IRAKLIA at a Glance
Study Design
Phase 3, randomized, open-label, non-inferiority trial: Sarclisa SC via the CirCLIQ on-body injector at a fixed flat dose vs weight-based Sarclisa IV, both plus pomalidomide and dexamethasone (Pd), in relapsed/refractory multiple myeloma. (Sanofi Press / ASCO 2025)
Efficacy — ORR Non-Inferiority (Co-Primary)
ORR 71.1% (187/263) with Sarclisa SC-Pd vs 70.5% (189/268) with Sarclisa IV-Pd; non-inferiority established (relative risk 1.008, 95% CI 0.903–1.126, p=0.0006). Observed Ctrough co-primary also met. (Sanofi Press / ASCO 2025 abstract 7506)
Safety
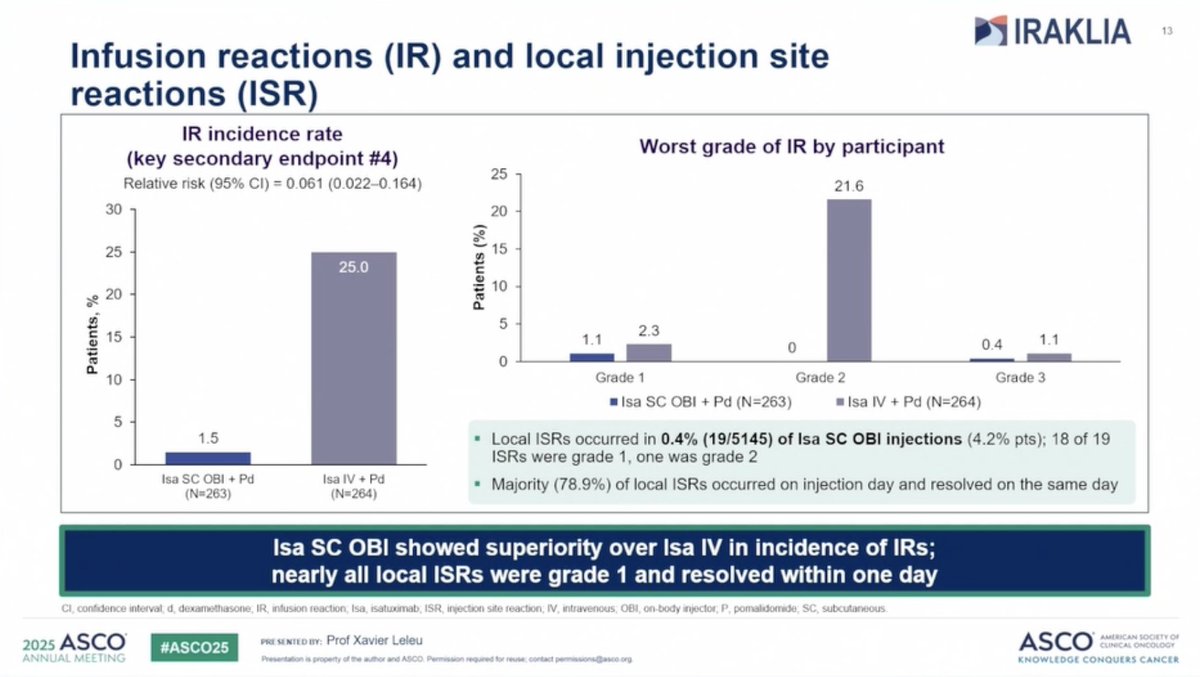
Systemic (infusion-related) reactions occurred in 1.5% of SC-Pd patients vs 25% of IV-Pd patients. Injection-site reactions were low-grade at 0.4% of OBI injections (19/5,145). No new safety concerns. (Sanofi Press)
Device
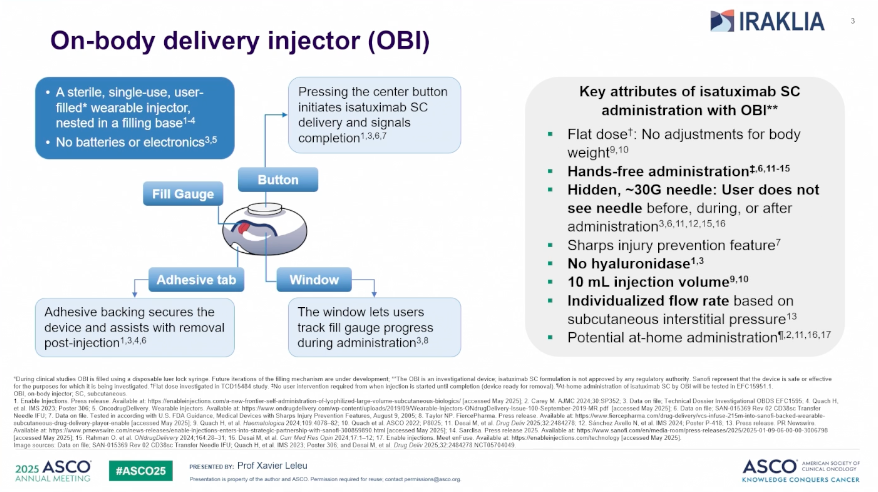
CirCLIQ on-body injector (Enable Injections, enFuse platform): sterile single-use wearable, no batteries/electronics, flat dose (no body-weight adjustment), hands-free, hidden ~30-gauge needle, 10 mL volume, individualized flow rate. (ASCO 2025 slide)
Regulatory
FDA approved July 10, 2026 — Sarclisa (isatuximab-irfc) Escena SC, the first anticancer treatment administered via an on-body injector, across all existing Sarclisa IV indications (Isa-VRd, Isa-Pd, Isa-Kd). (Sanofi Press, Jul 10 2026)
Sponsor & Drug
Sanofi. Drug: isatuximab-irfc (brand Sarclisa; SC formulation branded Sarclisa Escena), an anti-CD38 monoclonal antibody. (Sanofi Press)
Track oncology’s top KOLs in your specialty
Create a free account, pick the tumor types you cover, and go beyond the tweet — the intelligence pharma teams use to map influence and prepare for engagement:
- ✓Enhanced KOL profiles
- ✓Pharma influence & potential advisory-board patterns
- ✓2025 Open Payments financial analysis
- ✓Social-media sentiment & trend signals
Top KOLs Discussing IRAKLIA










IRAKLIA Key Slides & Visuals






IRAKLIA Top Tweets
Top physician voices discussing IRAKLIA — click to view on X
Press Release: New Sarclisa subcutaneous formulation met co-primary endpoints in the IRAKLIA phase 3 study in multiple myeloma
#mmsm @IMFmyeloma @theMMRF @HealthTree @LLSusa
https://t.co/WGsMD5NSYA
On-body isatuximab matches IV in myeloma, with fewer reactions❗️
The phase 3 IRAKLIA trial showed that subcutaneous isatuximab delivered via on-body delivery system (OBDS) is non-inferior to intravenous (IV) isatuximab when combined with pomalidomide and dexamethasone in https://t.co/4wBtMyPeSu
