1L ALK+ metastatic NSCLC - Xcovery/BeiGene
Discover KOL Sentiment on eXalt3 →








Top 10 by impressions - click to view on X
Another ALK inhibitor (#ensartinib) gets @US_FDA approval eXalt3 study: - 1L, Ph III, ALK+ mNSCLC vs Crizotinib - Ensartinib vs crizotinib (NR vs 12.7mos, HR: 0.45) -...
In case you missed it: real progress is happening in ALK+ NSCLC. And we are just getting started. Here’s to what’s next. @myESMO #ELCC26
FDA approves ensartinib for #ALK NSCLC based on phase III eXALT3 trial that compared 1L ensartinib & crizotinib. PFS favored ensartinib (25.8m vs 12.7m, HR 0.56), no OS...
🔥🚨@OncoAlert Hot off the press. @US_FDA approves NEW #ALK inhibitor (#Ensartinib) for 1st line Tx of advanced #ALK+...
The approval was based on the eXALT3 trial, a randomized study comparing ensartinib to crizotinib in 290 patients. Ensartinib significantly improved progression-free survival (PFS) with a median of...
This was presented in 2020. This was published in 2021. It got approval in fag end of 2024. Was @FDAOncology playing monopoly game ? Ensartinib vs Lorlatinib? What will u prefer ? Who...

ICYMI: The US FDA approves ensartinib for ALK-positive NSCLC and provides an updated regulatory review of subcutaneous amivantamab. More updates in ILCN: #LCSM
@US_FDA approves ensartinib for ALK+ NSCLC. Back in 2017, during my time as an intern @VUMCMedicineRes, I co-wrote one of my first oncology review articles on the eXalt3 trial with...

FDA approves ensartinib for ALK-positive locally advanced or metastatic non-small cell lung cancer ✅.

@SuyogCancer @FDAOncology @StephenVLiu data leading to FDA approval have been digitized on see : eXALT3 trial❗️
eXALT3 is a global, open-label, randomized Phase 3 trial that established ensartinib (Ensacove) as a first-line treatment option for patients with ALK-positive locally advanced or metastatic NSCLC. The trial compared ensartinib 225 mg daily to crizotinib 250 mg twice daily in 290 ALK TKI-naive patients and demonstrated a statistically significant improvement in progression-free survival. Ensartinib also showed superior intracranial activity, with a CNS objective response rate nearly three times that of crizotinib, addressing a critical unmet need in ALK-positive NSCLC where brain metastases are common.
Phase 3, global, open-label, 1:1 randomized, active-controlled, multicenter trial comparing ensartinib to crizotinib in ALK TKI-naive patients with locally advanced or metastatic ALK-positive NSCLC. ALK positivity confirmed by FDA-approved Vysis FISH assay. Randomization stratified by prior chemotherapy (0 vs 1), ECOG PS (0/1 vs 2), CNS metastases (yes/no), and geographic region (Asia vs rest of world). Treatment continued in 28-day cycles until progression or unacceptable toxicity.
