CheckMate-9ER (NCT03141177) is a Phase 3 trial of nivolumab (Opdivo) plus cabozantinib (Cabometyx) versus sunitinib in previously untreated advanced clear cell renal cell carcinoma. The combination doubled median progression-free survival (16.6 vs 8.3 months; HR 0.51) and improved overall survival (final 5.5-year median 46.5 vs 35.5 months; HR 0.79). It is FDA approved as a first-line regimen. Sponsors: Bristol Myers Squibb and Exelixis.
Discover KOL Sentiment on CheckMate-9ER →Design — Phase 3, randomized, open-label; nivolumab (Opdivo) + cabozantinib (Cabometyx) vs sunitinib, 651 previously untreated advanced clear cell RCC across all IMDC risk groups (NCT03141177). (NEJM 2021; ASCO GU 2025 final)
PFS (primary) — Median 16.6 vs 8.3 months (HR 0.51; 95% CI 0.41-0.64) — roughly doubled versus sunitinib. (NEJM 2021)
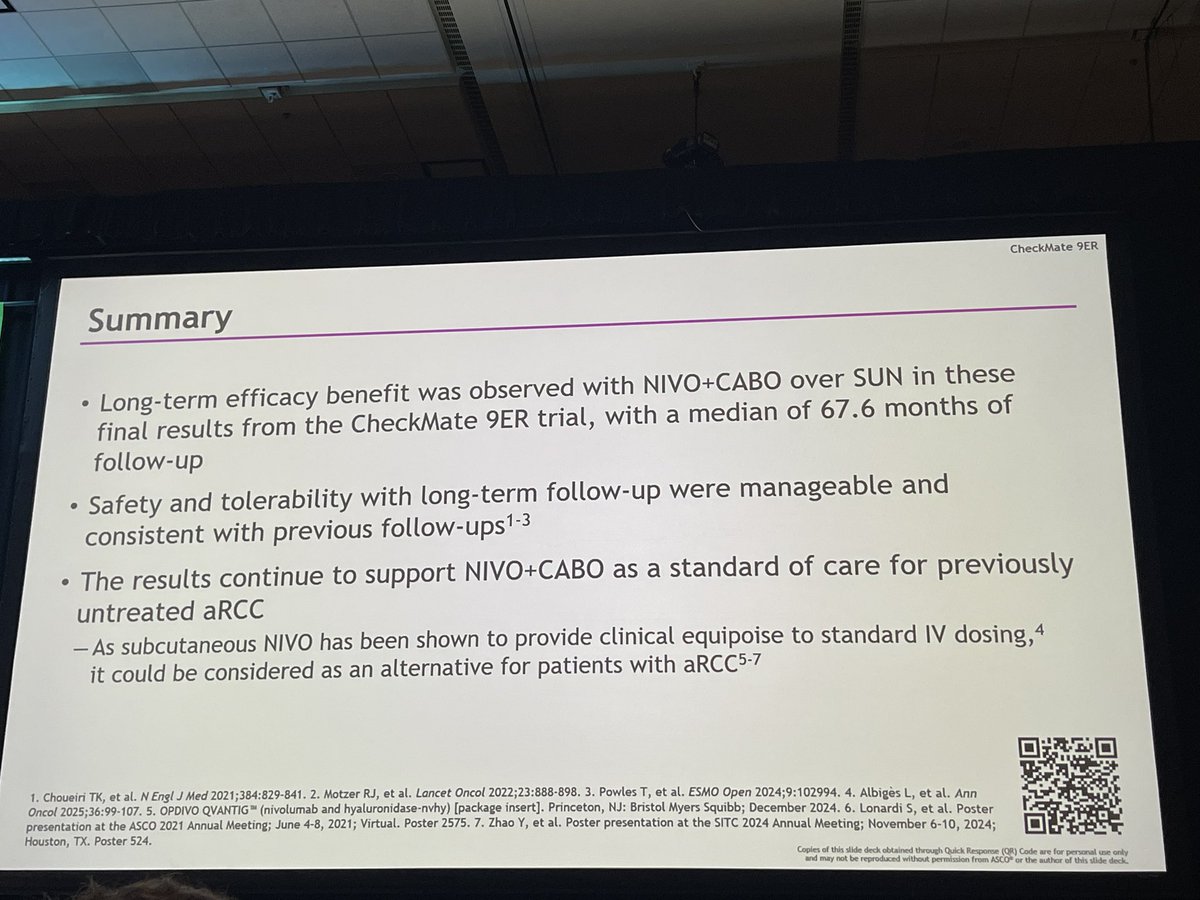
Overall survival — Primary-analysis OS HR 0.60 (98.89% CI 0.40-0.89); final 5.5-year median OS 46.5 vs 35.5 months (HR 0.79; 95% CI 0.65-0.96); 60-month OS 40.9% vs 35.4%. (ASCO GU 2025)
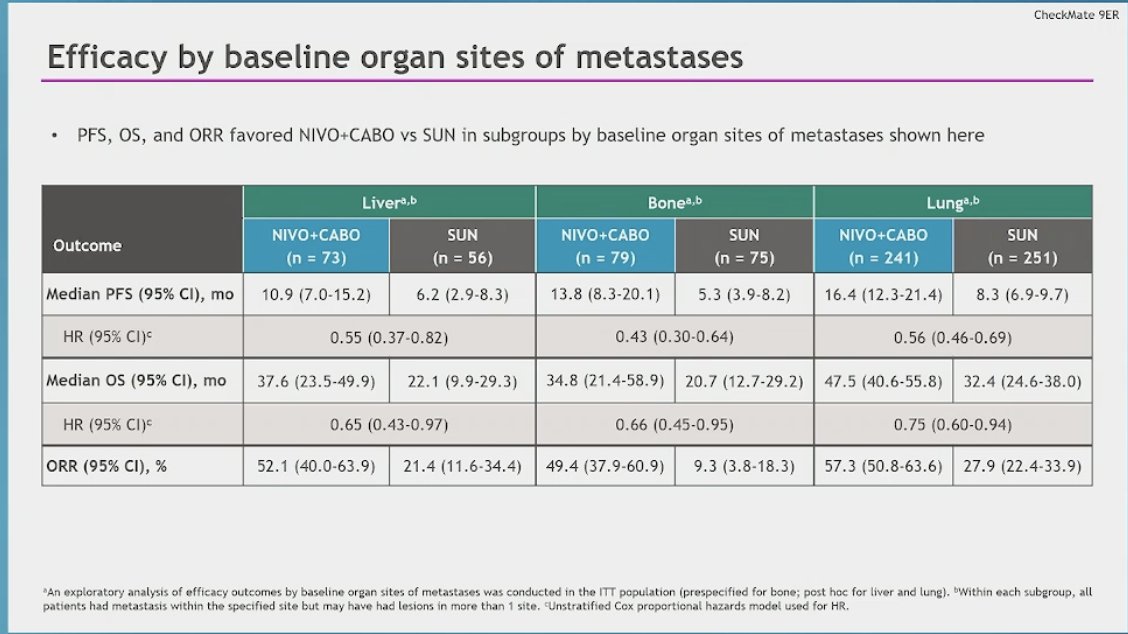
Subgroup — OS benefit not observed in the favorable-risk subgroup at final follow-up; benefit driven by intermediate/poor-risk disease. (ASCO GU 2025)
Safety — Grade 3/4 treatment-related AEs 60.6% vs 50.9%; AE discontinuation 15.3% vs 8.8%; common events diarrhea, hypertension, hepatotoxicity. (NEJM 2021, primary analysis / label)
Regulatory / Sponsor — FDA APPROVED January 2021 — Opdivo + Cabometyx, first-line advanced RCC. Bristol Myers Squibb and Exelixis. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.