Bravo to the teams involved! It's a challenging road to be second in class, but
- more options for patients
- competition we can hope will bring prices down, and
- we can ask if there are any clinical differences with Dara that might be exploited
#mmsm #cancersucks https://t.co/Tka6h3Irpe
#mmsm #ASCO25 oral myeloma sessions
IRAKLIA study of OBI device of Isa
Cool device to deliver Isa
Study schema https://t.co/knuY1Ks0te
3/ #ASCO25 #MMsm newly Dx'ed:
7506 IRAKLIA (Ailawadhi): subQ isa via auto-injector (no slow RN push): non-inferior to IV Isa. Only 0.4% ISRs!
Plus ⬆️ pt satisfaction (albeit only 70% vs 53%, will need to see why not 100%). COLUMBA-like approval soon?
https://t.co/u7r6TtRdAZ https://t.co/uMkNK4sjY1
IRAKLIA study shows on body delivery system is safe, effective and preferred by patients. Cool fearture that time of administration depends on tissue resistance.
Called "escargot" in France! Less infusion/injection reactions (1.5 vs 25%)
#ASCO25 https://t.co/abwbFApAWv
#Myeloma Paper of the Day: Phase 3 IRAKLIA study shows Isatuximab (+Pom/dex) w/ on-body delivery system shows similar efficacy & pharmacokinetic non-inferiority versus Isa-iv/Pom/dex w/ no unexpected safety signal and lower infusion reaction rate: https://t.co/r10pHr405g. #mmsm https://t.co/Vp7A3kCIqj
Nice to see subQ isatuximab approved!
*But* reminds me of this study👇 from @majorajay- subQ forms (this was for BsAbs) didn’t lead to the time convenience I would have expected https://t.co/h2cxkuDEp3 https://t.co/XPqiBaENbM
FDA Approval
About the IRAKLIA Trial
IRAKLIA (NCT05405166) is a Phase 3, randomized, open-label, international non-inferiority study from Sanofi evaluating subcutaneous Sarclisa (isatuximab-irfc), delivered at a fixed flat dose via the CirCLIQ on-body injector, versus weight-based intravenous Sarclisa, both combined with pomalidomide and dexamethasone (Pd), in adults with relapsed/refractory multiple myeloma. The trial enrolled 531 patients and met both co-primary endpoints — overall response rate (71.1% SC-Pd vs 70.5% IV-Pd; non-inferior) and observed Ctrough at steady state — while systemic (infusion-related) reactions fell from 25% with IV to 1.5% with the on-body injector. On the strength of these data, the subcutaneous formulation, branded Sarclisa Escena, became the first anticancer treatment administered via an on-body injector and was FDA approved on July 10, 2026 across all existing Sarclisa IV indications.