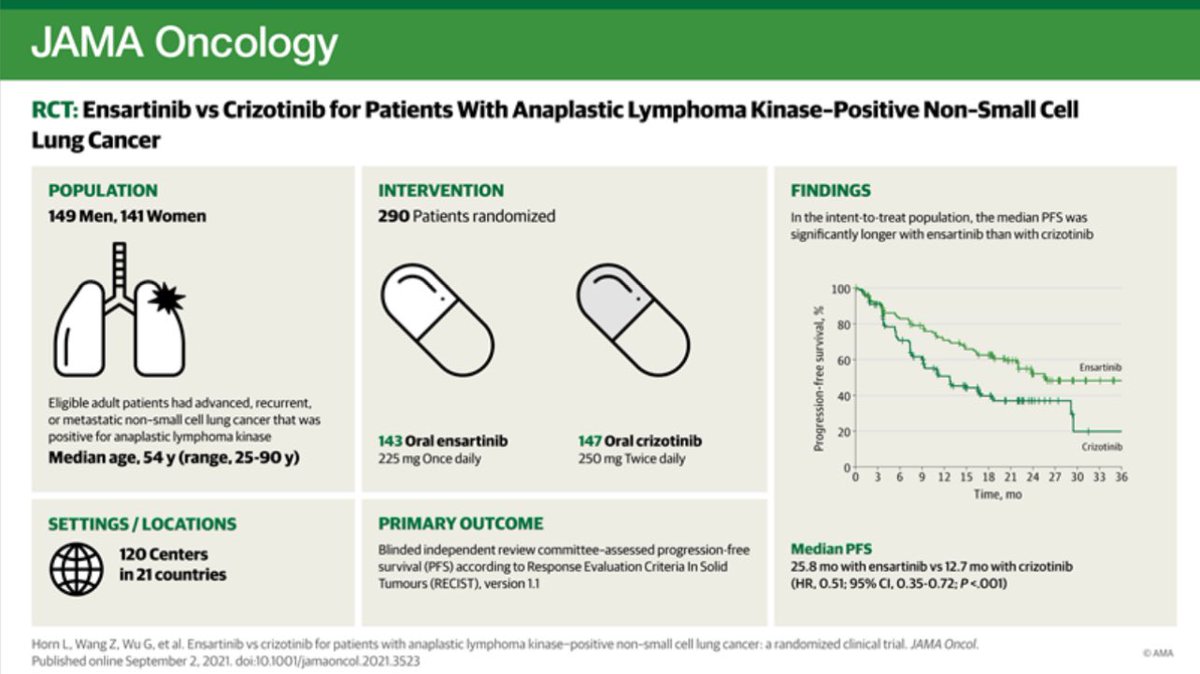
Adults with locally advanced (stage IIIB) or metastatic (stage IV) ALK-positive NSCLC who had not previously received an ALK TKI. Up to one prior chemotherapy regimen permitted. Asymptomatic brain metastases allowed (untreated if not on corticosteroids; treated if on stable/decreasing corticosteroids). ECOG PS 0-2 required. Baseline demographics: median age 54, 51% male, 56% Asian, 41% White, 95% ECOG PS 0-1, 62% never smokers, 36% with baseline CNS metastases, 26% with prior chemotherapy.
Ensartinib 225 mg orally once daily (n=143) versus crizotinib 250 mg orally twice daily (n=147), both administered in 28-day cycles until disease progression or unacceptable toxicity. Crossover was not allowed, but treatment beyond progression was permitted.
Primary endpoint: progression-free survival (PFS) by blinded independent central review (BICR) per RECIST v1.1. Key secondary endpoints: overall survival (OS), CNS response rate by BICR, time to CNS progression by BICR, and overall response rate (ORR). Other endpoints included patient-reported quality of life (EORTC QLQ-C30/LC13) and time to deterioration.
