Phase 3 Alliance trial (A021502) testing adjuvant atezolizumab + mFOLFOX6 vs mFOLFOX6 alone in resected stage III dMMR/MSI-H colon cancer. 3-year DFS 86.3% vs 76.2% (HR 0.50, NEJM 2026). NCCN Category 2A preferred; FDA sBLA under Priority Review (PDUFA Oct 9, 2026) - not yet approved. NCI/Alliance for Clinical Trials in Oncology, with Genentech/Roche (atezolizumab/Tecentriq).
Stage III dMMR/MSI-H Colon Cancer (Adjuvant)Atezolizumab (Tecentriq) + mFOLFOX6ASCO 2025 Plenary (#ASCO25, LBA1)ESMO GI 2026 Update (#ESMOGI26)⚠ Investigational - FDA Priority Review (PDUFA Oct 9, 2026)
Design: Phase 3 Alliance/NCTN trial (A021502 / AIO-KRK-0317), 712 patients, resected stage III colon cancer with dMMR/MSI-H, randomized 1:1 to mFOLFOX6 + atezolizumab (12 months total therapy) vs mFOLFOX6 alone (6 months).
DFS (primary endpoint): 86.3% vs 76.2% at 3 years - HR 0.50 (95% CI 0.35-0.73), P<0.001 (NEJM, 2026).
OS (secondary endpoint): Immature - 5-year OS 89.7% vs 87.9%, HR 0.90 (0.55-1.47), not statistically significant (NEJM update, 45.8-month follow-up).
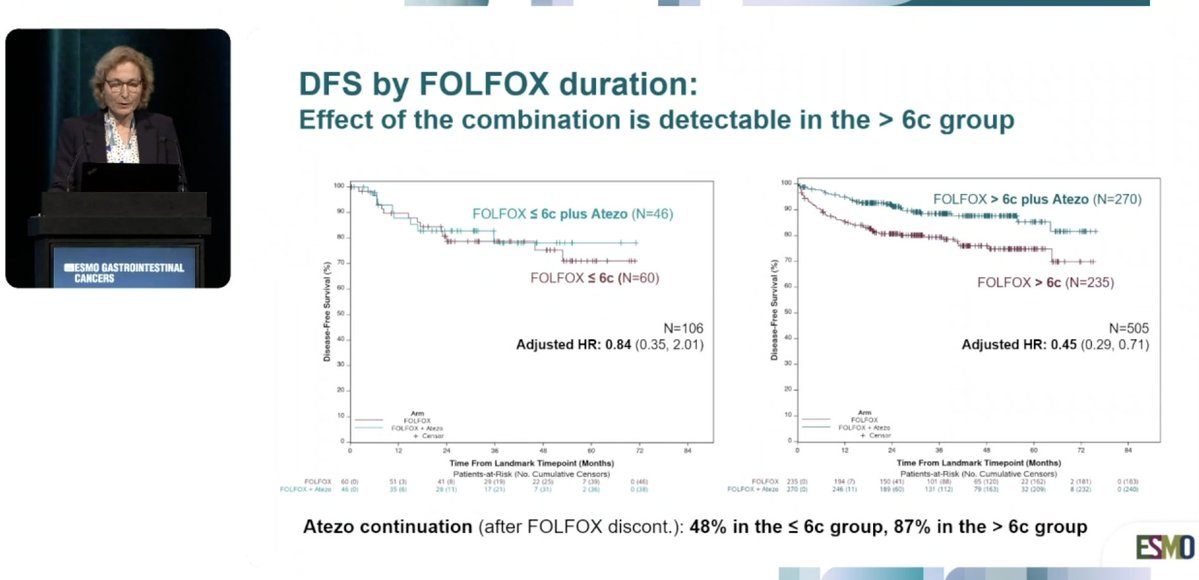
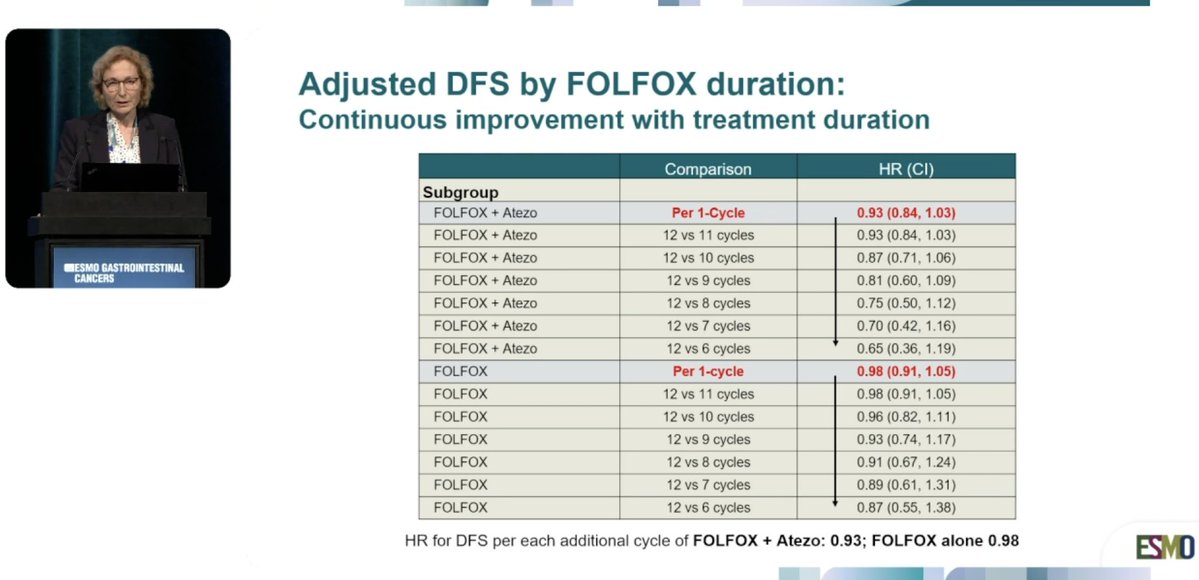
Duration analysis (exploratory, ESMO GI 2026): Atezolizumab benefit concentrated in patients completing >6 cycles of FOLFOX (HR 0.41) vs little benefit at ≤6 cycles (HR 0.97).
