High-risk early triple-negative breast cancer (TNBC), post-surgery + (neo)adjuvant chemotherapy — University of Padova (Department of Surgery, Oncology and Gastroenterology); drug supply and financial support from Merck KGaA
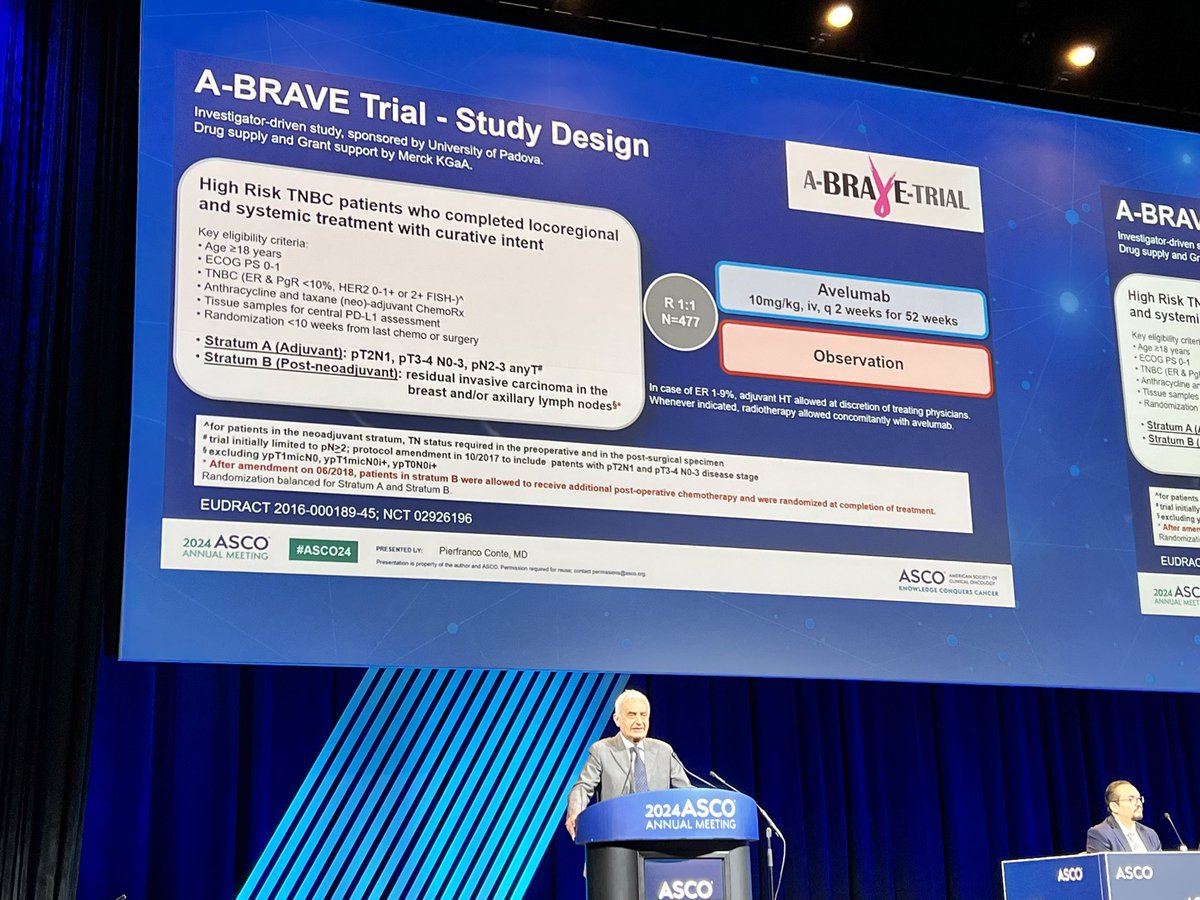
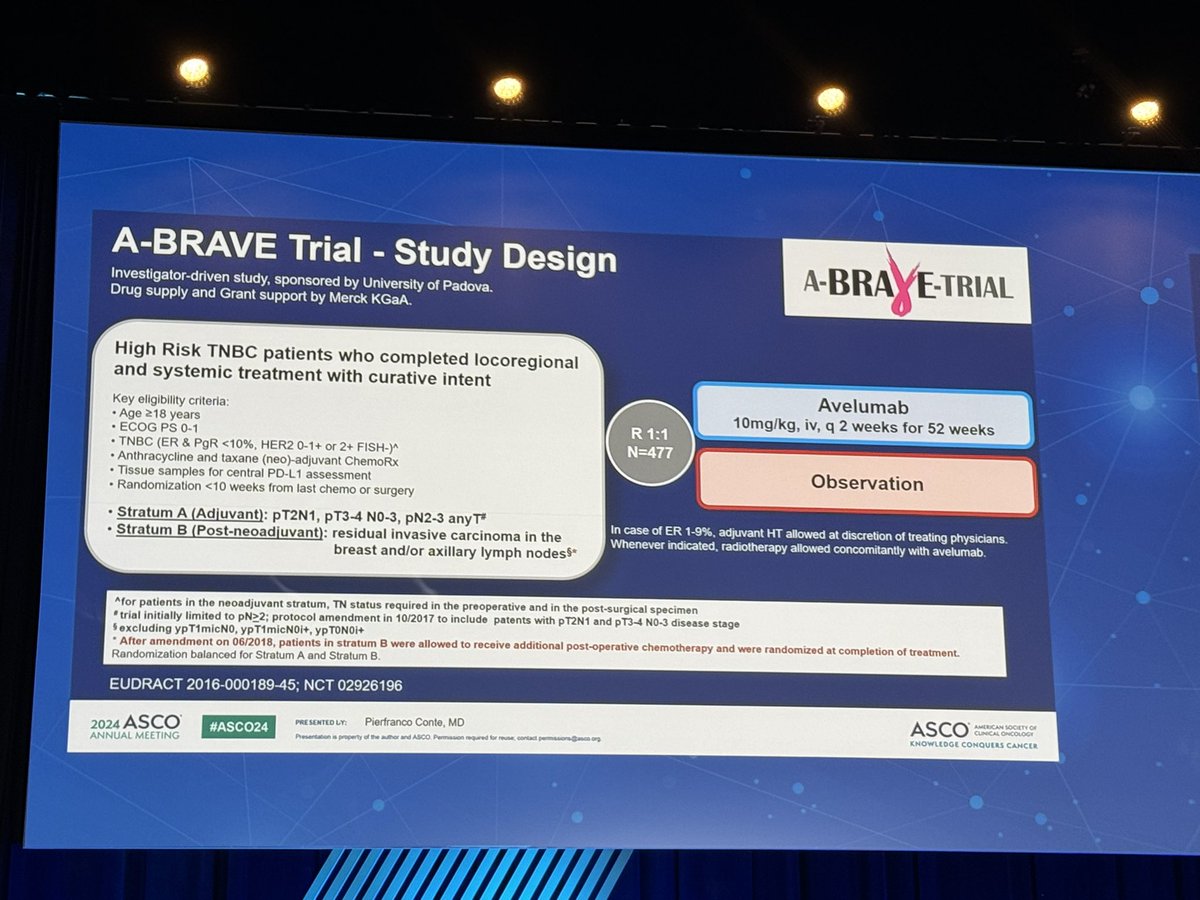
