Women ≥70 years old with stage I luminal A-like early breast cancer after breast-conserving surgery — Fondazione Radioterapia Oncologica (Italian academic consortium; 17 Italian + 1 Slovenian center)
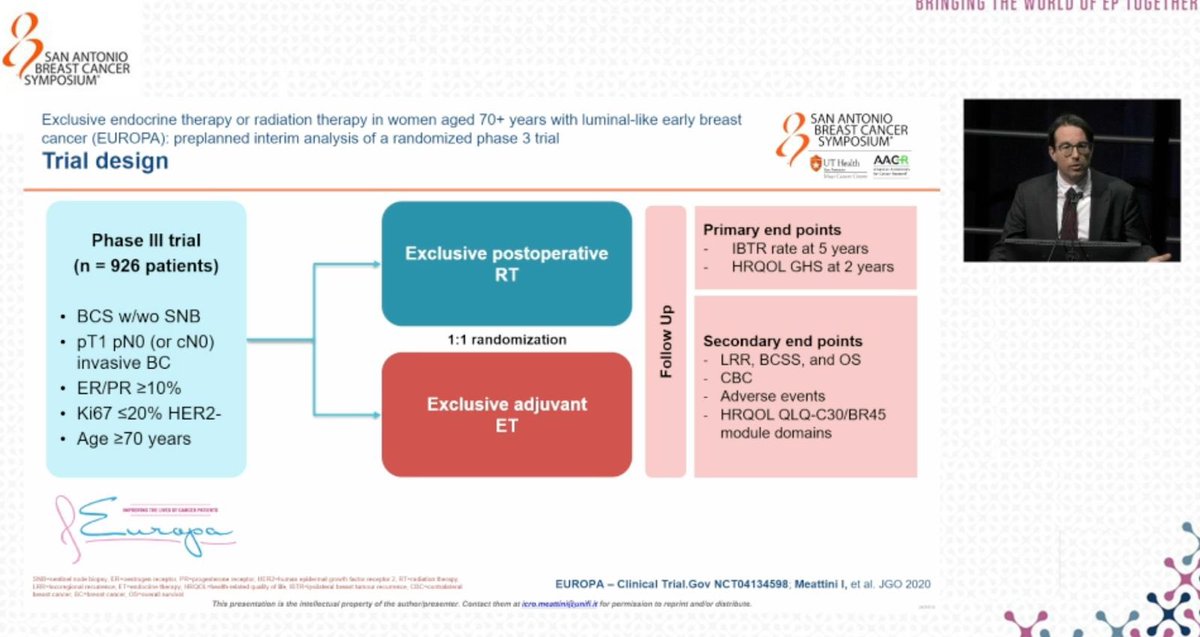
Discover KOL Sentiment on EUROPA →Design - Phase 3 academic randomized trial: postoperative radiotherapy alone vs adjuvant endocrine therapy alone, women >=70y with stage I luminal A-like BC after breast-conserving surgery (NCT04134598).
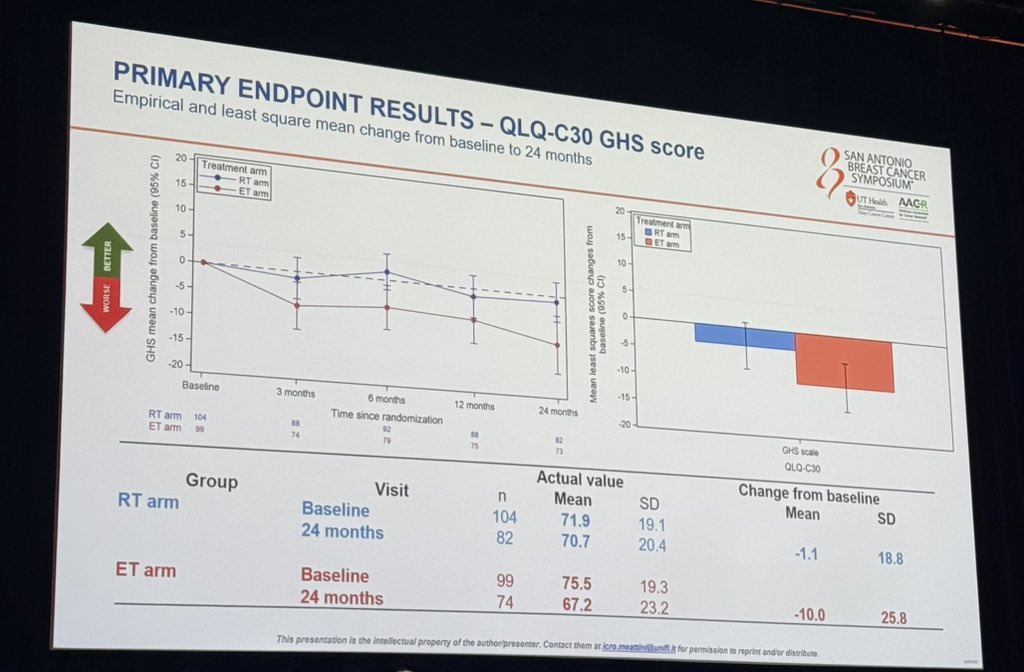