Trial Methodology & Results
Study Design
Phase 3, randomized, open-label, non-inferiority study (NCT05405166) comparing Sarclisa SC via the CirCLIQ on-body injector at a fixed flat dose vs weight-based Sarclisa IV.
Population
Adults with relapsed/refractory multiple myeloma who received at least 1 prior line of therapy; all received a pomalidomide + dexamethasone (Pd) backbone.
Interventions
Isatuximab SC via CirCLIQ on-body injector (or manual SC injection) + Pd, versus weight-based isatuximab IV + Pd.
Endpoints
Co-primary: (1) ORR by IMWG 2016 (Independent Review Committee) and (2) observed Ctrough at steady state (pre-dose cycle 6 day 1). Both met.
Device
CirCLIQ on-body injector (Enable Injections, enFuse platform): sterile single-use wearable; flat dose; hands-free; hidden ~30-gauge needle; no hyaluronidase; 10 mL volume; individualized flow rate; potential at-home administration. Now FDA approved (Jul 10, 2026).
Lead Author / PI
Sikander Ailawadhi, MD (Mayo Clinic, Jacksonville, FL), principal investigator; ASCO 2025 primary analysis (abstract 7506) presented by Xavier Leleu, MD; senior author Philippe Moreau, MD.
Overall Response Rate (Co-Primary Endpoint)
ORR was 71.1% (187/263) with Sarclisa SC-Pd vs 70.5% (189/268) with Sarclisa IV-Pd, establishing non-inferiority (relative risk 1.008, 95% CI 0.903–1.126, p=0.0006). Median on-body-injector administration was 13 minutes, identical in the clinic and at home. Source
Non-inferiority established: ORR 71.1% SC vs 70.5% IV (RR 1.008, p=0.0006)Source: Sanofi press release + IRAKLIA ASCO 2025 abstract 7506 (ClinicalTrials.gov NCT05405166)
Pharmacokinetics — Ctrough at Steady State (Co-Primary Endpoint)
Geometric mean Ctrough at steady state (predose C6D1) was 426 µg/mL with Sarclisa SC-Pd (N=121) vs 278 µg/mL with Sarclisa IV-Pd (N=121); geometric mean ratio 1.532 (90% CI 1.316–1.784), with the lower CI above the non-inferiority margin of 0.8 — establishing pharmacokinetic non-inferiority. Where home administration was permitted, all OBI injections were completed (100%) with no new safety signals. Source
Ctrough 426 vs 278 µg/mL — GMR 1.532 (PK non-inferior)Source: IRAKLIA ASCO 2025 abstract 7506 (ClinicalTrials.gov NCT05405166)
Safety & Tolerability
Systemic administration (infusion-related) reactions occurred in 25% of IV-Pd patients vs 1.5% of SC-Pd patients (relative risk 0.061, 95% CI 0.022–0.164). Injection-site reactions were low-grade and occurred in 0.4% of on-body injector injections (19/5,145 injections). The overall safety profile was consistent with established Sarclisa IV-Pd, with no new safety concerns. Grade ≥3 hematologic lab abnormalities (OBI vs IV): neutropenia 84.7% vs 74.3%, thrombocytopenia 26.1% vs 23.0%, anemia 17.6% vs 19.5%. Grade ≥3 non-hematologic AEs: pneumonia 14.8% vs 15.5%, COVID-19 2.7% vs 1.9%, upper respiratory tract infection 1.5% in both arms. Source