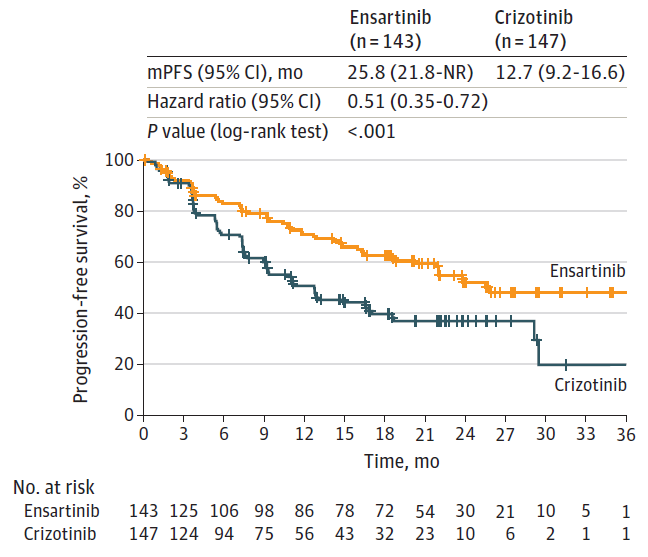
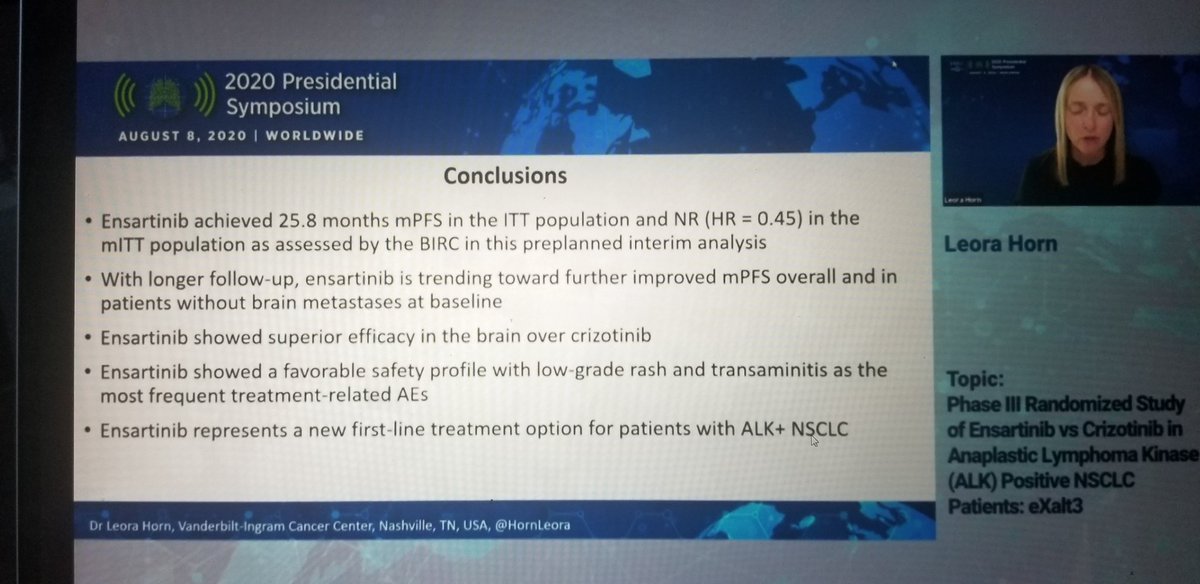
eXALT3 met its primary endpoint with a statistically significant PFS improvement. PFS HR was 0.56 (95% CI: 0.40-0.79; p=0.0007), representing a 44% reduction in the risk of progression or death. Median PFS was 25.8 months (95% CI: 21.8-NE) with ensartinib versus 12.7 months (95% CI: 9.2-16.6) with crizotinib. ORR was 74% (95% CI: 66%-81%) vs 67% (95% CI: 58%-74%), with complete response rates of 12% vs 5%. CNS ORR in patients with measurable baseline brain disease was 59% (95% CI: 33%-82%) vs 21% (95% CI: 7%-42%), including 24% vs 8% complete responses.
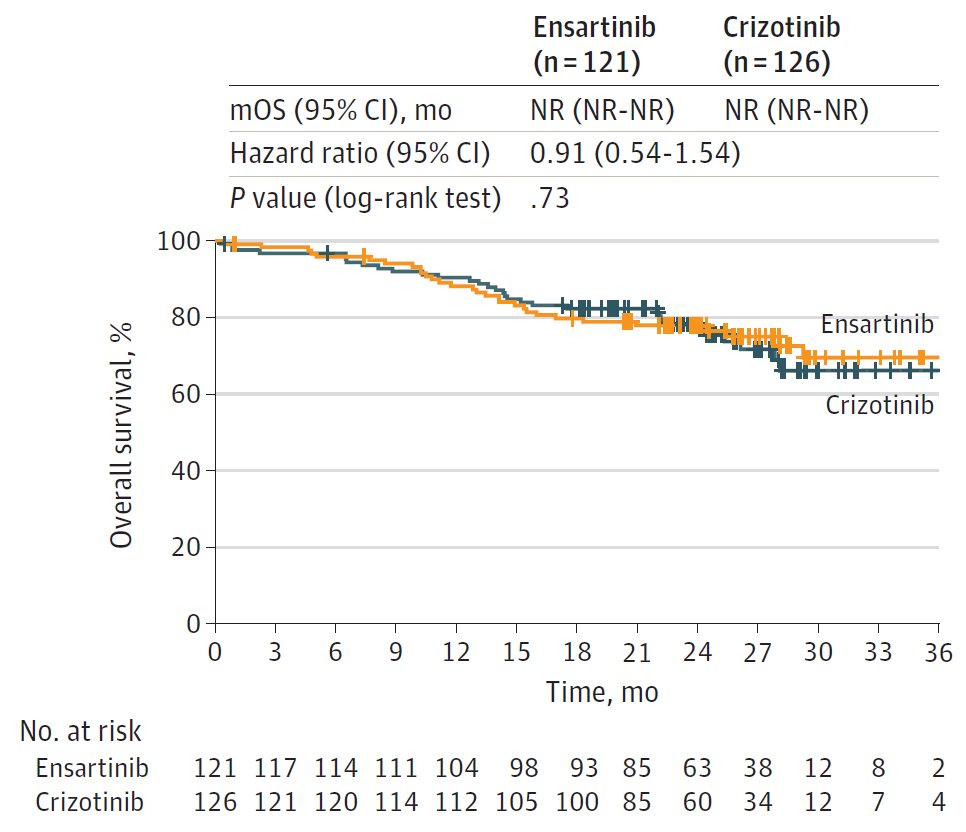
At the final OS analysis, there was no statistically significant difference between arms. Median OS was 63.2 months with ensartinib versus 55.7 months with crizotinib (HR 0.88; 95% CI: 0.63-1.23; p=0.4570). The lack of OS difference is consistent with the availability of effective subsequent ALK TKIs, allowing crossover benefit in the crizotinib arm. Both arms showed extended survival consistent with the favorable natural history of ALK-positive NSCLC.