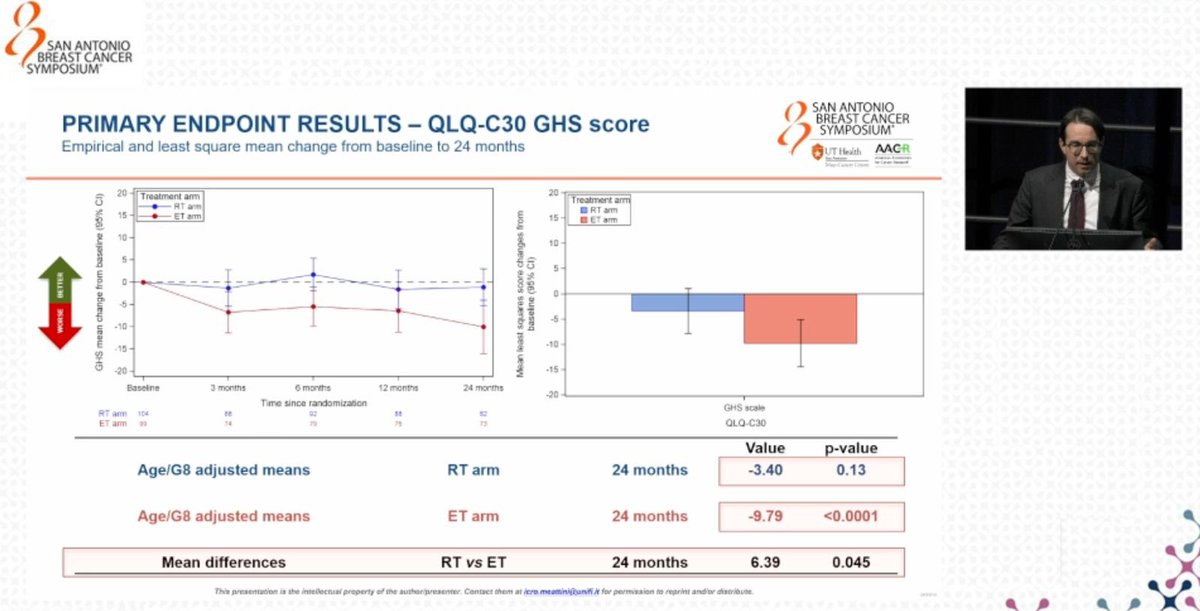
HRQoL (co-primary, 24 mo) - Global health status better preserved with radiotherapy: adjusted mean change -3.4 (RT) vs -9.79 (endocrine therapy); between-arm difference favored RT (GHS difference reported 6.39, P=0.045).
Recurrence / OS - At 24 months, no ipsilateral breast tumor recurrence, locoregional relapse, or breast-cancer deaths in either arm; deaths during follow-up (4 RT, 2 ET) were not breast-cancer related. 5-year IBTR co-primary endpoint pending.