Infusion-related reactions: 1.5% SC vs 25% IV (RR 0.061)Source: Sanofi press release (Jul 10, 2026)
Patient Preference — Supportive Phase 2 IZALCO Study (NCT05704049)
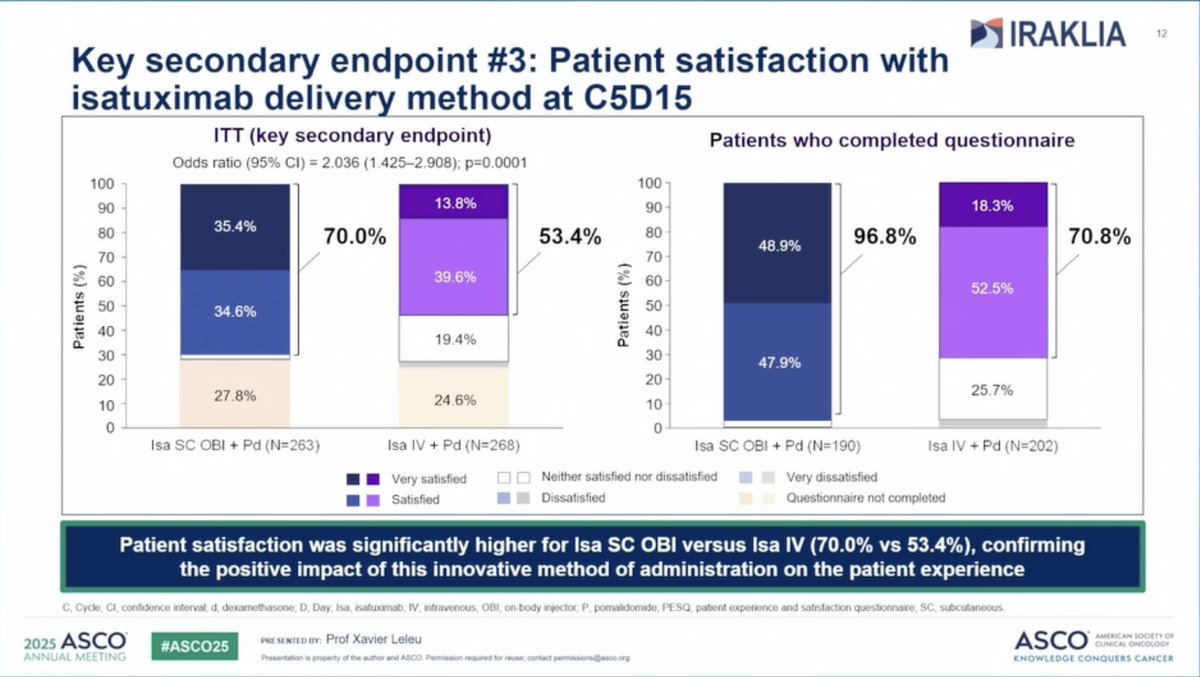
In the Phase 2 IZALCO study (NCT05704049) — a separate patient-preference study of subcutaneous isatuximab via the on-body injector — after experiencing both methods, 74.5% of patients preferred the on-body injector over manual SC injection (17% preferred manual; 8.5% no preference; p=0.0004). In IRAKLIA itself, patient satisfaction (very satisfied plus satisfied) at C5D15 was 70.0% for Sarclisa SC-Pd vs 53.4% for IV-Pd (odds ratio 2.036, 95% CI 1.425–2.908, p=0.0001). Source
IZALCO: 74.5% preferred the on-body injector (p=0.0004)Source: IZALCO — ClinicalTrials.gov NCT05704049
IRAKLIA in the News
Key KOL Sentiments - IRAKLIA
Frequently Asked Questions
Is subcutaneous Sarclisa FDA approved?
Yes. On July 10, 2026, the FDA approved Sarclisa (isatuximab-irfc) Escena — the subcutaneous formulation delivered via the CirCLIQ on-body injector — for multiple myeloma. It is the first anticancer treatment administered via an on-body injector, approved across all existing Sarclisa IV indications.
What is the CirCLIQ on-body injector?
The CirCLIQ on-body injector (OBI), made by Enable Injections on its enFuse platform, is a sterile, single-use, user-filled wearable device with no batteries or electronics. It delivers a flat dose of isatuximab SC hands-free, using a hidden ~30-gauge needle, a 10 mL injection volume, and an individualized flow rate based on subcutaneous interstitial pressure, with potential for at-home administration.
How did SC compare to IV in IRAKLIA?
In the Phase 3 IRAKLIA non-inferiority trial, Sarclisa SC (via on-body injector) plus pomalidomide and dexamethasone met both co-primary endpoints. ORR was 71.1% (187/263) with SC-Pd vs 70.5% (189/268) with IV-Pd — non-inferiority established (relative risk 1.008, 95% CI 0.903–1.126, p=0.0006) — and observed Ctrough at steady state was non-inferior. Systemic (infusion-related) reactions occurred in 1.5% of SC-Pd patients vs 25% of IV-Pd patients.
Which regimens are approved?
Sarclisa Escena SC is approved across all existing Sarclisa IV indications: Isa-VRd (with bortezomib, lenalidomide, and dexamethasone) in newly diagnosed MM patients not eligible for autologous stem cell transplant; Isa-Pd (with pomalidomide and dexamethasone) in R/R MM patients who received at least 2 prior therapies; and Isa-Kd (with carfilzomib and dexamethasone) in R/R MM patients who received 1–3 prior lines.
Who sponsored IRAKLIA?
IRAKLIA (NCT05405166) was sponsored by Sanofi. The principal investigator and lead author was Sikander Ailawadhi, MD (Mayo Clinic, Jacksonville, FL); the ASCO 2025 primary analysis (abstract 7506) was presented by Xavier Leleu, MD, with senior author Philippe Moreau, MD.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 10, 2026.