Regulatory: Investigational - FDA accepted an sBLA and granted Priority Review (June 2026); PDUFA target action date October 9, 2026. Not yet approved.
NCCN: FOLFOX/CAPOX + atezolizumab added as a Category 2A preferred regimen for stage III dMMR/MSI-H colon cancer (2025 update).
Sponsor/drug: NCI / Alliance for Clinical Trials in Oncology, with Genentech, a member of the Roche Group (atezolizumab/Tecentriq). Presenter/PI: Frank A. Sinicrope, MD (Mayo Clinic).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 5, 2026.
Free Access · KOL Pulse Intelligence
Track oncology’s top KOLs in your specialty
Create a free account, pick the tumor types you cover, and go beyond the tweet — the intelligence pharma teams use to map influence and prepare for engagement:
Choose the tumor types you follow. No cost, unsubscribe anytime.
Influence Leaders
Top KOLs Discussing ATOMIC
Frank Sinicrope, MD — Presenter/PI
@FASinicropeMD
24.9K impressions
Dr Amol Akhade
@SuyogCancer
41.6K impressions
Toni Choueiri, MD
@DrChoueiri
22.0K impressions
Sharlene Gill, MD, MPH, MBA, FASCO
@GillSharlene
12.2K impressions
Bishal Gyawali, MD, PhD, FASCO
@oncology_bg
11.6K impressions
Dr Joseph McCollom DO
@realbowtiedoc
6.9K impressions
Conference Presentations
ATOMIC Key Slides & Visuals
Official ATOMIC trial slides shared by KOLs at ASCO 2025 (#ASCO25) - study design, safety, discussant commentary, and conclusions. Click any image to expand.
[Slide 1]
14
Safety Summary
Characteristics
mFOLFOX6 + Atezo
mFOLFOX6
(N=346)
(N=334)
Any Grade AE, % (n)
100% (346)
95.1% (329)
Treatment-related
99.7% (345)
94.2% (326)
Grade 3-4 AE, % (n)
83.8% (290)
69.1% (239)
Treatment-related
72.3% (250)
59.2% (205)
Grade 5 AE, % (n)
1.7% (6)
0.6% (2)
Treatment-related
0.6% (2)*
0.0% (0)
Investigator attribution of treatment-related adverse events (AE)
# Received at least one dose of treatment
"1 sudden death NOS (possibly related): 1 sepsis (possibly related)
2025
ASCO
#ASCO25
PRESENTED BY Frank A Sinicrope M.D.