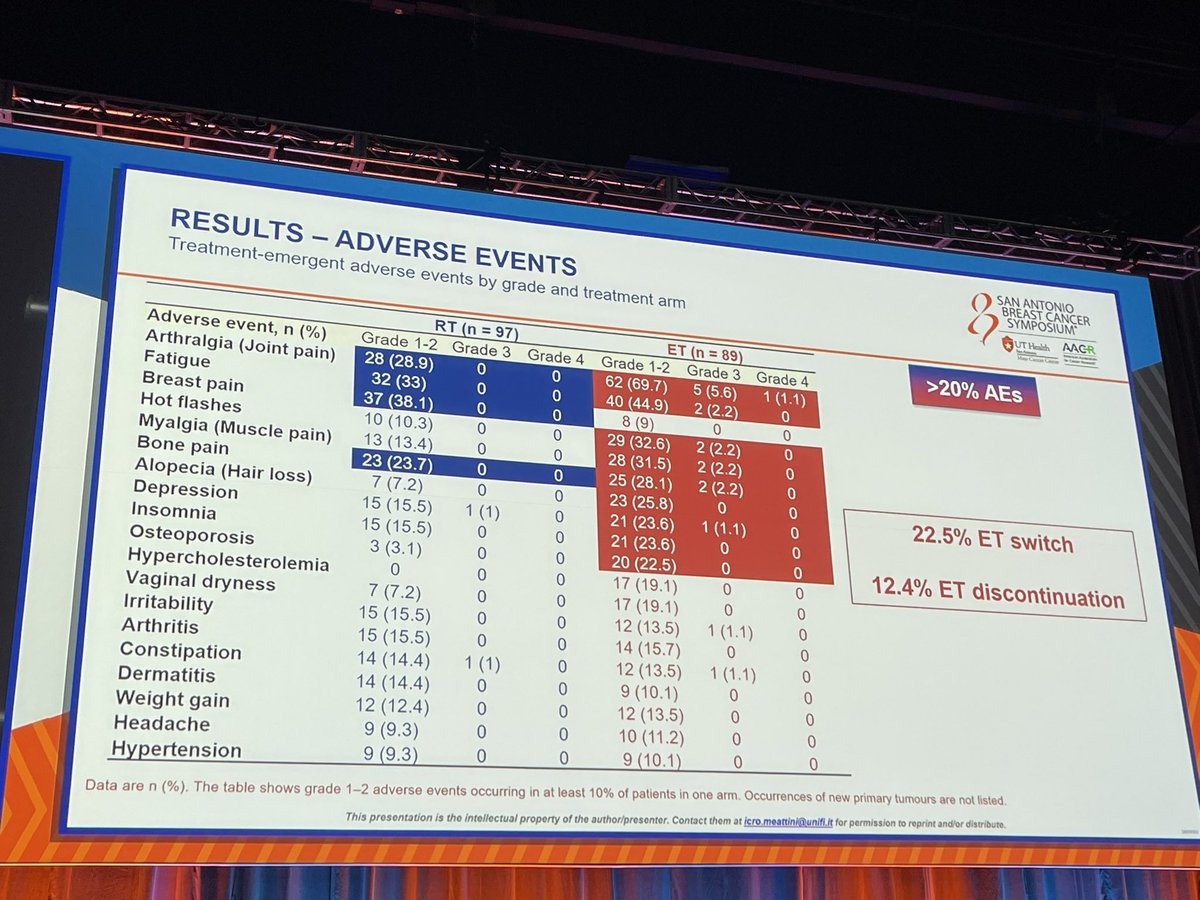
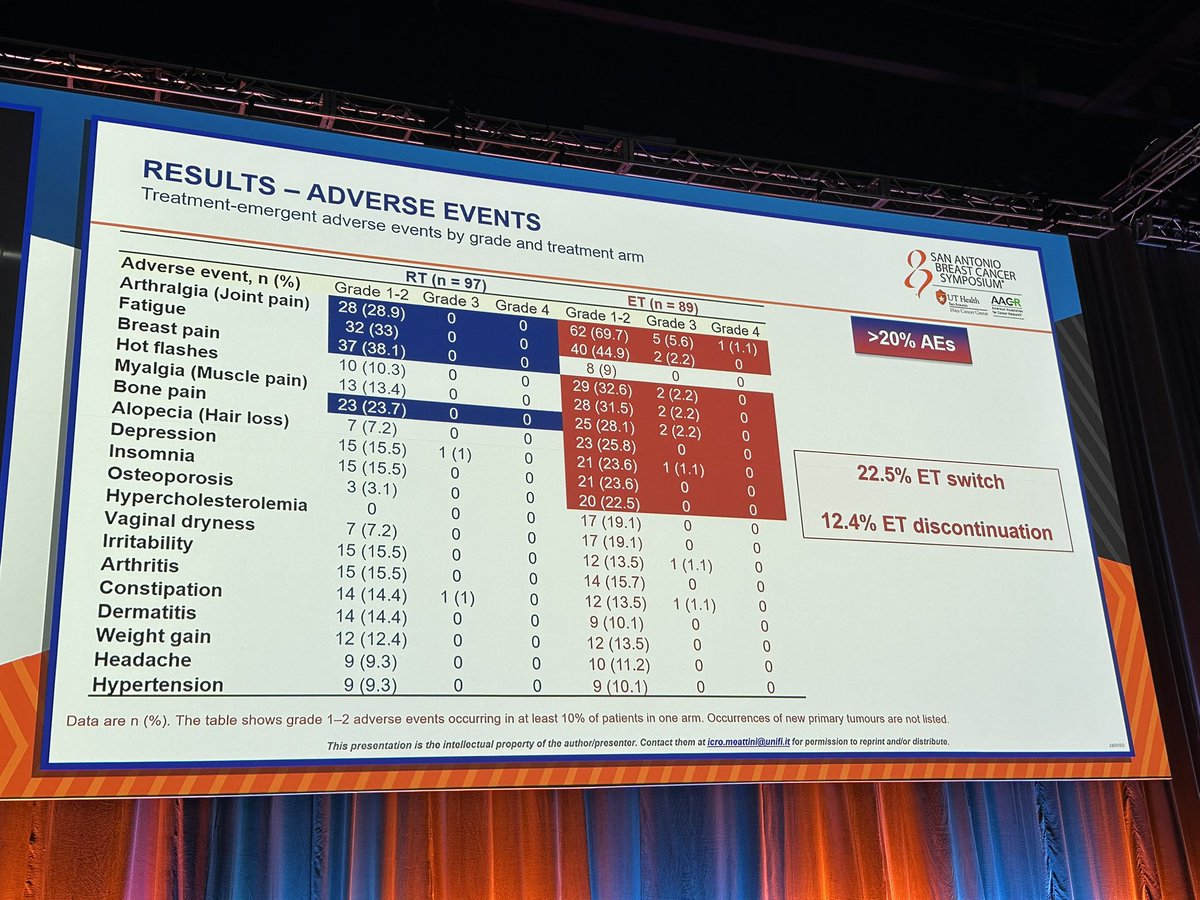
Safety - Grade >=3 adverse events 67.0% (RT) vs 85.4% (endocrine therapy); discontinuation due to AEs 0% (RT) vs 12.4% (ET).
Regulatory - Investigational/academic single-modality de-escalation strategy; not an FDA drug-registration trial.
Sponsor - Fondazione Radioterapia Oncologica / Careggi (Italian academic consortium).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.











Top tweets by impressions — click to view on X
‼️ EUROPA interim
Ph3 RCT 70+ y/o low risk breast cancer -> BCS -> adjuvant endocrine only vs adjuvant APBI only
APBI has better HRQoL than endocrine tx, adj mean difference 6.39…
#SABCS24 Part 2: Highlights w/ @jamecancerdoc
✅ #EUROPA
✅ #TAILORx
✅ #PADMA
✅ #EMBER3
Full 📢:
⭐️ https://t.co/26pwXj5j8g
⭐️ https://t.co/jc9mu7uaBn
⭐️Also on “Oncology Brothers”…
Why every one is behind to stop RT ? Is it that toxic even With newer technology? Non Inferiority trials are flooding RT . I am very curious. 🤔 @5_utr @NiuSanford @KrishanJethwa @dr_yakupergun…
The interim-analysis of the groundbreaking EUROPA trial demonstrates what we all have been thinking:
⁃Much less AE’s in the RT arm
⁃Better HRQoL preservation in the RT arm
Time for a paradigm shift!…
📌 EUROPA Trial: Exclusive Endocrine Therapy or Radiation Therapy in Women Aged 70+ Years with Luminal-Like Early Breast Cancer: Preplanned Interim Analysis of a Randomized Phase 3 Trial …
At #SABCS24 GS2 opens with the great @Icro_Meattini presenting the awaited data of EUROPA trial, aka exclusive RT vs. ET in 70+ women with LumA eBC👵🏻
RT offers better QoL and less adverse events…