Discover KOL Sentiment on A-BRAVE →Design - Phase 3 academic randomized trial of 1 year adjuvant avelumab (Bavencio) vs observation in high-risk early TNBC after surgery + (neo)adjuvant chemotherapy (NCT02926196; University of Padova; Merck KGaA drug supply).
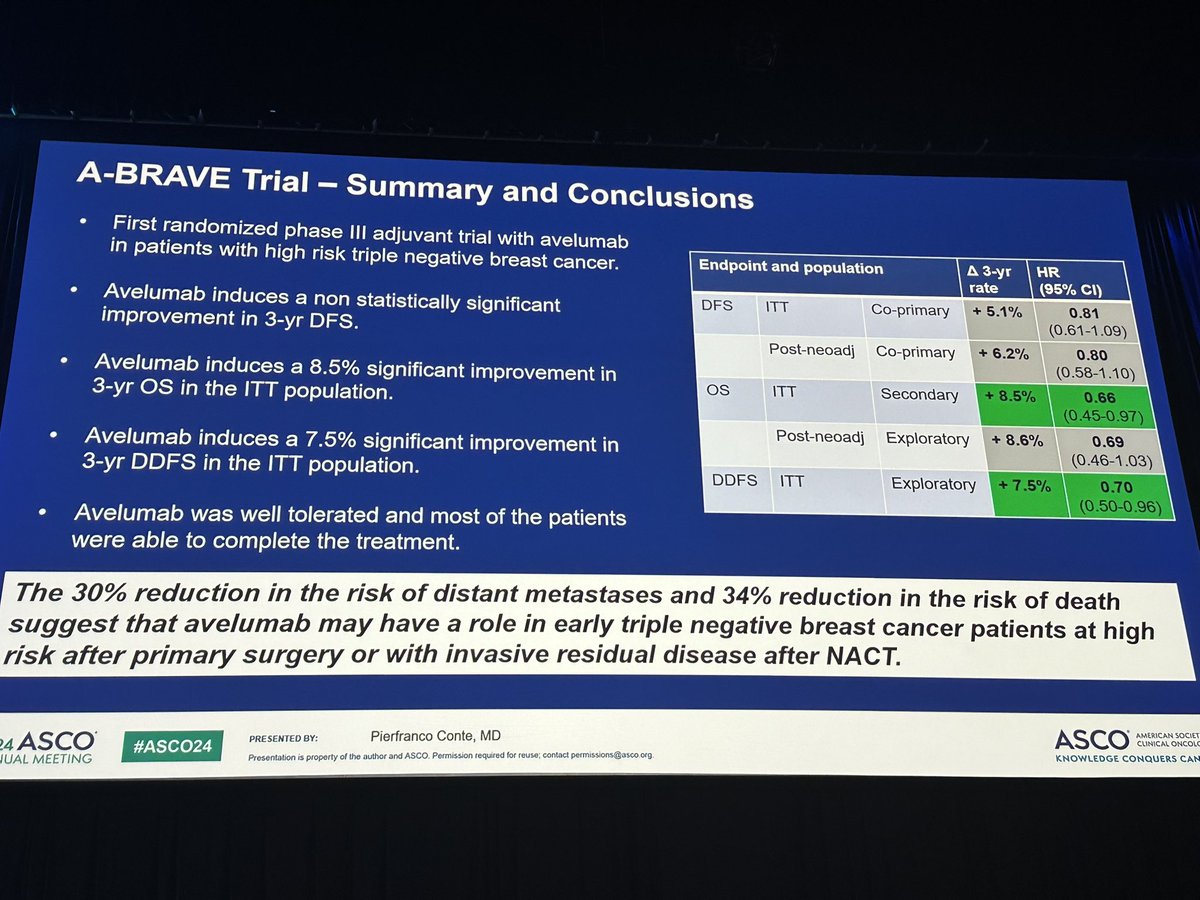
