast cancer that ZEST evaluated is investigational and was not established, because the trial was terminated early for low enrollment.
ZEST is a cautionary tale in the design of MRD-guided therapy trials: screening enough patients to find and randomize a ctDNA-positive population before overt recurrence is operationally very difficult. Its enrollment experience informs how future ctDNA-triggered interception trials set eligibility windows, screening cadence, and sample-size assumptions.