#SABCS24 @Icro_Meattini presents interim analysis of the Europa trial. Older women with stage I lo KI67. HR+ BC Rand to RT vs ET. 24 mo FU. No recurrences yet. RT less toxic, 12% stopped ET. 850…

Presented in general session 2 of #SABCS24 by super @Icro_Meattini 🇮🇹 results of the interim analysis of the #EUROPA trial simultaneously published in @TheLancetOncol…really proud for the chance to…
EUROPA trial is out in Lancet Oncology
Excellent work @Icro_Meattini
https://t.co/jbJiCuXdj7

The #OncoAlertTopTweet 🚨Day THREE #SABCS24
Post by @5_utr
EUROPA interim 🇪🇺
Ph3 RCT 70+ y/o low risk breast cancer -> BCS -> adjuvant endocrine only vs adjuvant APBI only
APBI has better…
EUROPA challenges the assumption that ET is superior to RT as single-modality post-breast-conserving surgery in low-risk older women. At 24 months, RT preserved HRQOL significantly better than ET (adjusted difference 6.39, P=0.045), with substantially lower AE burden (67% vs. 85%) and lower discontinuation. ET was associated with a 22.5% treatment switch rate and 12.4% discontinuation. Both single-modality options showed zero IBTR/relapse/BC-death at 24 months — definitive 5-year IBTR data needed to confirm equivalent disease control. Supports ultra-hypofractionated partial-breast RT (5 fractions) as practical alternative to 5-10 years of daily AI/tamoxifen in elderly patients. Discussant noted PRIME II and CALGB 9343 suggest RT omission is also reasonable.
Median: -3.4 ΔGHS from baseline (radiotherapy alone) vs. -9.79 ΔGHS from baseline (endocrine therapy alone). GHS change RT arm rate: -3.4% (adjusted mean Δ) vs. -7.82 to 1.03% (95% CI). GHS change ET arm rate: -9.79% (adjusted mean Δ) vs. -14.45 to -5.13% (95% CI). Adjusted