Suspected advanced non-small cell lung cancer (NSCLC) — diagnostic workflow optimization — Princess Margaret Cancer Centre / University Health Network (Toronto)
Discover KOL Sentiment on ACCELERATE →Design - Prospective observational diagnostic-workflow study of upfront plasma ctDNA genotyping (InVisionFirst-Lung, Inivata) at referral, before tissue diagnosis, in suspected advanced NSCLC (NCT04863924; University Health Network / Princess Margaret, Toronto).
Primary endpoint - time to treatment - Median referral-to-treatment 39 days (IQR 27-52) with upfront plasma vs 62 days (IQR 44-82) with standard tissue-first testing - 23 days faster.
Molecular yield - 12% of patients had actionable alterations identified only through plasma - alterations that would have been missed or delayed by a tissue-only pathway.
Overall survival - Survival was not a primary endpoint; ACCELERATE measured operational/diagnostic outcomes, not therapeutic efficacy.
Safety - Diagnostic-workflow study - no therapeutic intervention and no drug-safety endpoints.
Regulatory / sponsor - Observational; no drug approval. Assay InVisionFirst-Lung (Inivata). Sponsor University Health Network. Garcia-Pardo et al., JAMA Network Open 2023.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.











Top tweets by impressions — click to view on X
🚨ACCELERATE Trial🚨
Resected Gallbladder Adenocarcinoma