ASCO
ANNUAL MEETING
KNOWLEDGE CONQUERS CANCER
---
[Slide 2]
Study Design
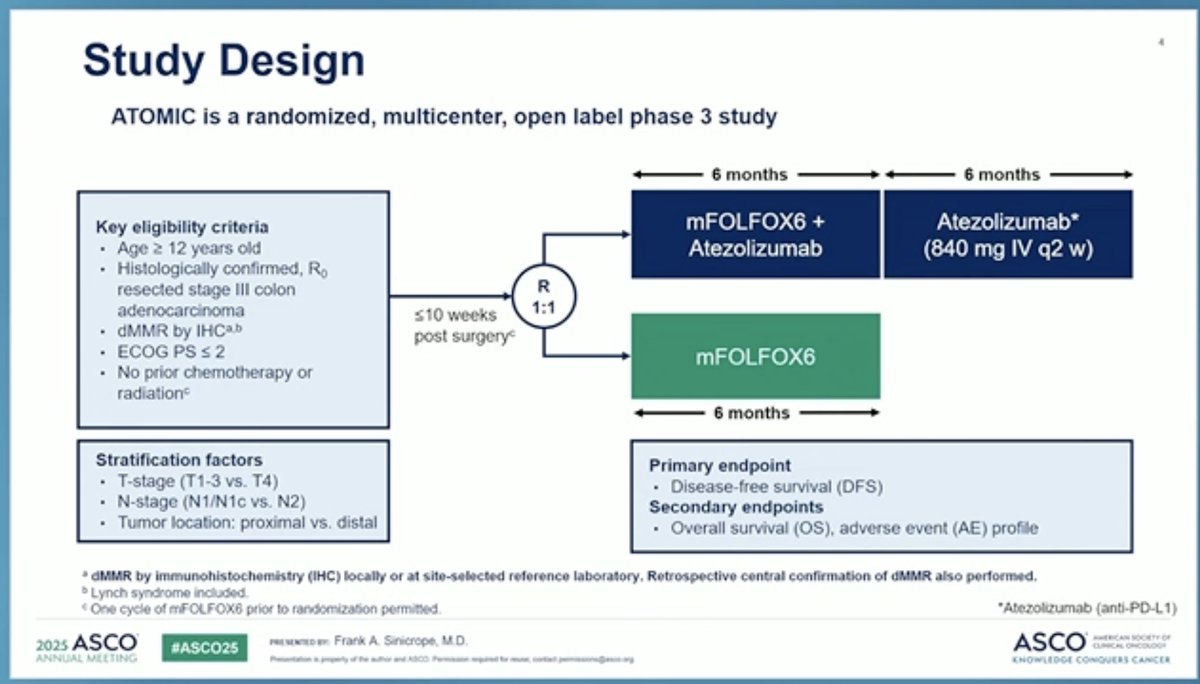
ATOMIC is a randomized, multicenter, open label phase 3 study
6 months
6 months
Key eligibility criteria
mFOLFOX6 +
Atezolizumab*
Age 2 12 years old
Atezolizumab
(840 mg IV q2 w)
Histologically confirmed, Ro
resected stage III colon
R
adenocarcinoma
s10 weeks
1:1
dMMR by IHCa.b
post surgery
ECOG PS s 2
mFOLFOX6
No prior chemotherapy or
radiation
6 months
Stratification factors
Primary endpoint
T-stage (T1-3 vs. T4)
Disease-free survival (DFS)
N-stage (N1/N1c vs. N2)
Secondary endpoints
Tumor location: proximal vs. distal
Overall survival (OS), adverse event (AE) profile
a
dMMR by immunohistochemistry (IHC) locally or at site-selected reference laboratory. Retrospective central confirmation of dMMR also performed
b Lynch syndrome included
< One cycle of mFOLFOX6 prior to randomization permitted
*Atezolizumab (anti-PD-L1)
2025 ASCO
#ASCO25
PRESENTED BY
Frank A Sinicrope M.D.
ASCO
ANNUAL MEETING
[Slide 1]
Key Takeaways
Adjuvant folfox + atezolizumab leads to a 10% absolute improvement in 3-year
2025
ASCO
DFS in stage 3 dMMR colon cancers
ANNUAL MEETING
An option to consider for resected dMMR colon cancers
Neoadjuvant immunotherapy is more effective and allows for de-escalation of
chemotherapy and surgery
MMR deficiency is amongst the best predictive biomarkers for immunotherapy
efficacy
urgent need for biomarkers to avoid overtreatment: who needs (neo)adjuvant
treatment?
2025
ASCO
PRESENTED BY Myrian Chalabi MO. PhD
ASCO
AMERICAN
#ASCO25
CLINICAL
ANNUAL MEETING
Passportation
KNOWLEDGE CONQUERS CANCER
---
[Slide 2]
Chemotherapy has very limited efficacy in dMMR colon cancers
Efficacy of adjuvant atezolizumab alone unknown after ATOMIC
Could chemo blunt the T-cell response?
2025 ASCO
ANNUAL MEETING
Neoadjuvant immunotherapy is extremely effective, without
chemotherapy, with limited toxicity
Study Schema
FOLFOX cycle
Arm3
FOLFOX steasAzumab
KE month then
Randomization (1:1)
altne
Surgery to
Assessment of
confirm
Institution factors:
KS month
HMR status by
stage II
IHCS
colon cancer
Arm
FOLFOX month
up to 10 works
at
laboratory
The missing Arm 3
Atezolizumab alone
2025
ASCO
#ASCO25
ESENTED BY Myriam Chalabi MD PhD
ASCO
AMERICAN
CLANKA
KNOWLEDGE CONQUERS CANCER
2025
ASCO
ANNUAL MEETING
---
[Slide 3]
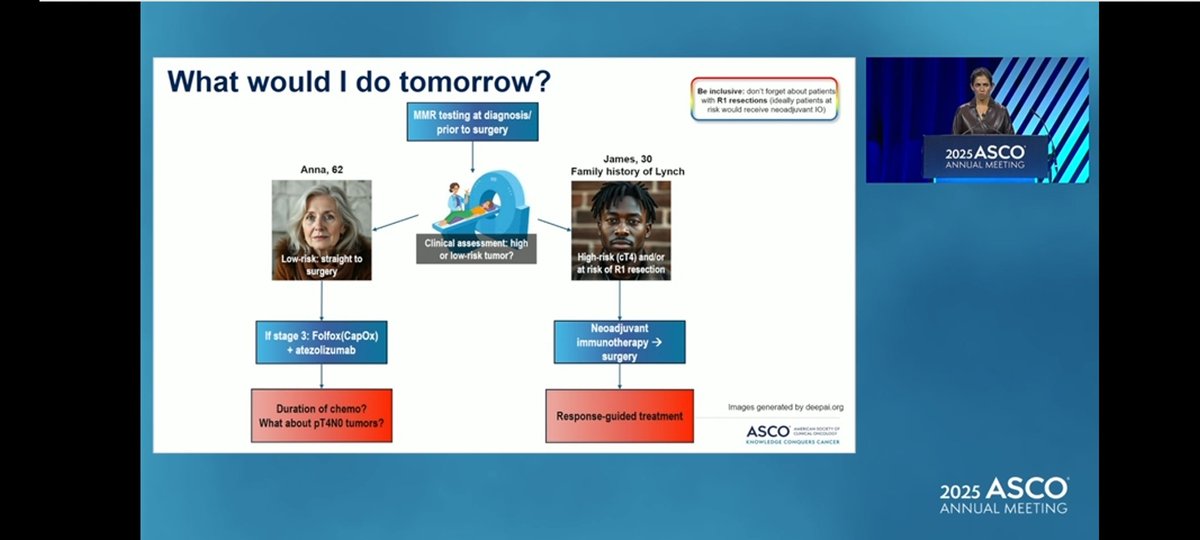
What would | do tomorrow?