Top 10 by impressions -- click to view on X
Final #CheckMate9ER results (5+ yr FU: N+C > S in 1L #aRCC PFS HR 0.58, OS HR 0.79, ORR 55.7% vs 27.4%. No new safety signals. N+C remains a SOC for untreated aRCC. @ASCO #GU25 @motzermd @tompowles1 @MSKCancerCenter @OncoAlert
Congrats to @DrChoueiri @motzermd for developing one of the most effective combinations cabozantinib + nivolumab for mRCC #kidneycancer Checkmate 9ER phase 3 trial continued strong OS benefit @tompowles1 @AlbigesL @asco #GU25
5 year update of checkmate 9ER. Nivo plus Cabo vs Sunitinib for advanced clear cell RCC. Note that Sunitinib arm is not doing bad either. 35.4 % are alive on Sunitinib arm also at the end of 5 years. ( vs 40.9 % on nivo plus Cabo arm ) gap between two has narrowed . Any views
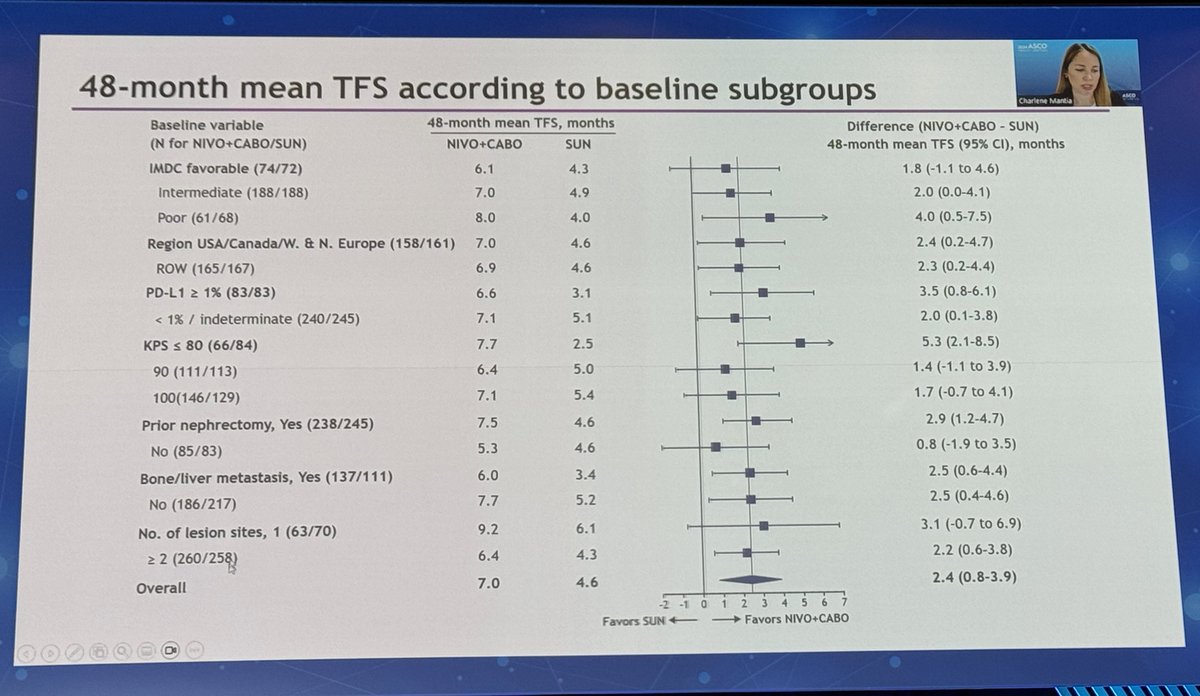
Excellent analysis by our very own @CharleneMantia of survival states over 4 years in #CheckMate9ER comparing 1L Nivo + Cabo vs. Sun in pts w/ aRCC! #ASCO24 Over the 4-year period since initiation of 1L therapy, the longer OS with Nivo+Cabo was accompanied by 1.5 times
Final analysis of Checkmate 9ER in @Annals_Oncology : 1L mRCC trial
Ab#439 @ASCO #GU25 by #RobertMotzer Final results of CheckMate 9ER #kidneycancer Median OS 46.5 vs 35.5 mo w/ 1L Cabo+Nivo vs sunitinib @DrChoueiri @OncoAlert @urotoday @KidneyCancer @Uromigos @kidneycan
CheckMate 9ER: 5-Year Final Analysis Nivo + Cabo (N+C) outperforms Sunitinib (S) in 1L aRCC PFS: 16.4 vs 8.3 mo OS: 46.5 vs 35.5 mo ORR: 56% vs 27%, CR: 14% vs 5% @motzermd @MSKCancerCenter #GU25 @asco #kidneycancer
@ASCO #GU25 | Abstract #439 Presented by: @motzermd Key authors: @tompowles1, @DrChoueiri @OncoAlert Final 5-year results from CheckMate 9ER: PFS: 16.4 vs. 8.3 months (HR 0.58, 95% CI 0.49-0.70) OS: 46.5 vs. 35.5 months (HR 0.79, 95% CI 0.65-0.96)
@ASCO #GU25: CheckMate 9ER (5+ year follow-up): Nivolumab + Cabozantinib continues to show durable efficacy in 1L advanced RCC vs. Sunitinib. No new safety signal! @motzermd @ASCOPost @ASCOTECAG @OncoAlert

Final updates of #CheckMate 9ER trial? nivolumab + cabozantinib vs sunitinib in 1L advanced RCC @ASCO #GU25 Key Takeaways, nivolumab with cabozantinib: Improved PFS in ITT 16.4m vs 8.3m HR 0.58 Improved OS in ITT 46.5m vs 35.5m HR 0.79 Doubled ORR 55.7% vs 27.4%
CheckMate-9ER is a phase 3, randomized, open-label trial evaluating nivolumab (Opdivo) plus cabozantinib (Cabometyx) versus sunitinib in 651 previously untreated patients with advanced clear cell renal cell carcinoma across all IMDC risk groups. The combination demonstrated statistically significant improvements in PFS, OS, and ORR compared to sunitinib, leading to FDA approval in January 2021. Final 5.5-year follow-up data presented at ASCO GU 2025 confirm durable benefit with median PFS of 16.6 vs 8.3 months (HR 0.58) and median OS of 46.5 vs 35.5 months (HR 0.79), establishing nivo+cabo as a standard of care for first-line advanced RCC.