DFS (co-primary, MISSED) - 3-year DFS 68.3% (avelumab) vs 63.4% (observation), ITT HR 0.82 (95% CI 0.61-1.11), P=0.193; Stratum A (post-neoadjuvant) 66.9% vs 61.0%.
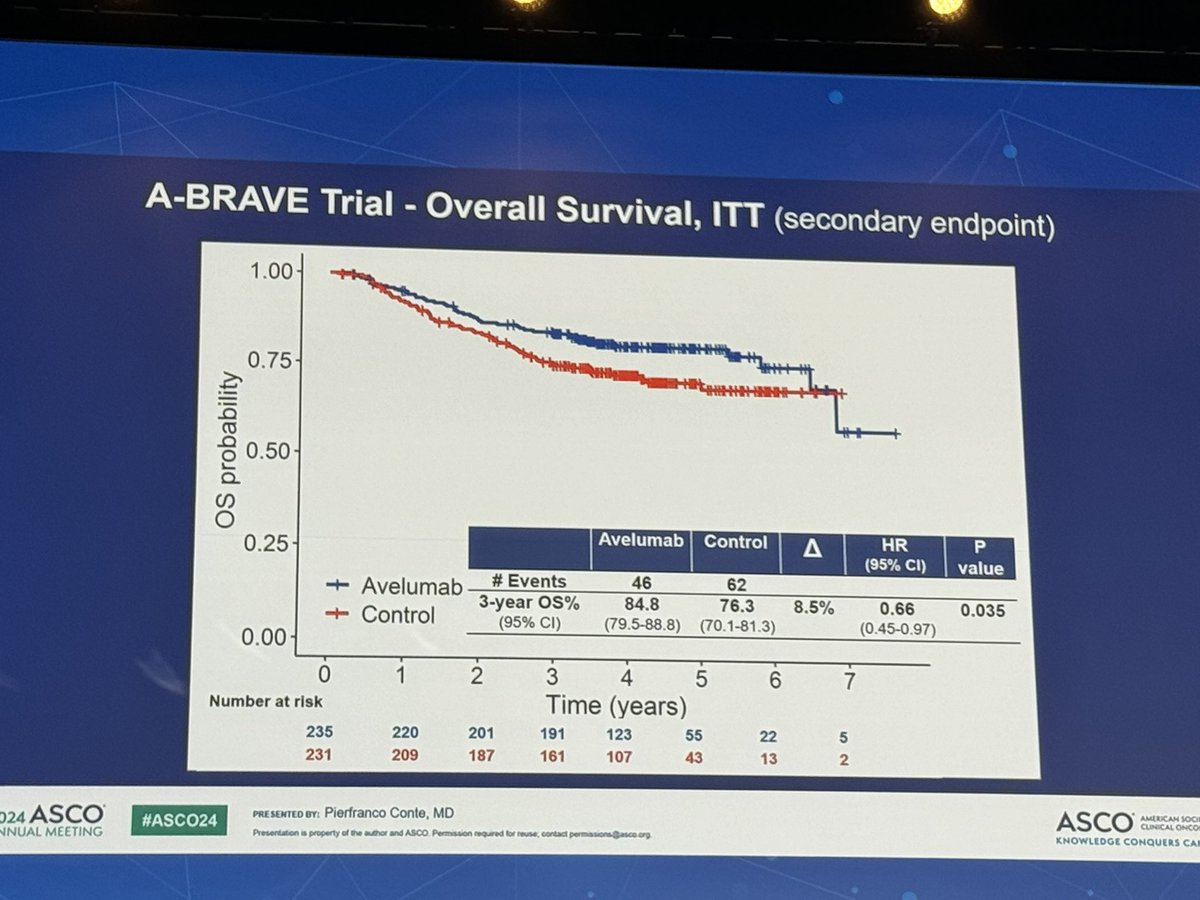
Overall survival (secondary, POSITIVE) - HR 0.66 (95% CI 0.44-0.98), P=0.041 - a 34% reduction in risk of death; 3-year OS 85.2% vs 78.2% (ITT).
