Transplant-ineligible NDMM - Janssen
Discover KOL Sentiment on CEPHEUS →















Top 10 by impressions - click to view on X
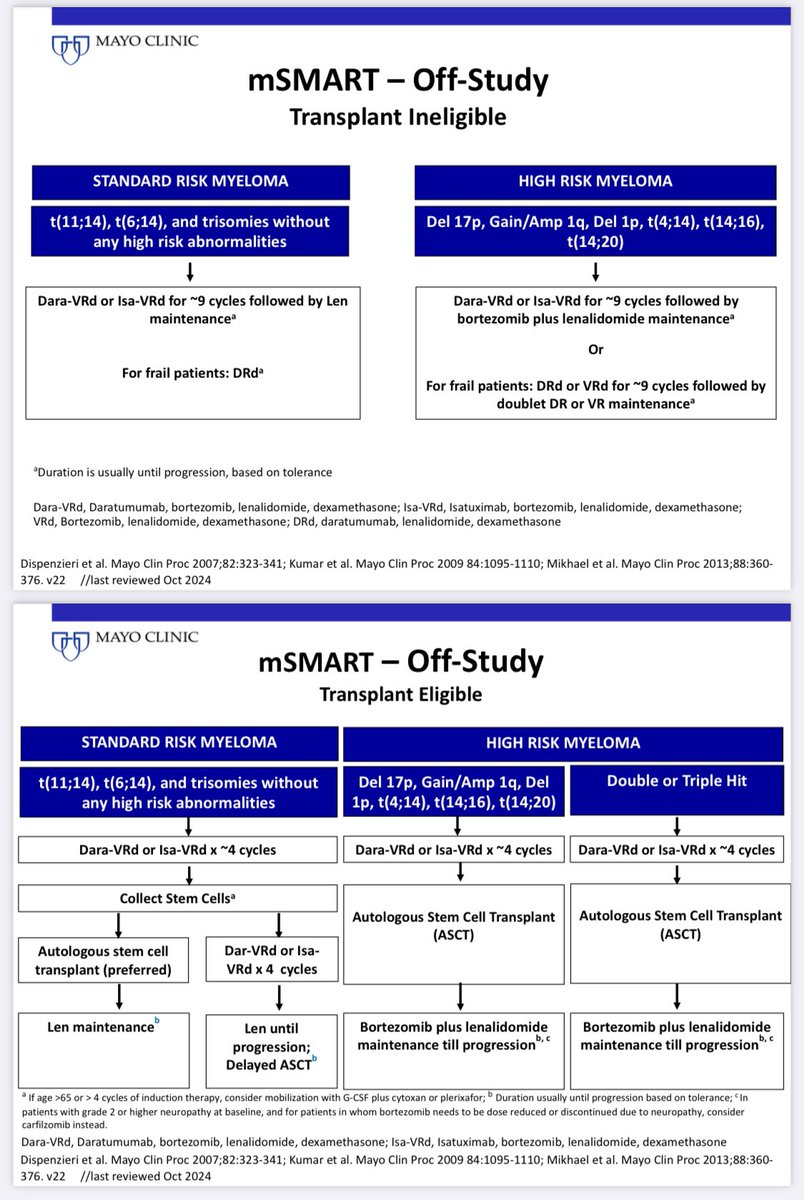
Just out: mSMART Updated guidelines for newly diagnosed myeloma. Main Change: We recommend quadruplets as initial therapy for all newly diagnosed patients who are not frail. Update based on IMROZ,...
Just out: Results of the CEPHEUS trial presented by @szusmani @MSKCancerCenter at the Plenary Session @Myeloma_Society Significant improvement in PFS with Dara-VRd...
CEPHEUS out! 👏 @szusmani et al. PFS ⬆️ ⬆️ with quad in ø ASCT #MMsm. Nice discussion of similarities (many) & differences (few) vs IMROZ. 📢 CD38-VRd now the norm...
CEPHEUS supports use of quads as initial therapy in transplant ineligible patients who are not frail, complementing data from the IMROZ trial which used Isatuximab-VRd.