Be inclusive don't forget about patients
with R1 resections (ideally patients at
MMR testing at diagnosis/
risk would receive neoadjuvant IO)
prior to surgery
James, 30
2025 ASCO
Anna, 62
ANNUAL MEETING
Family history of Lynch
Clinical assessment: high
Low-risk straight to
or low-risk tumor?
High-risk (cT4) and/or
surgery
at risk of R1 resection
Neoadjuvant
If stage 3: Folfox(CapOx)
immunotherapy ->
+ atezolizumab
surgery
Duration of chemo?
Images generated by deepai.org
What about pT4N0 tumors?
Response-guided treatment
ASCO
KNOWLEDGE CONQUIRES CANCER
2025
ASCO
ANNUAL MEETING
[Slide 1]
Study Details
First patient enrolled in October 2017. Closed to accrual January 2023
Study randomized 712 patients
At 2nd interim analysis, the stratified log-rank test for comparing DFS
between arms crossed the protocol-specified interim boundary of 0.009 for
efficacy, and the DSMB released the data
At data cutoff (Feb 4, 2025), median follow-up was 37.2 months (Q1, Q3:
24.2, 55.7)
2025 ASCO
#ASCO25
PRESENTED IN Frank A Sinicrope M.D.
ASCO
AMERICA SOCIETY
CURRENC ONCOUNCIA
ANNUAL MELTING
Reservation importly ACCO
KNOWLEDGE CONQUERS CANCER
[Slide 1]
Conclusions
mFOLFOX6 + Atezolizumab demonstrated a statistically significant and clinically
meaningful 50% risk reduction in recurrence or death over mFOLFOX6 alone
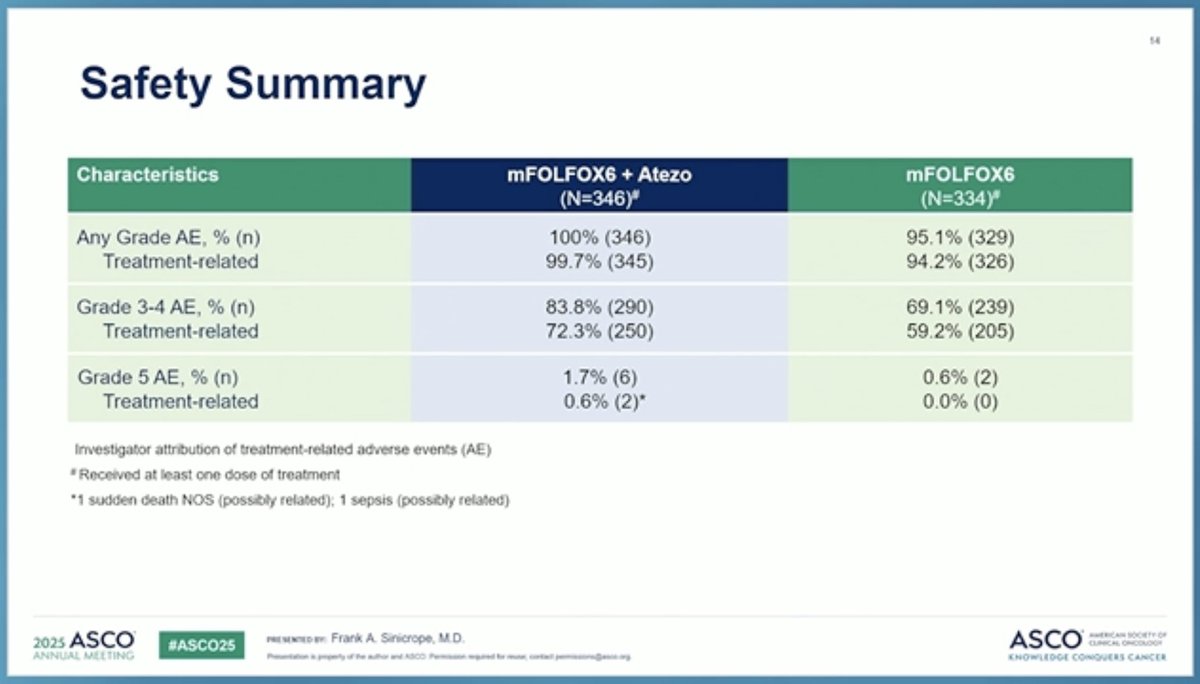
The safety of mFOLFOX6 + Atezolizumab was in line with the known safety
profiles of each, with a manageable increase in non-febrile neutropenia
Atezolizumab plus mFOLFOX6 is a practice changing and new standard treatment
for patients with dMMR stage III colon cancer
ASCO
AMERICAN
PRESENTED BY: Frank A. Sinicrope, M.D.