mean difference rate: 6.39% (favoring RT) vs. 0.14-12.65% (95% CI). Phase 3 non-inferiority trial (N=731 randomized; interim analysis N=207 with median follow-up 23.9 months). Co-primary 1 (HRQOL): adjusted mean change in Global Health Status at 24 months was -3.40 (95% CI -7.82 to 1.03, P=0.13) with RT vs. -9.79 (95% CI -14.45 to -5.13, P<0.0001) with ET — adjusted mean difference 6.39 (95% CI 0.14-12.65, P=0.045) FAVORING RADIOTHERAPY. Co-primary 2 (5-year IBTR): NOT reported at interim. Meattini et al., Lancet Oncol 2025;26(1):37-50.
At 24 months: NO ipsilateral breast tumor recurrence (IBTR), locoregional relapse, or breast cancer-related deaths in either arm. 5-year IBTR co-primary endpoint pending. 4 patients in RT arm and 2 in ET arm died during follow-up; none were breast cancer-related. Final analysis scheduled at 5 years.
Grade ≥3 adverse events: 67.0% (rt) vs. 85.4% (et). Discontinuation due to AEs: 0% (rt) vs. 12.4% (et). Key AEs: RT arm: arthralgia (28.9%), fatigue (33.0%), breast pain (38.1%), bone pain (23.7%), ET arm: arthralgia (69.7%), fatigue (44.9%), hot flashes (32.6%), myalgia (31.5%), bone pain (28.1%), alopecia (25.8%), ET arm Grade ≥3: arthralgia (7%), pelvic organ prolapse (3%). Treatment-related AE rates 67.0% (RT) vs. 85.4% (ET), adjusted difference -18.4 (95% CI -30.2 to -6.2). Within 24 months, 22.5% of ET patients switched to different treatment, 12.4% discontinued ET entirely. Serious AEs 15% vs. 15%. Both arms had 2 fatal TEAEs: RT (esophageal neoplasia, Listeria meningitis); ET (pneumonia, ischemic heart disease). 84.6% of RT patients received partial breast irradiation (5-8 fractions), 15.4% received whole-breast RT.