Safety - Key immune-related events: hypothyroidism (13.2%), colitis/diarrhea (7.2%), hyperthyroidism (4.7%), transaminase increase (4.7%); 72% completed 1 year, grade >=3 irAEs 1.3%, no treatment-related deaths.
Interpretation - Unusual pattern - negative co-primary DFS but positive secondary OS; role remains unclear in the current KEYNOTE-522 era.
Regulatory / sponsor - Investigational in adjuvant TNBC; avelumab (Bavencio) approved in other indications. University of Padova; Merck KGaA/Pfizer alliance.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.















Top tweets by impressions — click to view on X
A-BRAVE adjuvant avelumab in TNBC.
Misses primary endpoint 5% 🔼PFS
Hits secondary endpoint 8.5% 🔼OS
What to do?
If you ‘reject” b/c of surrogate of PFS, you forsake a + result in more important…
A-BRAVE adjuvant avelumab in TNBC.
Misses primary endpoint 5% 🔼PFS
Hits secondary endpoint 8.5% 🔼OS
What to do?
If you ‘reject” b/c of surrogate of PFS, you forsake a + result in more important…
ABRAVE trial: Adj avelumab x 1yr in TNBC, n=477
2 strata: Adj tx, B: post preop tx
24% adj Cape
3 yr DFS: 63.2 vs 68.3%, HR 0.81, p=0.17
3 yr DFS in Stratum B; 60.7 vs 66.9, NS
3 yr DDFS 67.9 vs…
A-BRAVE phase 3: among pts with TNBC and (mostly) RD after NACT, adjuvant avelumab for 1 year did not sign improve DFS (68.3% vs 63.2%, p=0.1) but did improve DDFS and OS (84.8% vs 76.3%, p=0.02),…
A-BRAVE: adjuvant aveulmab after definitive treatment for high risk TNBC
❌DFS not significantly improved~5% numerically diff
✅ OS 8.5 months better!
✅ DDFS 7.5% better, HR 0.70
#ASCO24
#bcsm…
So apart from plenary sessions - what intresting Data coming up for Breast cancer at #asco24 @ASCO