CEPHEUS presented by @szusmani at #IMS24: Dara-VRd vs VRd in transplant deferred patients with myeloma. 🥇endpoint: MRD neg + CR as best response 👵👴Over 50% patients aged...

President’s address #IMS2025: Impressive projected #PFS 8.3. Years!! #mmsm #multiple #myeloma

@BonumCe @BloodCancerCME @Global_CME @RahulBanerjeeMD @PlasmaCellPete @SagarLonialMD @DoctorAKrishnan @NoopurRajeMD...

In the phase 3 CEPHEUS trial, patients with multiple myeloma were treated with subcutaneous daratumumab plus bortezomib, lenalidomide and dexamethasone, which led to a deeper and more durable...

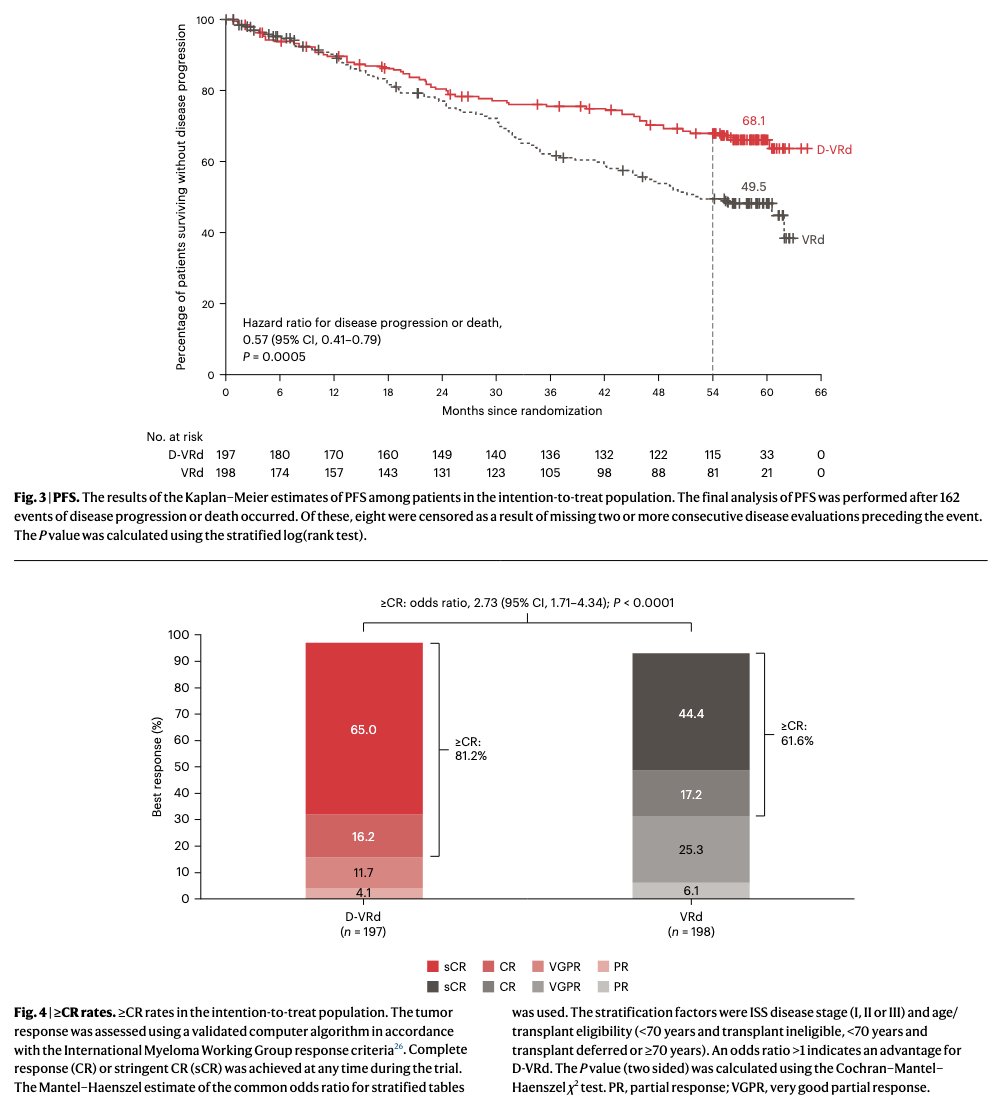
#Myeloma Paper of the Day: Phase 3 CEPHEUS study of Dara+VRd vs. VRd finds MRD-negativity 60.9% for quad vs. 39.4% w/ VRd; ≥CR rates 81.2% vs. 61.6%; sustained MRD negativity (≥12...