CLINICAL or
2025 ASCO
#ASCO25
KNOWLEDGE CONQUERS
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse; contact permissions@asco.org
---
[Slide 2]
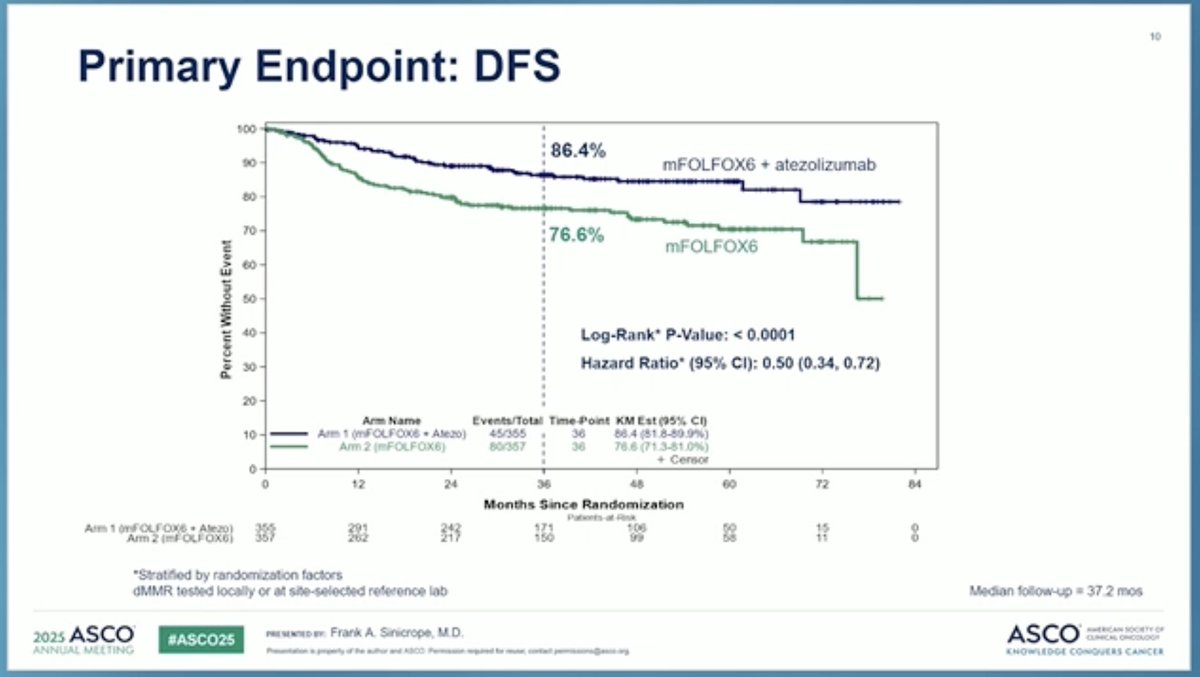
Primary endpoint: 3-year DFS
100
10% improvement in 3-year DFS: statistically
90
significant and clinically meaningful
80
70
13% recurrences despite 6 months of folfox +
60
Log-Rank* P-Value: < 0.0001
1 year atezo
50
Hazard Ratio* (95% CI): 0.50 (0.34, 0.72)
40
77% of patients are disease-free at 3 years
30
without atezolizumab
20
Arm Name
Events/Total Time-Point KM Est (95% CI)
10
Arm 1 (FOLFOX + Atezo)
45/355
36
86.4 (81.8-89.9%)
Arm 2 (FOLFOX)
80/357
36
76.6 (71.3-81.0%)
+ Censor
How many, and which, patients are cured with
0
0
12
24
36
48
60
72
84
surgery alone?
Months Since Randomization
Patients-at-Risk
FOLFOX Atezo)
355
291
242
171
106
50
15
Arm 2 (FOLFOX)
357
262
217
150
99
58
11
00
ASCO
#ASCO25
PRESENTED BY: Myriam Chalabi, MD, PhD
ASCO
AMERICAN SOCIETY OF
CLINICAL ONCOLOGY
JAL MEETING
Presentation is property of the author and ASCO Permission required for reuse contact permissions@asco.org
KNOWLEDGE CONQUERS CANCER
[Slide 1]
Open Questions on dMMR Colon Cancers
Who needs treatment? (prognostic and predictive biomarkers)
Can adjuvant immunotherapy cure more patients with dMMR colon
cancers?