CheckMate-9ER (NCT03141177) is a Phase 3, randomized, open-label trial evaluating nivolumab (Opdivo) plus cabozantinib (Cabometyx) versus sunitinib in 651 previously untreated patients with advanced clear cell renal cell carcinoma across all IMDC risk groups. It was sponsored by Bristol Myers Squibb and Exelixis (with Ono Pharmaceutical).
Nivolumab plus cabozantinib doubled median progression-free survival to 16.6 versus 8.3 months (HR 0.51) and improved overall survival (primary-analysis HR 0.60; final 5.5-year median OS 46.5 vs 35.5 months, HR 0.79) versus sunitinib, along with a higher objective response rate. Final follow-up at ASCO GU 2025 confirmed durable long-term benefit.
Yes. Nivolumab (Opdivo) in combination with cabozantinib (Cabometyx) was FDA approved in January 2021 for the first-line treatment of advanced renal cell carcinoma, based on the CheckMate-9ER trial. It is a National Comprehensive Cancer Network Category 1 preferred first-line regimen.
Nivolumab plus cabozantinib is one of several immunotherapy-plus-tyrosine-kinase-inhibitor combinations used first-line in advanced RCC, alongside lenvatinib plus pembrolizumab (CLEAR / KEYNOTE-581) and pembrolizumab plus axitinib (KEYNOTE-426). Cross-trial comparisons are limited by differing populations; all are considered standard first-line options.
Grade 3 or 4 treatment-related adverse events occurred in about 60.6% of patients on the combination versus 50.9% with sunitinib, and treatment discontinuation due to adverse events was higher (15.3% vs 8.8%). Common events included diarrhea, hypertension and hepatotoxicity (ALT/AST elevation), generally managed with dose modification of cabozantinib.
Phase 3, randomized 1:1, open-label trial. Stratified by IMDC risk score, tumor PD-L1 expression, and geographic region. Median follow-up 67.6 months (final analysis).
651 previously untreated patients with advanced or metastatic clear cell RCC across all IMDC risk groups (favorable, intermediate, and poor).
Nivolumab 240 mg IV Q2W + cabozantinib 40 mg PO daily vs sunitinib 50 mg PO daily (4 weeks on / 2 weeks off). Treatment until progression or unacceptable toxicity.
PFS per BICR (RECIST v1.1). Key secondary: OS, ORR per BICR, and safety.