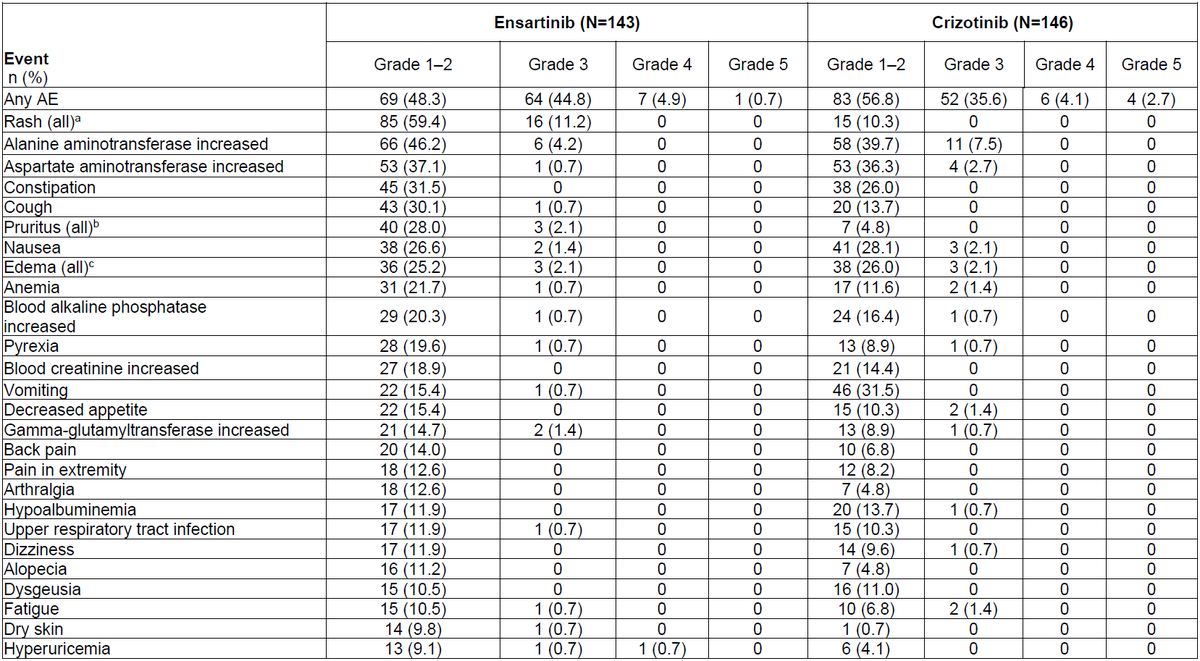
Grade 3-4 AEs occurred in approximately 50% of ensartinib patients vs 40% with crizotinib. Rash was the most common adverse reaction at 66% all-grade (12% Grade 3-4) vs 10% with crizotinib. ALT elevation occurred in 73% (5% Grade 3-4). Pruritus in 30% (2.1% G3-4). Musculoskeletal pain in 36%. Treatment discontinuation due to AEs was 12%, with key reasons being pneumonitis/ILD (2.1%), increased ALT (2.1%), and increased AST (2.1%). Dose interruptions occurred in 41% and dose reductions in 24%. One fatal adverse reaction (0.7%) due to bronchopneumonia was reported.