In the era of immunotherapy: do patients with dMMR colon cancers
need adjuvant chemotherapy?
Is neoadjuvant immunotherapy better than adjuvant chemotherapy in
dMMR colon cancers?
2025 ASCO
#ASCO25
ASCO
AMERICAN SOCIETY OF
PRESENTED BY: Myriam Chalabi, MD. PhD
CLINICAL ONCOLOGY
ANNUAL MEETING
Presentation is property of the author and ASCO Permission required for reuse contact permissions@asco. org
KNOWLEDGE CONQUERS CANCER
[Slide 1 - Baseline characteristics]
FOLFOX duration analysis: Baseline characteristics.
Groups: FOLFOX+Atezo ≤6c (N=46), FOLFOX+Atezo >6c (N=270), FOLFOX ≤6c (N=60), FOLFOX >6c (N=235), Total (N=611).
No significant differences noted between groups (sex, nodal status, T-stage, risk group all balanced).
[Slide 2 - Conclusions/Takeaways]
Conclusions / Take aways. In this retrospective, exploratory analysis:
FOLFOX duration: >6 cycles of FOLFOX showed a DFS benefit when combined with Atezo (but not with ≤6 FOLFOX cycles).
Association per cycle: DFS benefit of Atezo plus FOLFOX increased continuously with an increasing number of FOLFOX cycles.
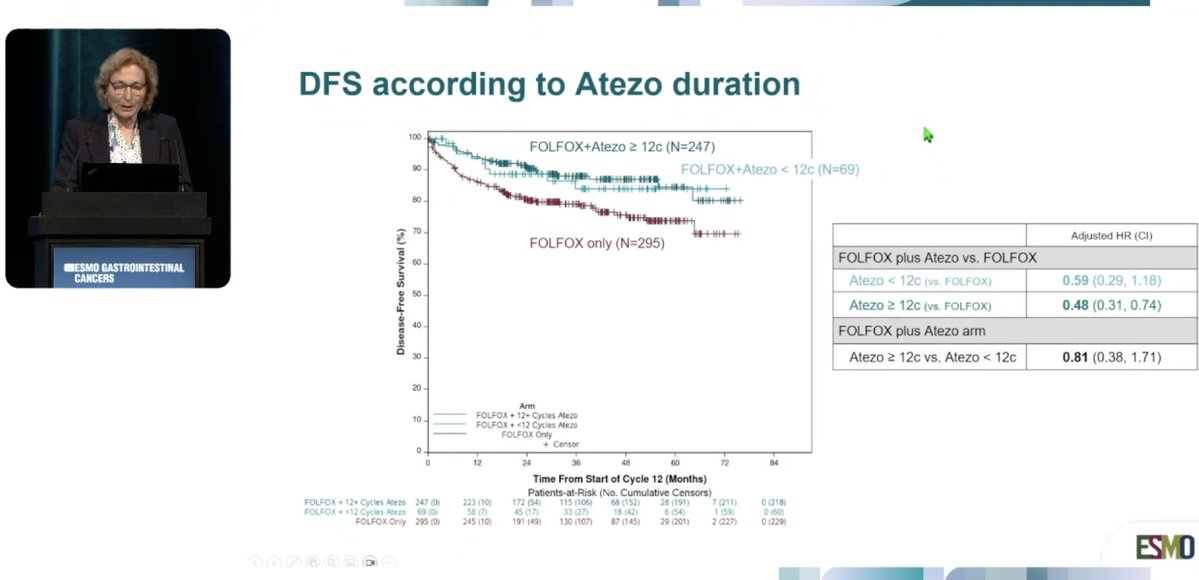
Atezo duration: A numerical DFS benefit was seen in patients receiving ≥12 cycles of Atezo (vs. fewer cycles).
ATOMIC (Alliance A021502, also known by its German co-sponsor designation AIO-KRK-0317) is a Phase 3, randomized, open-label, multicenter trial run through the NCI-funded Alliance for Clinical Trials in Oncology and National Clinical Trials Network, in partnership with Genentech, a member of the Roche Group, and the German AIO group. The trial enrolled 712 patients with completely resected stage III colon adenocarcinoma and deficient mismatch repair (dMMR) or microsatellite instability-high (MSI-H) status between September 2017 and January 2023 across more than 300 US and 9 German sites. Patients were randomized 1:1 to mFOLFOX6 plus atezolizumab (840 mg IV every 2 weeks for 12 cycles, followed by atezolizumab monotherapy for 13 additional cycles - 12 months of atezolizumab total) versus mFOLFOX6 alone (12 cycles, 6 months). ATOMIC is the first phase 3 trial to demonstrate benefit from adding an immune checkpoint inhibitor to adjuvant chemotherapy in resectable (non-metastatic) colon cancer - checkpoint inhibitors were previously approved only in the metastatic dMMR/MSI-H colorectal cancer setting.