🔎Randomized
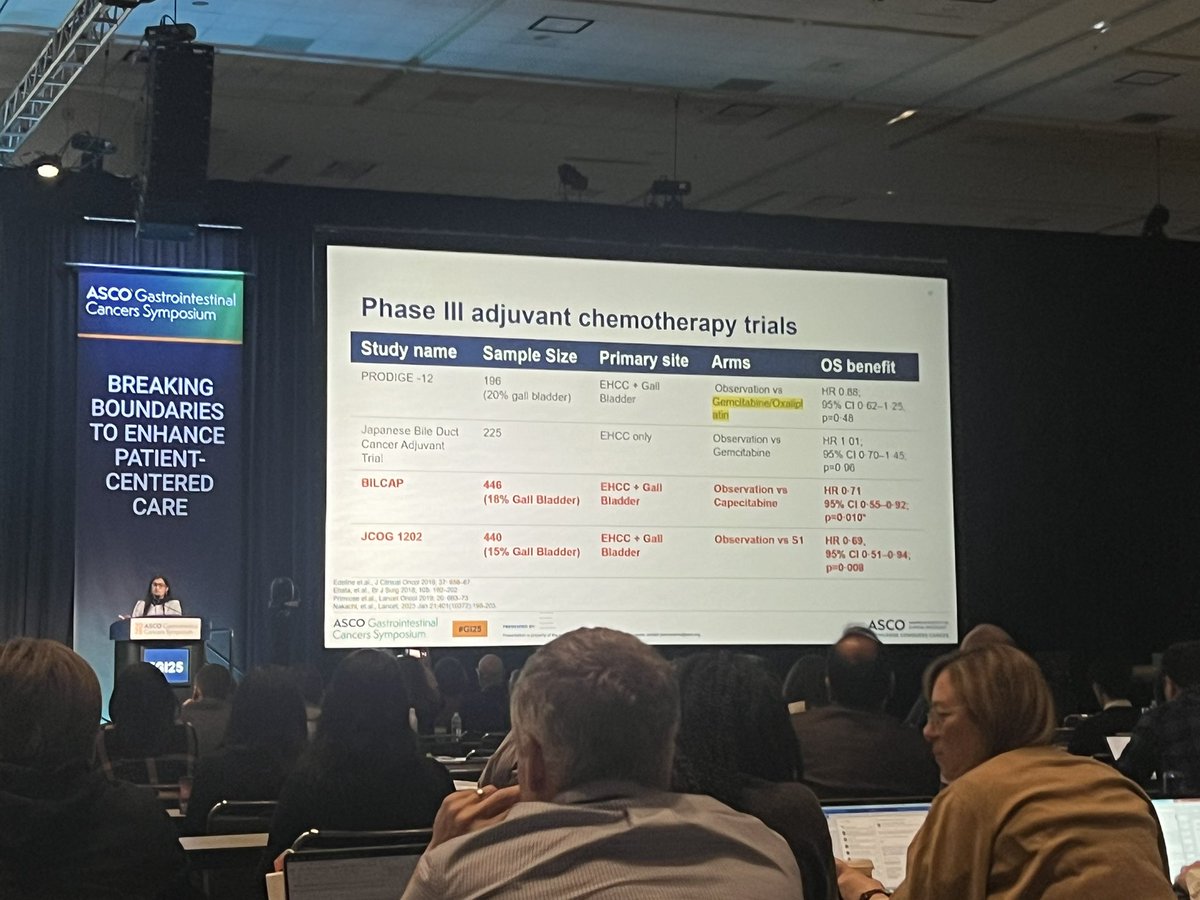
6c Systemic tx (Gem-Ox or Gem-Cis)
vs
3c Systemic Tx ▶️CRT (45 Gy/25 fx)▶️3c Systemic Tx
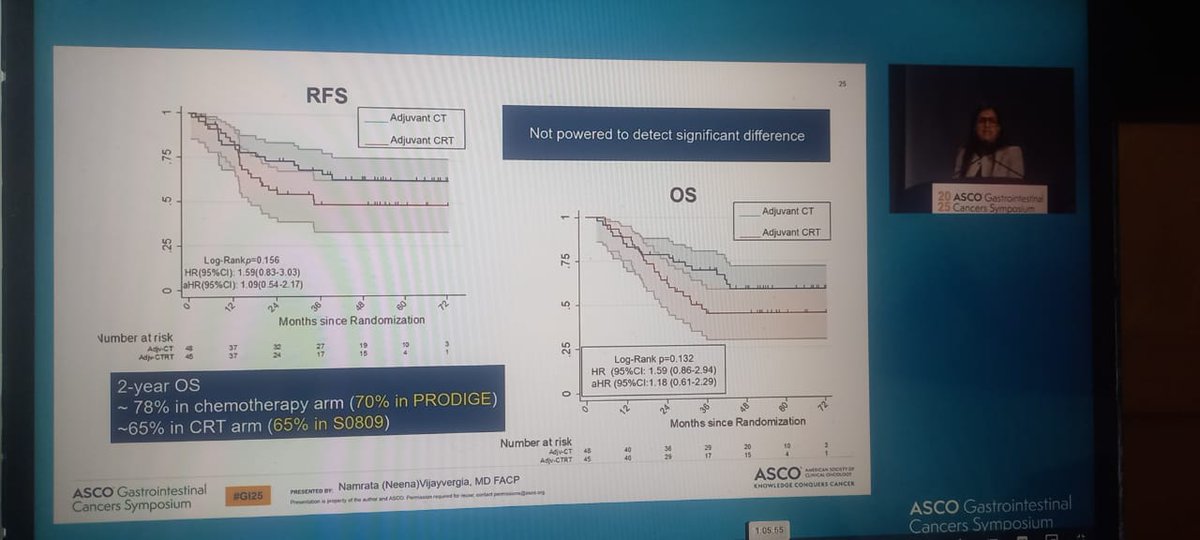
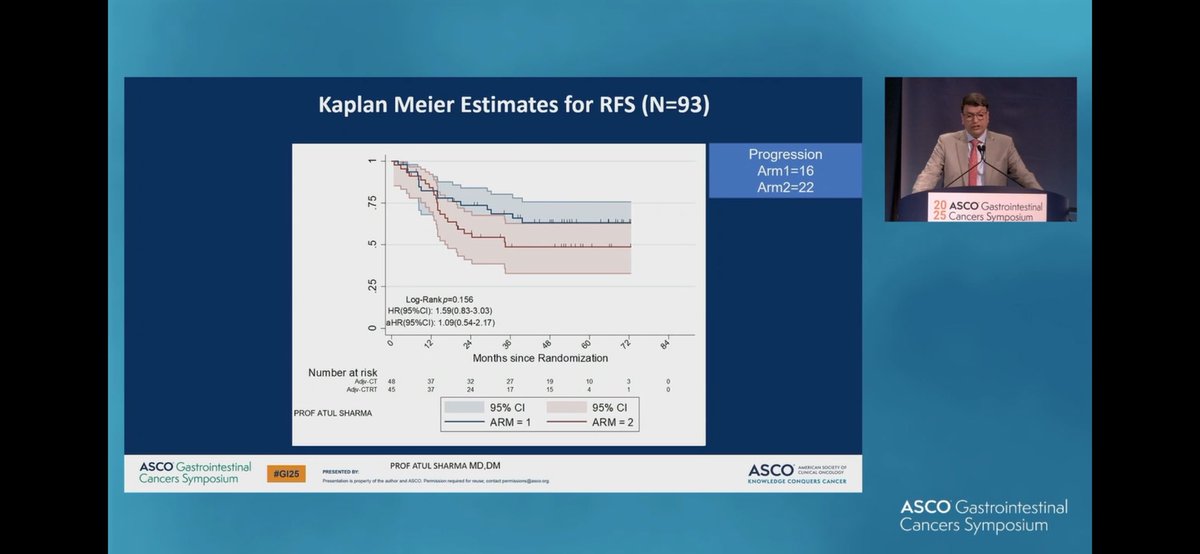
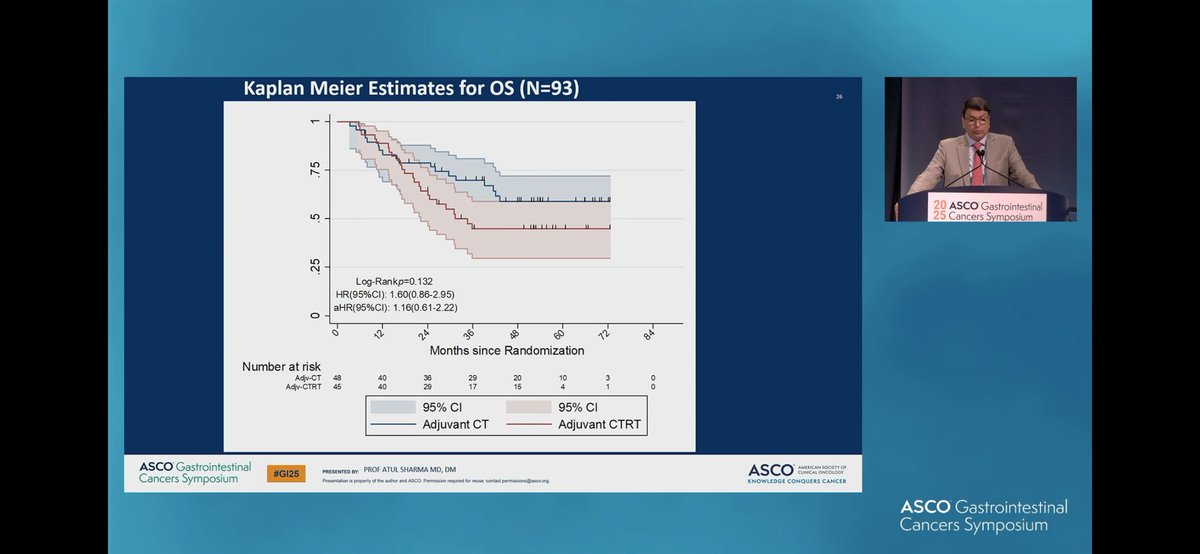
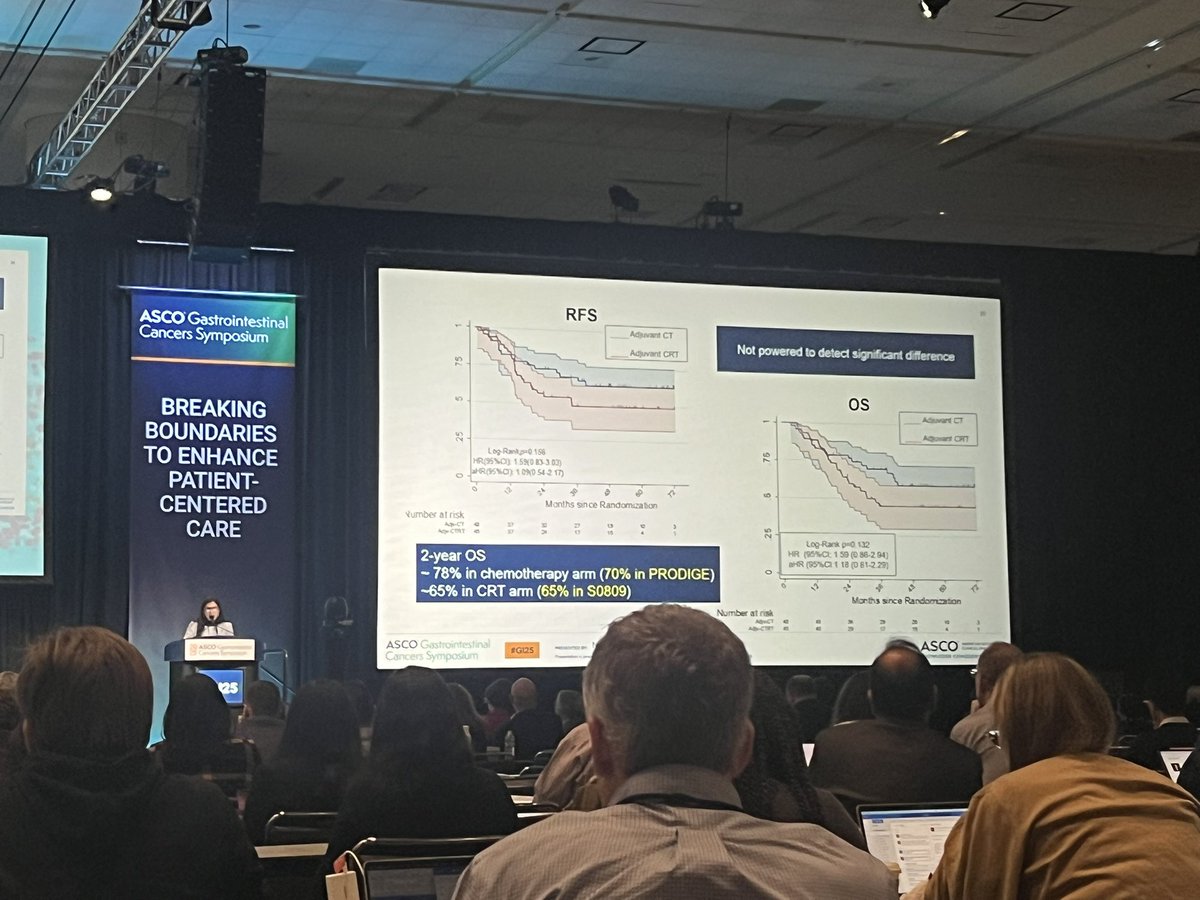
⛔️No improvement in OS or RFS with…
Adjuvant chemotherapy vs Adjuvant CTRT in Gall bladder cancer . Phase 3 RCT from India 🇮🇳 @aiims_newdelhi presented by Prof Dr Atul Sharma . Adjuvant chemo rt dose not add much benifit to Adjuvant…
Following up with presentation!
RCT
Gem-Ox or Gem-Cis +/- CRT for resected gallbladder cancer
In this relatively small study that incompletely accrued, there was not a significant improvement in…
Dr. Sharma presenting P3 ACCELERATE trial: Adjuvant chemotherapy or chemoRT in gallbladder cancer: GemOx +/- capeRT. No improvement in RFS or OS w/ addition of RT. Worse RFS for pts with elevated CA…
ACCELERATE trial in GBC
➡️adjuvant chemo (gemox/ cis/gem) vs chemo +CRT
➡️94 pts enrolled;planned 200
➡️no benefit of +rads (despite underpowered )
➡️med RFS 52 vs 44mths
➡️small study ? Would…
👏🏽 to the ACCELERATE 🏎️ investigators for first
dedicated GBCA RCT 🇮🇳 to compare adjuvant
chemotherapy vs chemoRT #GI25
No diff in RFS between 6c GemOx or GemCis vs
3c chemo followed by 45 Gy of…
Role for adjuvant ☢️ in GBCA after chemo?