1- postMONARCH trial - Abemaciclib post progression on CDK4/6 inhibitors in MBC .
Can we give…
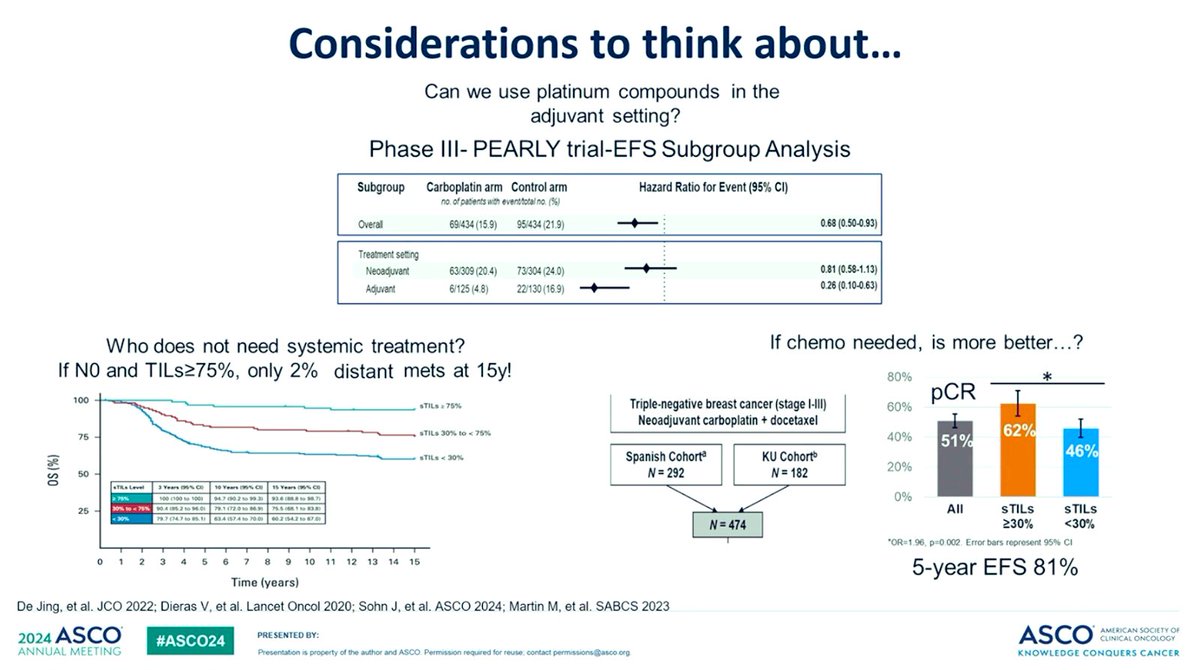
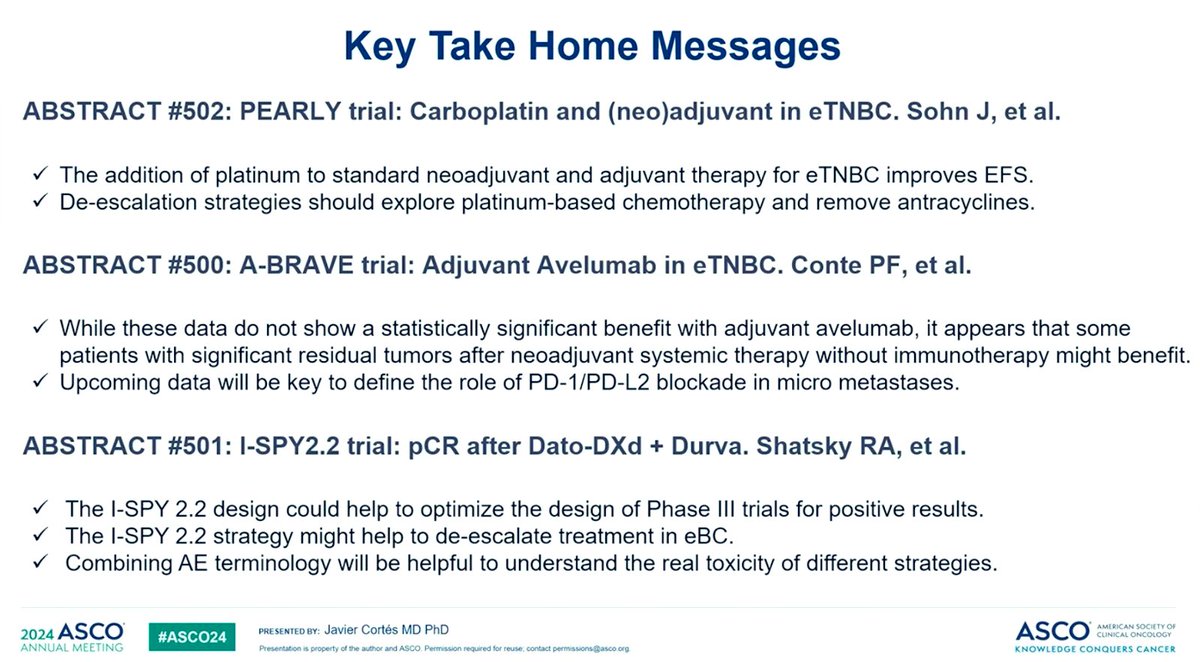
Is More Better? Customizing Systemic Therapy for High-Risk, Nonmetastatic Breast Cancer ➡️ Outstanding discussion 🔛 PEARLY trial, A-BRAVE trial and ISPY2.2 trial by @JavierCortesMD 👏🏻👏🏻👏🏻
#ASCO24…

#ASCO24 Conte describes results of ABrave. Adjuvant and post neoadjuvant Avelumab. Did not meet primary DFS endpoint but improved OS. Intriguing data. @OncoAlert https://t.co/Tj5hUz50wh
Another trial with NO DFS benifit ( Hr -0.81 , p value - 0.172 but OS benifit. HR - 0.66 - p value 0.035 ) A -Brave trial.
Is this not happening more often now a days ? @Timothee_MD @VPrasadMDMPH…

#ABRAVE: PhIII, Adj Avelumab in TNBC after NACT:
- Did not meet PFS end point but met OS secondary endpoint.
- 3yr OS84.8% w/ Avelumab vs. 76.3% (HR 0.66)
- KN522 as SoC, how does this fit in?…
A-BRAVE is an unusual trial in that it missed both co-primary DFS endpoints but showed a statistically significant 34% OS reduction as a secondary endpoint — a discrepancy that raises interpretive questions. In the current era where KEYNOTE-522 (neoadjuvant pembro+chemo) is SOC for high-risk early TNBC, A-BRAVE may apply to the real-world 'miss-the-window' population: patients who received neoadjuvant chemo alone (no pembro) and had residual disease at surgery. The OS signal suggests adjuvant IO may still benefit these patients. Discussant noted PD-L1 status data should be explored. SWOG S1418 (pembrolizumab adjuvant in TNBC residual disease post-neoadj) is the most directly comparable ongoing trial.