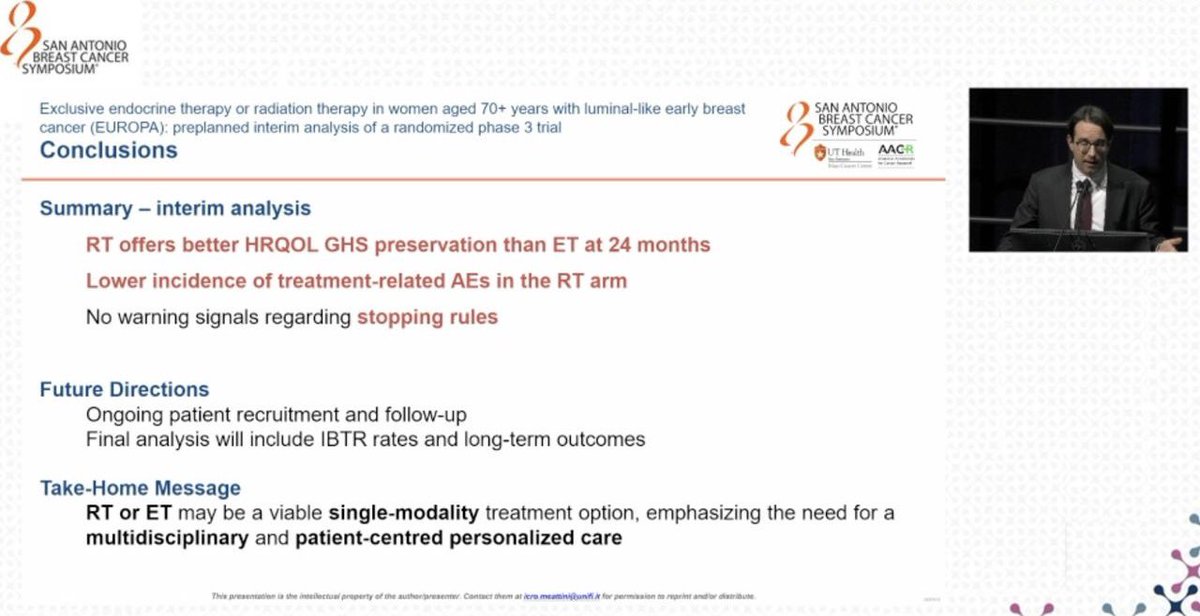
🔄 Interim: radiotherapy better preserves QOL vs. endocrine therapy in 70+ luminal A BC; 5-year IBTR still awaited. EUROPA challenges the assumption that ET is superior to RT as single-modality post-breast-conserving surgery in low-risk older women. At 24 months, RT preserved HRQOL significantly better than ET (adjusted difference 6.39, P=0.045), with substantially lower AE burden (67% vs. 85%) and lower discontinuation. ET was associated with a 22.5% treatment switch rate and 12.4% discontinuation. Both single-modality options showed zero IBTR/relapse/BC-death at 24 months — definitive 5-year IBTR data needed to confirm equivalent disease control. Supports ultra-hypofractionated partial-breast RT (5 fractions) as practical alternative to 5-10 years of daily AI/tamoxifen in elderly patients. Discussant noted PRIME II and CALGB 9343 suggest RT omission is also reasonable.
EUROPA (NCT04134598) is a Phase 3, academic randomized trial from an Italian consortium (Fondazione Radioterapia Oncologica / Careggi) comparing exclusive postoperative radiotherapy alone versus exclusive adjuvant endocrine therapy alone in women aged 70 years or older with stage I luminal A-like early breast cancer after breast-conserving surgery. Its co-primary endpoints are quality of life at 24 months and 5-year ipsilateral breast tumor recurrence.
At 24 months, radiotherapy alone better preserved global health status/quality of life than endocrine therapy alone (adjusted mean change -3.4 versus -9.79). There were no ipsilateral breast tumor recurrences, locoregional relapses, or breast-cancer deaths in either arm at 24 months. The 5-year ipsilateral breast tumor recurrence co-primary endpoint is still awaited.
No. EUROPA is a de-escalation strategy trial that compares two single-treatment approaches - radiotherapy alone versus endocrine therapy alone - after breast-conserving surgery in older women with low-risk disease. It is not an FDA drug-registration study and does not evaluate a new medicine for approval.