@NVijayvergiaMD giving a master class #GI25
ACCELERATE trial 🇮🇳
Chemotherapy 💪 outperformed prior RCTs
Chemo ☢️ 💪 results similar to @SWOG S0809
Lack of…
ACCELERATE rand PhIII of adjuvant IC chemo (gem/ox or cis/gem) vs chemo + chemoRT in >pT2 or N+ resected #gallbladder cancer ➡️ no sig diff in RFS or OS between arms
@ASCO #GI25
@OncoAlert…

#GI25
ACCELERATE (great name, negative trial)
Resected Gallbladder adenocarcinoma
adjuvant chemotherapy vs chemoRT
No change in outcomes between chemo (GemCis/GemOx) vs Chemo + RT
45 vs 48…
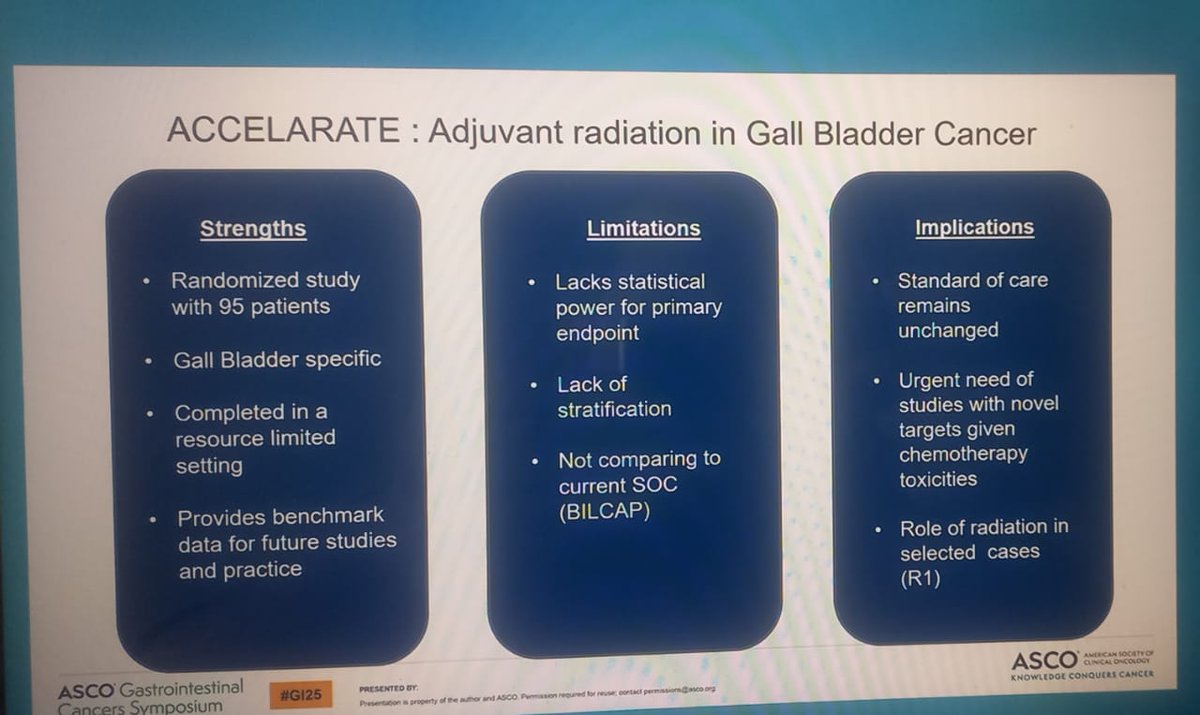
Additional considerations when interpreting the study
The chemo alone group received more cycles of chemo AND had lower stage disease, each of which were associated with survival.
At present,…
ACCELERATE validates a workflow change in advanced NSCLC diagnosis: plasma ctDNA testing at referral (before tissue biopsy confirmation) gets patients to treatment 23 days faster and catches actionable alterations (12%) that tissue-only testing would have missed. Implementation requires coordinated referral-to-oncology pathway with liquid biopsy at point of entry. Complements established tissue NGS in the hybrid testing paradigm. Expanding adoption of this model could accelerate targeted therapy initiation across thoracic oncology practice, especially in EGFR/ALK/ROS1/KRAS G12C/MET/BRAF/HER2/RET/NTRK-eligible patients.