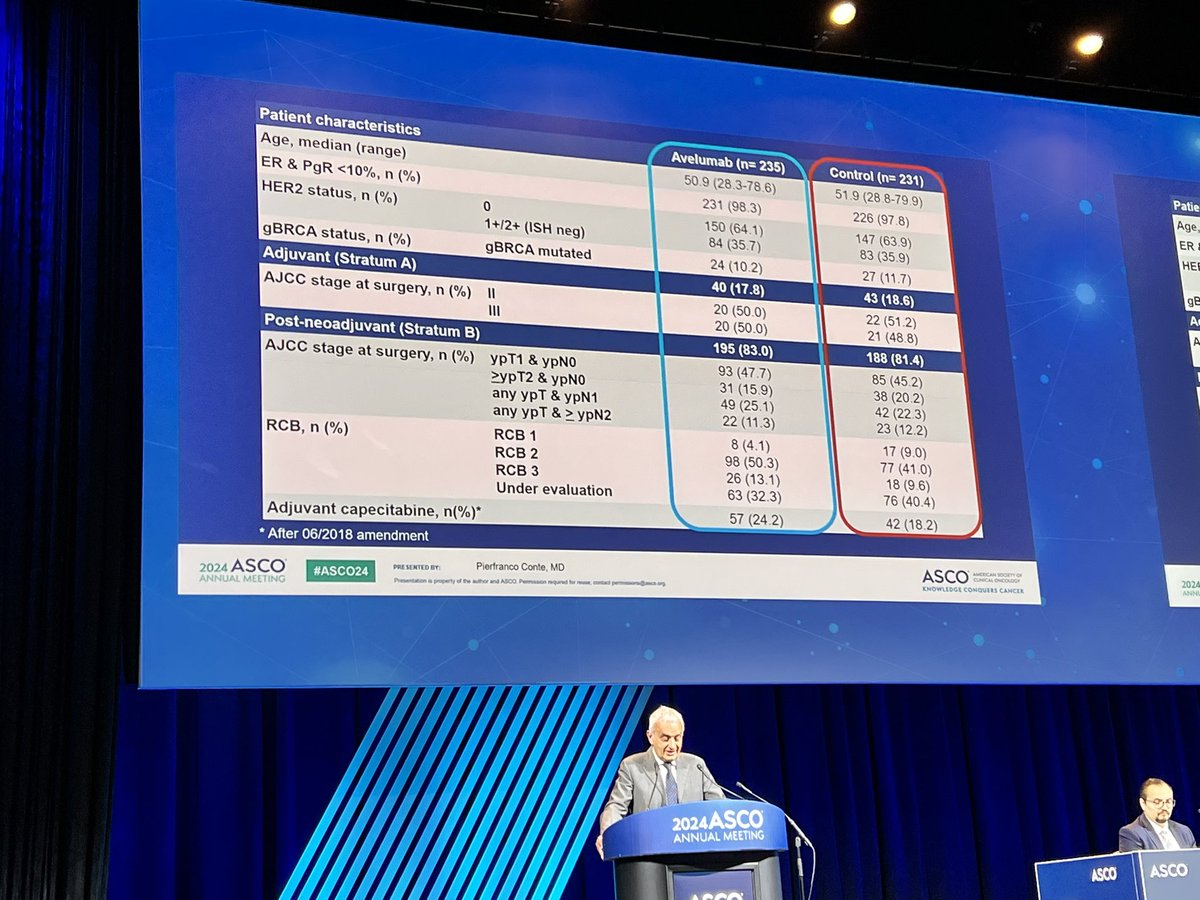
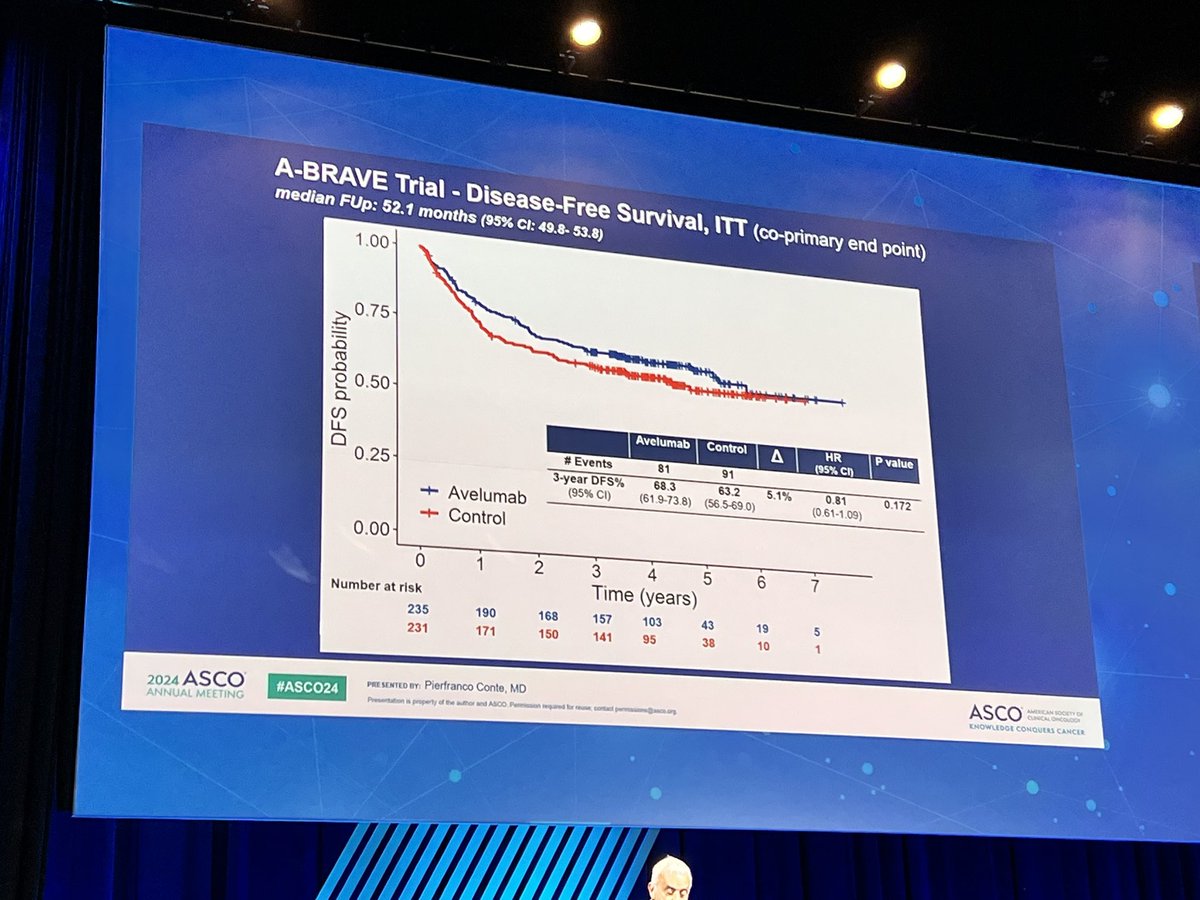
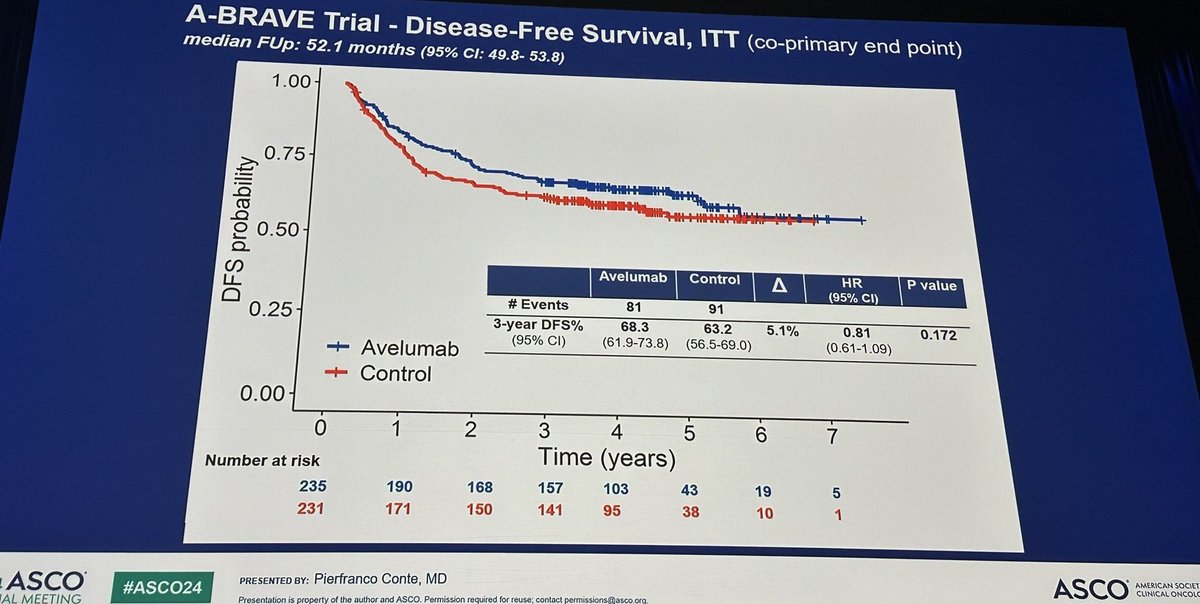
Median: 68.3 % 3-yr DFS (avelumab ITT) vs. 63.4 % 3-yr DFS (control (observation) ITT). HR 0.82 (95% CI 0.61-1.11), P=0.193 3-yr DFS ITT rate: 68.3% (avelumab) vs. 63.4% (control). 3-yr DFS Stratum A (post-neoadjuvant) rate: 66.9% (avelumab) vs. 61.0% (control). A-BRAVE did NOT meet its co-primary DFS endpoints. ITT DFS: HR 0.82 (95% CI 0.61-1.11, P=0.193); 3-yr DFS 68.3% vs. 63.4%. Stratum A (post-neoadjuvant, n=378): HR 0.81 (95% CI 0.58-1.11, P=0.194); 3-yr DFS 66.9% vs. 61.0%. N=477 randomized (64 Italian + 6 UK centers). 11 patients withdrew consent post-randomization. Stratum A = invasive residual disease after neoadjuvant chemo (83%); Stratum B = high-risk post-primary-surgery (17%). Median follow-up 52.1 months. Conte et al., Ann Oncol 2025;36(12):1492-1502.