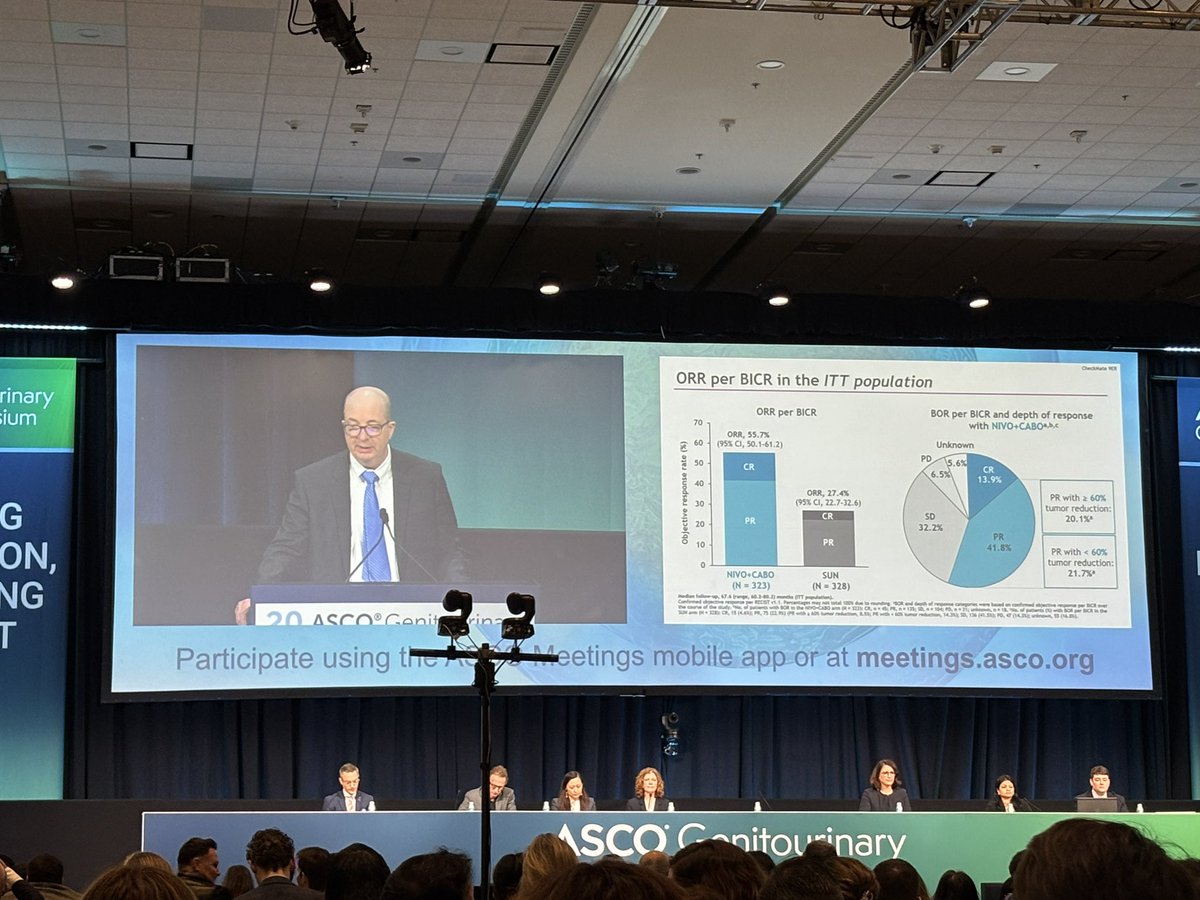
Nivolumab + cabozantinib doubled median PFS compared to sunitinib: 16.6 months vs 8.3 months (HR 0.51, 95% CI: 0.41-0.64, p<0.0001). At the final 5.5-year analysis, the PFS benefit remained durable with HR 0.58 (95% CI: 0.49-0.70). ORR was 55.7% vs 27.1-27.4%, with complete response rates of 13.9% vs 4.6%. Median duration of response was 22.0 vs 15.2 months.
At primary analysis, OS HR was 0.60 (98.89% CI: 0.40-0.89, p=0.001) favoring nivolumab + cabozantinib. Final 5.5-year follow-up showed median OS of 46.5 vs 35.5 months (HR 0.79, 95% CI: 0.65-0.96). The 60-month OS rates were 40.9% vs 35.4%. Notably, in the favorable-risk subgroup, no OS benefit was observed (53.7 vs 58.9 months, HR 1.08), a finding that continues to be debated among KOLs.
Grade 3/4 treatment-related adverse events occurred in 60.6% of the nivo+cabo arm vs 50.9% with sunitinib. Treatment discontinuation due to adverse events was higher with the combination (15.3% vs 8.8%). Common adverse events included diarrhea, hypertension, and hepatotoxicity (ALT/AST elevation). Safety was manageable with dose modifications, and no new safety signals emerged at 5.5-year follow-up. The cabozantinib dose was reduced to 40 mg (from standard 60 mg) when combined with nivolumab.
CheckMate-9ER final data confirm nivolumab + cabozantinib as a durable first-line standard of care for advanced RCC (NCCN Category 1 preferred). The combination is one of several IO-TKI options competing in 1L RCC, alongside CLEAR (lenvatinib + pembrolizumab) and KEYNOTE-426 (pembrolizumab + axitinib). Treatment selection depends on risk group, toxicity profile, and physician preference. The favorable-risk debate -- whether IO-TKI is needed over TKI monotherapy -- remains an active area of discussion among GU oncology KOLs.