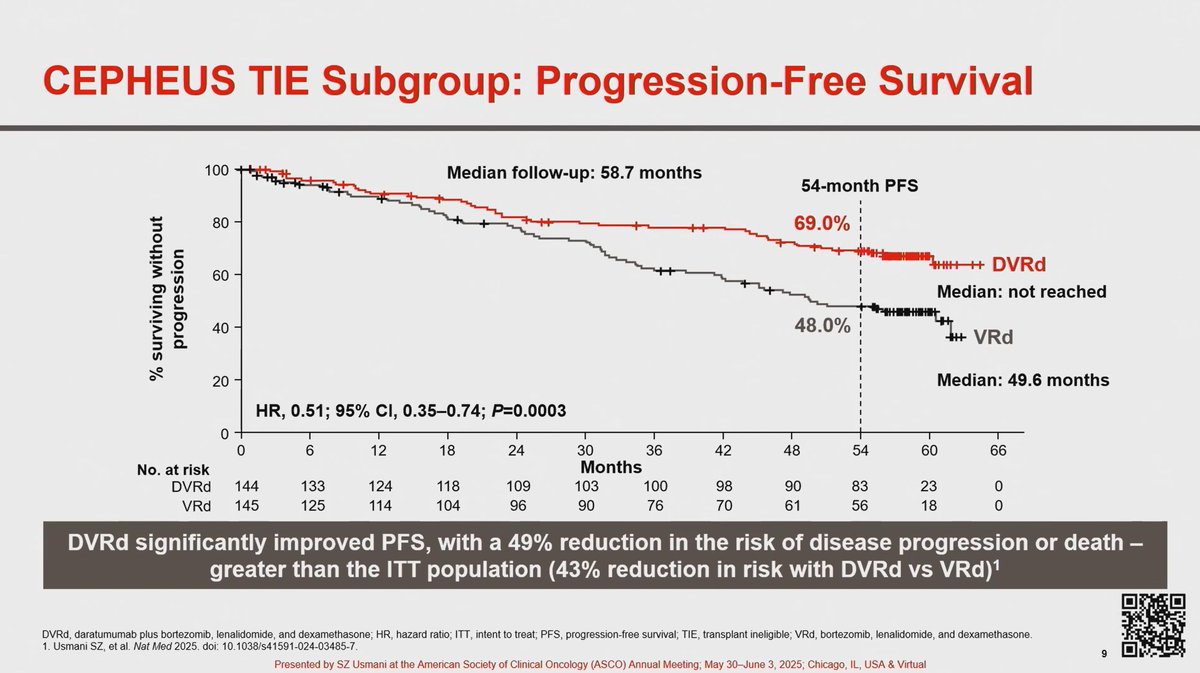
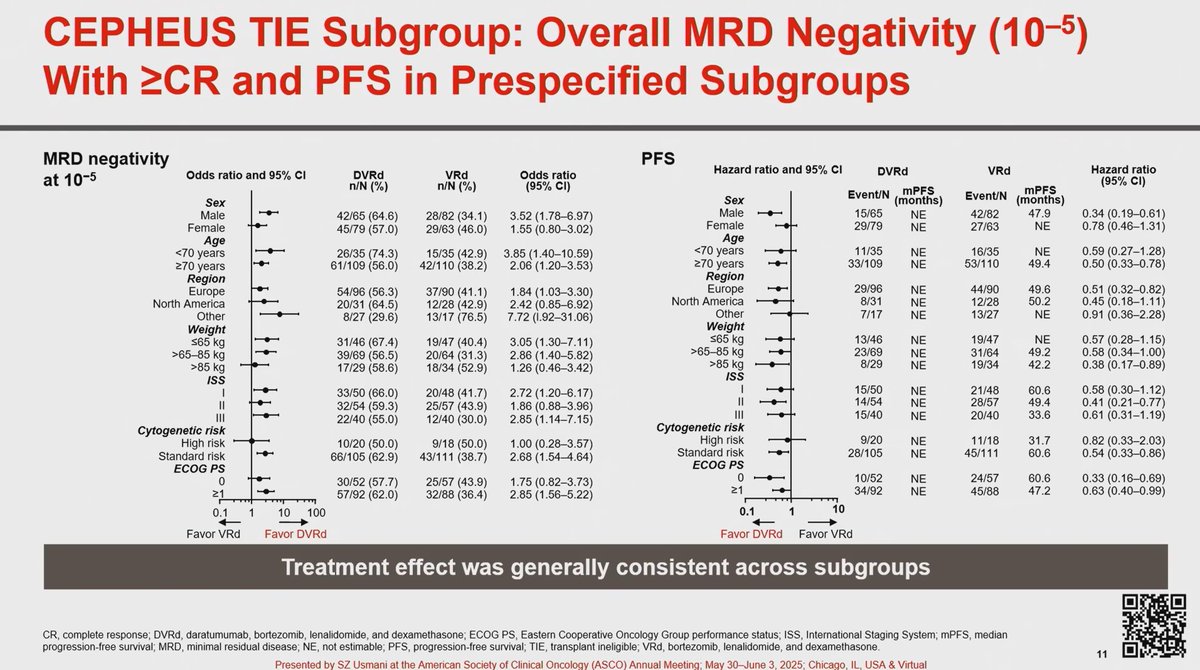
CONGRESS | #ASCO25 | Saad Usmani @szusmani @MSKCancerCenter shared a subgroup analysis of transplant-ineligible patients with NDMM treated with DVRd in the phase...
CEPHEUS is a Phase III, open-label, multicenter, randomized trial evaluating the addition of subcutaneous daratumumab (Darzalex Faspro) to bortezomib, lenalidomide, and dexamethasone (D-VRd) versus VRd alone in patients with transplant-ineligible or transplant-deferred newly diagnosed multiple myeloma. The trial enrolled 395 patients and demonstrated that the D-VRd quadruplet significantly