Median: 39 days (IQR 27-52) (ACCELERATE cohort (plasma ctDNA before tissue dx)) vs. 62 days (IQR 44-82) (Reference cohort (standard tissue testing after tissue dx)). Turnaround: plasma rate: 7% (days) vs. 6-9% (IQR). Turnaround: tissue NGS rate: 23% (days) vs. 18-28% (IQR). Advanced nonsquamous NSCLC (n=90) rate: 23% (% started targeted therapy pre-tissue NGS) vs. 12% (% actionable alterations found ONLY via plasma). Single-group nonrandomized clinical trial, N=150 enrolled July 2021 – November 2022 at Princess Margaret Cancer Centre (Toronto). Of 150 enrolled: 60% (n=90) had advanced nonsquamous NSCLC (primary analysis cohort). Intervention: plasma ctDNA NGS testing BEFORE tissue biopsy. Median time to treatment: ACCELERATE cohort 39 days (IQR 27-52) vs. reference cohort 62 days (IQR 44-82), P<0.001 — 23-day reduction. Plasma turnaround 7 days vs. tissue NGS 23 days. Of 90 advanced nonsquamous NSCLC patients: 21 (23%) started targeted therapy BEFORE tissue NGS available; 11 (12%) had actionable alterations identified ONLY via plasma testing. García-Pardo et al., JAMA Netw Open 2023;6(7):e2325332.
Survival was not a primary endpoint of ACCELERATE. Key operational outcomes: 23-day faster treatment initiation with upfront plasma testing. 12% of patients had actionable alterations identified ONLY through plasma — these patients would have been missed by tissue-only testing. Supports workflow integration of liquid biopsy at referral, parallel to tissue biopsy pathway.
Diagnostic workflow trial — no therapeutic intervention safety endpoints.
✅ Positive: Upfront plasma ctDNA genotyping cuts time-to-treatment by 23 days in suspected advanced NSCLC. ACCELERATE validates a workflow change in advanced NSCLC diagnosis: plasma ctDNA testing at referral (before tissue biopsy confirmation) gets patients to treatment 23 days faster and catches actionable alterations (12%) that tissue-only testing would have missed. Implementation requires coordinated referral-to-oncology pathway with liquid biopsy at point of entry. Complements established tissue NGS in the hybrid testing paradigm. Expanding adoption of this model could accelerate targeted therapy initiation across thoracic oncology practice, especially in EGFR/ALK/ROS1/KRAS G12C/MET/BRAF/HER2/RET/NTRK-eligible patients.
ACCELERATE (NCT04863924) is a prospective observational study from the University Health Network / Princess Margaret Cancer Centre in Toronto. It tested whether performing plasma circulating-tumor-DNA (ctDNA) genotyping (InVisionFirst-Lung) at the time of referral - before tissue diagnosis - speeds up the lung-cancer diagnostic pathway for patients with suspected advanced NSCLC. It is a diagnostic-workflow study, not a drug trial.
Upfront plasma ctDNA genotyping cut the median time from referral to treatment initiation from 62 days (standard tissue-first testing) to 39 days - 23 days faster. In addition, 12% of patients had actionable genomic alterations identified only through the plasma test, alterations that a tissue-only pathway would have missed or delayed.
No. ACCELERATE is an observational diagnostic-workflow study, not a drug-registration trial. It evaluates a testing strategy (plasma ctDNA genotyping) rather than a therapeutic, so no new drug is approved through this study.
ACCELERATE supports moving molecular testing earlier in the pathway: ordering plasma ctDNA genotyping at referral - before or alongside tissue biopsy - can identify targetable alterations sooner and get patients to appropriate targeted therapy about three weeks faster, addressing a well-recognized bottleneck in advanced-NSCLC care.
ACCELERATE used the InVisionFirst-Lung plasma ctDNA next-generation-sequencing assay (Inivata). Because this is a diagnostic test rather than a therapeutic, ACCELERATE reports operational and molecular-yield outcomes - time to treatment and detection of actionable alterations - rather than drug-efficacy or safety endpoints.