EXPLORATORY ANALYSIS Duration of Chemotherapy & Atezolizumab Benefit
At ESMO GI 2026 (#ESMOGI26, Munich, Jul 1-4 2026), Dr. Frank Sinicrope presented a new exploratory analysis asking a pointed question: how much chemotherapy do patients receiving adjuvant atezolizumab actually need? The finding was surprising - the disease-free survival benefit of atezolizumab was concentrated in patients who completed more than 6 cycles of mFOLFOX6 (HR 0.41, 95% CI 0.27-0.64) versus little apparent benefit in patients who received 6 cycles or fewer (HR 0.97, 95% CI 0.44-2.11). As Dr. Arndt Vogel summarized: the benefit of atezolizumab appeared to increase with longer chemotherapy exposure - the opposite of what a toxicity-minimizing de-escalation strategy would hope to find. This creates real clinical tension between minimizing chemotherapy-related toxicity (Grade 3-4 AEs were already higher in the combination arm) and preserving the immunotherapy benefit that this analysis suggests depends on adequate chemotherapy exposure.
Important caveat: this is an exploratory, hypothesis-generating subgroup analysis - not a pre-specified primary or secondary endpoint. It should not be used alone to guide individual treatment-duration decisions; Dr. Sinicrope noted "more to come" on this question.
INVESTIGATIONAL FDA Priority Review Pending - Not Yet Approved
On June 10-11, 2026, the FDA accepted Genentech/Roche's supplemental Biologics License Application (sBLA) for adjuvant Tecentriq® (atezolizumab) and Tecentriq Hybreza® (atezolizumab and hyaluronidase-tqjs) plus chemotherapy in stage III dMMR/MSI-H colon cancer, and granted Priority Review. The FDA's target action (PDUFA) date is October 9, 2026. As of today, no approval has been granted for this indication - atezolizumab already carries broad FDA approvals in other cancers (e.g., NSCLC, hepatocellular carcinoma, melanoma), but the adjuvant colon cancer indication specifically remains under review. "This filing acceptance brings us closer to establishing adjuvant atezolizumab plus chemotherapy as a new standard of care for certain types of early colon cancer," said Levi Garraway, MD, PhD, Roche's Chief Medical Officer and Head of Global Product Development.
NCCN Guidelines: Ahead of any FDA decision, the NCCN Colon Cancer Guidelines Panel already added FOLFOX (or CAPOX) plus atezolizumab as a Category 2A preferred regimen for adjuvant treatment of both low-risk and high-risk stage III dMMR/MSI-H colon cancer (added 2025, reflected in Version 1.2026/2.2026) - and extended the recommendation to stage II T4bN0 dMMR colon cancer as well. Capecitabine/5-FU monotherapy was downgraded from Category 2A to 2B for this population in the same update.
Patients aged 12 years or older with completely resected stage III colon adenocarcinoma and deficient mismatch repair (dMMR) by immunohistochemistry (locally or centrally confirmed); Lynch syndrome patients were eligible. No prior chemotherapy or radiation, except up to one cycle of mFOLFOX6 while awaiting MMR results. 712 patients (355 atezolizumab arm / 357 control arm) were enrolled September 2017-January 2023 across 303 US NCTN sites plus 9 German AIO sites; 53.9% had high-risk tumors (T4, N2, or both).
712 patients · stage III dMMR/MSI-H colon cancer · 303 US + 9 German sites (NEJM, primary)
Experimental: mFOLFOX6 + atezolizumab 840 mg IV every 2 weeks for 12 cycles (6 months), followed by atezolizumab monotherapy for 13 additional cycles (total 12 months of atezolizumab). Control: mFOLFOX6 alone for 12 cycles (6 months). Primary endpoint: disease-free survival (DFS). Secondary endpoints: overall survival (OS) and adverse-event profile.
12 months total atezolizumab (concurrent + maintenance) vs 6 months chemotherapy alone (NEJM)
Disease-Free Survival (DFS) - Primary Endpoint - MET
At a median follow-up of 40.9 months, 127 DFS events had occurred (46 in the atezolizumab arm, 81 in the control arm). 3-year DFS was 86.3% (95% CI 81.8-89.8) with atezolizumab plus mFOLFOX6 vs 76.2% (95% CI 70.9-80.6) with mFOLFOX6 alone - HR 0.50 (95% CI 0.35-0.73), P<0.001(NEJM, primary analysis, DCO2). At the earlier ASCO 2025 plenary interim analysis (37.2-month follow-up, 124 events), the same 3-year DFS was reported as 86.4% vs 76.6%, HR 0.50, P<0.0001(ASCO Post, DCO1 interim). Centrally-confirmed dMMR analysis maintained HR 0.53. Benefit was consistent across all subgroups (age, sex, race, tumor location, T/N stage, risk category).