improved MRD negativity rates, depth of response, and progression-free survival. Together with PERSEUS, CEPHEUS establishes D-VRd as a new standard of care for NDMM regardless of transplant eligibility.
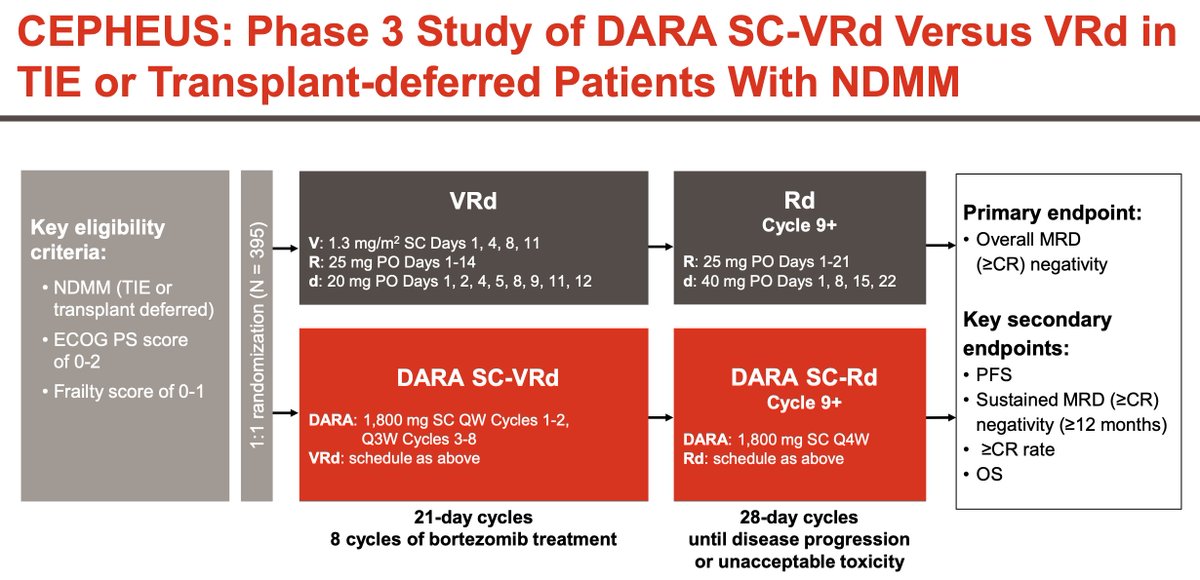
Phase III, open-label, 1:1 randomized, multicenter trial (NCT03652064). Patients received 8 cycles of D-VRd or VRd induction/consolidation (21-day cycles with bortezomib), followed by D-Rd or Rd maintenance (28-day cycles) until progression or unacceptable toxicity. Stratified by ISS stage and age/transplant eligibility (<70 years ineligible, <70 years deferred, and 70 years or older).