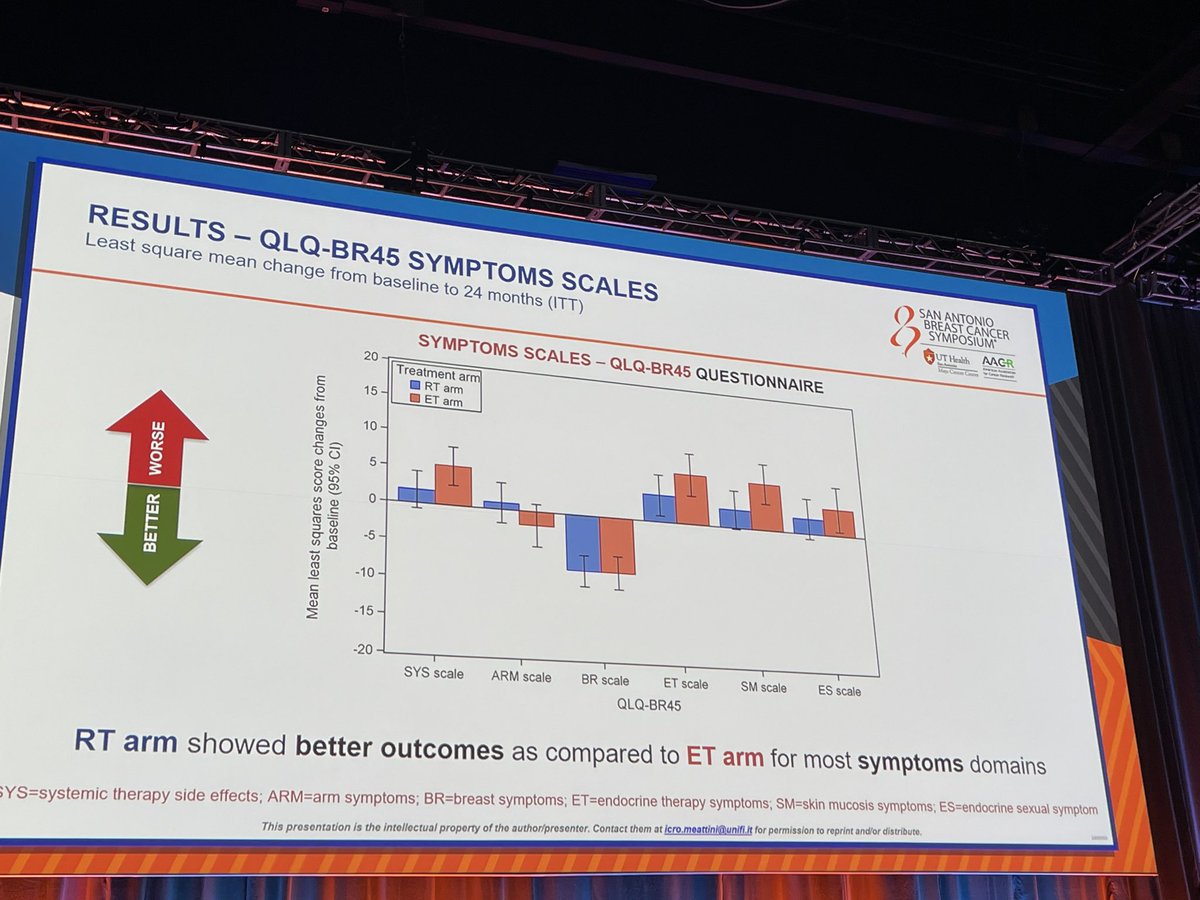
Grade 3 or higher adverse events were less frequent with radiotherapy (67.0%) than with endocrine therapy (85.4%), and no patients discontinued radiotherapy due to adverse events versus 12.4% discontinuing endocrine therapy. Endocrine therapy was associated with more arthralgia, fatigue, hot flashes and myalgia.
EUROPA challenges the assumption that endocrine therapy is preferable to radiotherapy as single-modality treatment after breast-conserving surgery in low-risk older women. Its interim data suggest radiotherapy alone can better preserve quality of life, though the 5-year local recurrence result is needed before firm conclusions.