At a median follow-up for OS of 45.8 months, death had occurred in 31 patients (atezolizumab arm) vs 33 patients (control arm), P=0.68. 5-year OS was 89.7% (95% CI 85.2-92.9) with atezolizumab plus mFOLFOX6 vs 87.9% (95% CI 83.1-91.4) with mFOLFOX6 alone - HR 0.90 (95% CI 0.55-1.47), not statistically significant(NEJM update, DCO2). OS data remain immature; longer follow-up is needed.
OS: HR 0.90 (0.55-1.47) · 89.7% vs 87.9% at 5 years · not significant (NEJM, DCO2)
Grade 3-4 adverse events occurred in 84.1% (atezolizumab arm) vs 71.9% (control arm) (NEJM update, DCO2) - the earlier ASCO 2025 interim reported 72.3% vs 59.2% treatment-related Grade 3-4 AEs (ASCO Post, DCO1). Most common Grade 3-4 AEs: decreased neutrophil count (43.6% vs 35.9%), peripheral sensory neuropathy (18.5% vs 15.0%), and fatigue (10.1% vs 3.3%). Grade 5 (fatal) AEs occurred in 6 patients (1.7%) in the atezolizumab arm vs 2 patients (0.6%) in the control arm; 2 deaths in the combination arm were considered treatment-related (1 sudden death, 1 sepsis). No clinically significant difference in Grade ≥3 immune-related AEs between arms.
Grade 3-4 AE 84.1% vs 71.9% · Grade 5 1.7% vs 0.6% (2 treatment-related deaths, combo arm) (NEJM, DCO2)
Clinical Debate - Adjuvant Chemoimmunotherapy vs Neoadjuvant Immunotherapy Alone
ASCO 2025 discussant Myriam Chalabi, MD, PhD (Netherlands Cancer Institute, PI of NICHE-2), noted that ATOMIC's 10% absolute DFS improvement is "an option to consider," but questioned whether 12 months of combined chemotherapy plus immunotherapy is over-treatment: chemotherapy has limited independent efficacy in dMMR tumors, and neoadjuvant immunotherapy alone (per NICHE-2: 95% pathologic response, 100% 3-year DFS with a short 2-cycle course) is more effective and better tolerated in early data. She raised the open question of whether chemotherapy could even blunt the anti-tumor T-cell response that drives immunotherapy benefit. These are non-randomized, smaller-sample comparisons - pathologic response is not a validated DFS surrogate, and longer follow-up is needed before adjuvant chemoimmunotherapy (ATOMIC) and chemotherapy-free neoadjuvant immunotherapy approaches can be directly compared.
Open question: adjuvant chemo+IO (ATOMIC) vs neoadjuvant IO-alone (NICHE-2) - non-randomized comparison
⚠ Investigational - not yet FDA approved. ATOMIC is the first phase 3 trial to show benefit from adding a checkpoint inhibitor to adjuvant chemotherapy in resectable colon cancer, and mFOLFOX6 + atezolizumab is already an NCCN Category 2A preferred regimen for stage III dMMR/MSI-H colon cancer ahead of the pending FDA decision (PDUFA October 9, 2026). The ESMO GI 2026 duration analysis (see above) is reshaping the practical question clinicians now face: not just whether to add atezolizumab, but how much chemotherapy is needed alongside it to preserve that benefit.
ATOMIC (Alliance A021502 / AIO-KRK-0317) is a Phase 3, randomized, open-label trial testing whether adding atezolizumab to adjuvant mFOLFOX6 chemotherapy improves disease-free survival versus mFOLFOX6 alone in patients with resected stage III colon cancer that is mismatch repair-deficient (dMMR) or microsatellite instability-high (MSI-H).
What were the ATOMIC trial disease-free survival results?
At a median follow-up of 40.9 months, 3-year disease-free survival was 86.3% with atezolizumab plus mFOLFOX6 versus 76.2% with mFOLFOX6 alone - a hazard ratio of 0.50 (95% CI 0.35-0.73, P<0.001), a 50% reduction in the risk of recurrence or death (NEJM, 2026).
Is atezolizumab FDA approved for adjuvant colon cancer?
No. Atezolizumab (Tecentriq) is not yet FDA approved for this adjuvant colon cancer indication. The FDA accepted a supplemental Biologics License Application and granted Priority Review in June 2026, with a target action (PDUFA) date of October 9, 2026.
What did the ATOMIC duration-of-therapy analysis show at ESMO GI 2026?
An exploratory analysis presented at ESMO GI 2026 found the disease-free survival benefit of atezolizumab was concentrated in patients who completed more than 6 cycles of mFOLFOX6 (HR 0.41) versus little apparent benefit in those who received 6 cycles or fewer (HR 0.97) - suggesting chemotherapy exposure may influence how much immunotherapy benefit patients receive. This is exploratory, hypothesis-generating data, not a confirmatory endpoint.
Is atezolizumab plus FOLFOX in the NCCN Guidelines for colon cancer?
Yes. FOLFOX (or CAPOX) plus atezolizumab was added as a Category 2A preferred regimen for adjuvant treatment of stage III dMMR/MSI-H colon cancer in the NCCN Colon Cancer Guidelines, reflected in Version 1.2026/2.2026, ahead of any FDA approval decision.