Adults with transplant-ineligible or transplant-deferred NDMM, ECOG PS 0-2, IMWG frailty score 0-1. Bortezomib dosed at 1.3 mg/m2 SC on days 1, 4, 8, 11 during induction cycles 1-8. Lenalidomide 25 mg PO days 1-14 during induction, 25 mg days 1-21 during maintenance. Daratumumab SC 1,800 mg weekly cycles 1-2, every 3 weeks cycles 3-8, every 4 weeks during maintenance.
Arm A: Darzalex Faspro + bortezomib + lenalidomide + dexamethasone (D-VRd) for 8 induction cycles, then D-Rd maintenance. Arm B: VRd for 8 cycles, then Rd maintenance. Treatment until progression or unacceptable toxicity.
Primary endpoint: overall MRD negativity rate (with CR or better) at 10-5 by NGS. Key secondary endpoints: PFS by independent review committee, CR or better rate, sustained MRD negativity (12 and 24 months), OS, and safety.
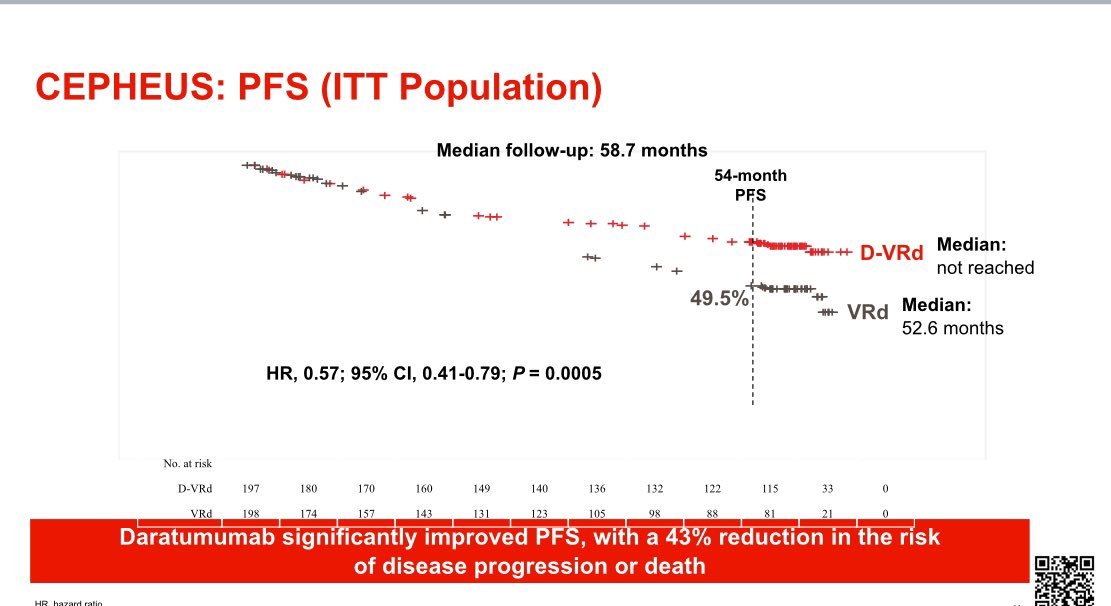
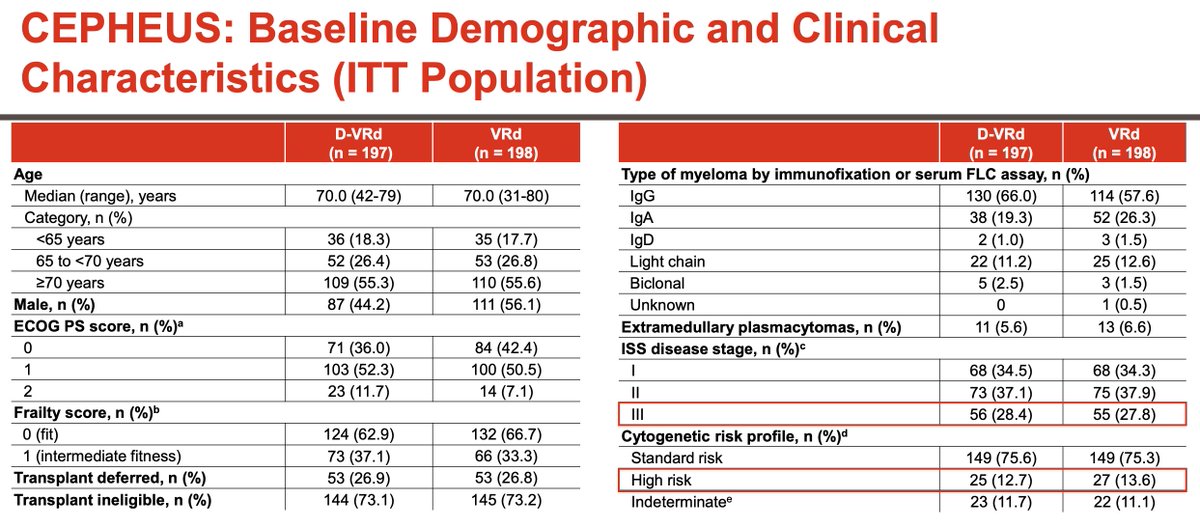
At the final PFS analysis (median follow-up 58.7 months), D-VRd demonstrated a significant PFS benefit with HR 0.57 (95% CI 0.41-0.79; p=0.0005), representing a 43% reduction in disease progression or death. MRD negativity was 60.9% vs 39.4% (OR 2.37; p<0.0001). CR or better rate was 81.2% vs 61.6% (p<0.0001). Sustained MRD negativity at 12 months was 48.7% vs 26.3% (p<0.0001). In the TIE subgroup, PFS HR was 0.51 (95% CI 0.35-0.74; p=0.0003) with median PFS NR vs 49.6 months. FDA-assessed efficacy: MRD negativity 52.3% vs 34.8% (p=0.0005); PFS HR 0.60 (95% CI 0.41-0.88; p=0.0078).