HR 0.66 (95% CI 0.44-0.98), P=0.041 Secondary OS endpoint SIGNIFICANTLY IMPROVED in ITT: median OS HR 0.66 (95% CI 0.44-0.98, P=0.041) — 34% reduction in risk of death. 3-yr OS 85.2% vs. 78.2% (ITT); 83.1% vs. 76.6% (Stratum A). Post-hoc analysis showed fewer distant disease events (48 vs. 58) and fewer deaths before documented DFS event (1 vs. 4) with avelumab. Discrepancy between DFS (negative) and OS (positive) signals is an ongoing point of scientific discussion; DFS was driven partly by non-BC events and may have been underpowered for magnitude of effect observed.
Key AEs: hypothyroidism (13.2%), colitis/diarrhea (7.2%), hyperthyroidism (4.7%), increased transaminases (4.7%). Well tolerated: 72% of patients completed 1 year of avelumab treatment. Grade ≥3 immune-related AEs occurred in only 1.3% of patients. No treatment-related deaths were reported.
⚠ Negative primary (DFS) but positive secondary (OS). Mixed signal; role unclear post-KEYNOTE-522. A-BRAVE is an unusual trial in that it missed both co-primary DFS endpoints but showed a statistically significant 34% OS reduction as a secondary endpoint — a discrepancy that raises interpretive questions. In the current era where KEYNOTE-522 (neoadjuvant pembro+chemo) is SOC for high-risk early TNBC, A-BRAVE may apply to the real-world 'miss-the-window' population: patients who received neoadjuvant chemo alone (no pembro) and had residual disease at surgery. The OS signal suggests adjuvant IO may still benefit these patients. Discussant noted PD-L1 status data should be explored. SWOG S1418 (pembrolizumab adjuvant in TNBC residual disease post-neoadj) is the most directly comparable ongoing trial.
A-BRAVE (NCT02926196) is an academic Phase 3 randomized trial led by the University of Padova that tested one year of adjuvant avelumab (Bavencio) versus observation in patients with high-risk early triple-negative breast cancer after surgery and (neo)adjuvant chemotherapy. Drug supply and financial support came from Merck KGaA. It had co-primary disease-free survival endpoints in the ITT and post-neoadjuvant (Stratum A) populations.
A-BRAVE missed both co-primary disease-free survival endpoints - 3-year DFS was 68.3% with avelumab versus 63.4% with observation (hazard ratio 0.82, P=0.193). However, the secondary overall-survival endpoint was statistically significant, with a 34% reduction in the risk of death (hazard ratio 0.66, 95% CI 0.44-0.98, P=0.041) and 3-year overall survival of 85.2% versus 78.2%.
No. Adjuvant avelumab is not FDA-approved for early triple-negative breast cancer, and its use in A-BRAVE is investigational. Avelumab (Bavencio) is separately FDA-approved in metastatic Merkel cell carcinoma, as maintenance in advanced urothelial carcinoma, and with axitinib in advanced renal cell carcinoma.
Avelumab was well tolerated: 72% of patients completed the full year of treatment, and grade 3 or higher immune-related adverse events occurred in only 1.3% with no treatment-related deaths. The most common immune-related events were hypothyroidism (13.2%), colitis/diarrhea (7.2%), hyperthyroidism (4.7%) and transaminase elevation (4.7%).
A-BRAVE is unusual because it missed its co-primary disease-free survival endpoints yet showed a significant secondary overall-survival benefit - a discrepancy that raises interpretive questions. In the current era where neoadjuvant pembrolizumab (KEYNOTE-522) is standard for high-risk early TNBC, the role of adjuvant avelumab remains unclear and the OS signal is viewed as hypothesis-generating.