Overall survival data are immature but show a trend favoring D-VRd with OS HR 0.66. When adjusting for COVID-19 deaths, the trend strengthens to HR 0.55. In the TIE subgroup, total deaths were lower with D-VRd (22.9%) than VRd (32.4%), with exposure-adjusted grade 5 TEAE rates similar between arms (0.27 vs 0.31 per 100 patient-months).
Grade 3/4 neutropenia was higher with D-VRd (44.2% vs 29.7%). Thrombocytopenia G3/4: 28.4% vs 20.0%. Peripheral neuropathy G3/4: comparable at 11.2% vs 10.8%. Pneumonia G3/4: 13.9% vs 12.0%. COVID-19 G3/4: 9.7% vs 3.5% (G5 COVID: 4.2% vs 0.7%). SAEs: 72.2% vs 69.7%. Notably, treatment discontinuation due to AEs was lower with D-VRd (7.6%) than VRd (15.9%), likely reflecting the PFS benefit keeping patients on therapy longer.
CEPHEUS establishes D-VRd as the standard of care for transplant-ineligible NDMM, complementing PERSEUS data in the transplant-eligible setting. The FDA approved Darzalex Faspro + VRd for TI-NDMM on January 27, 2026, based on these results. Key clinical debates include whether weekly vs twice-weekly bortezomib dosing (as increasingly used in real-world practice) maintains comparable efficacy, management of frail/elderly patients who may not tolerate the quadruplet, and whether MRD-guided treatment discontinuation could reduce treatment burden while maintaining outcomes.