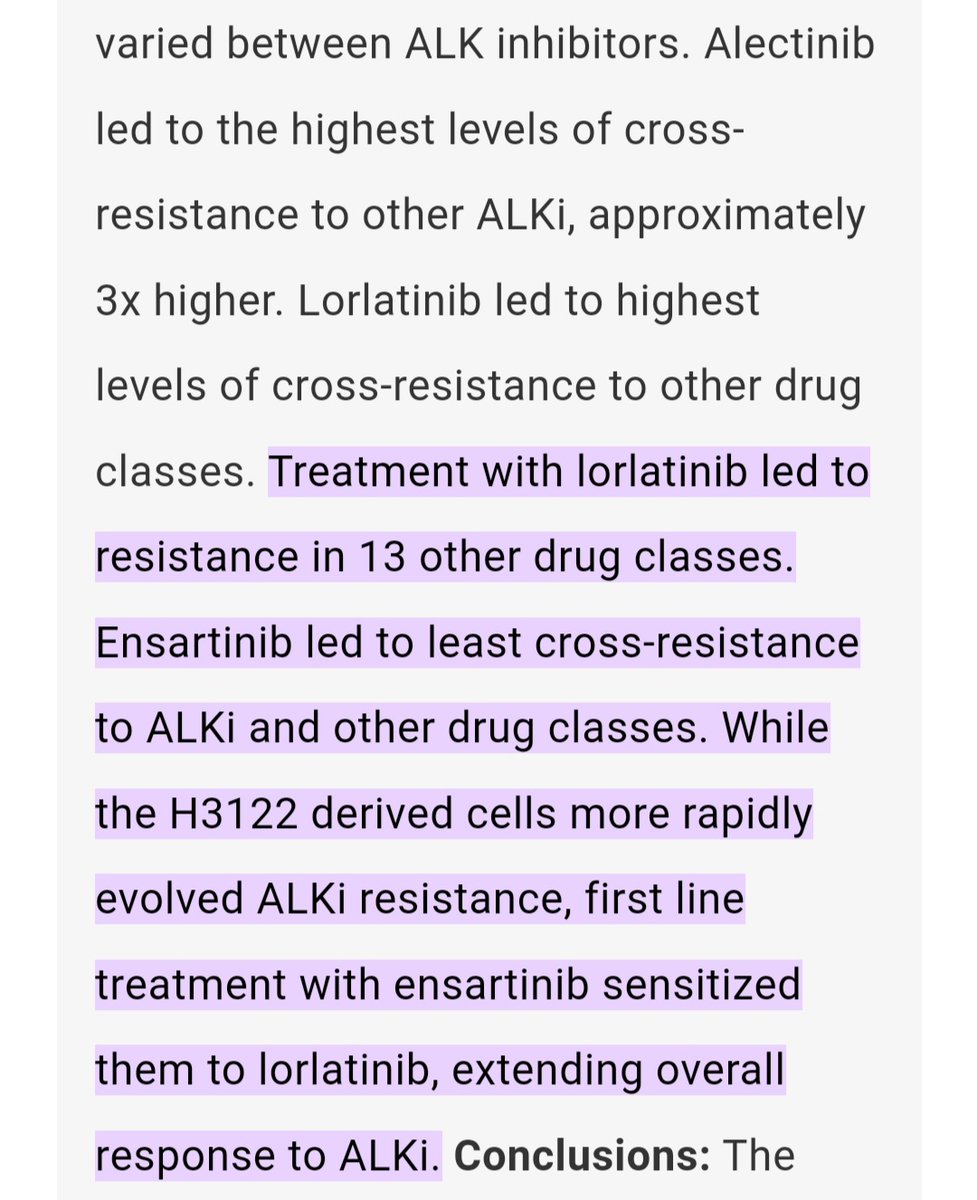
The FDA approved ensartinib (Ensacove) on November 18, 2024, for adult patients with ALK-positive locally advanced or metastatic NSCLC who have not previously received an ALK TKI. Ensartinib joins a competitive 1L ALK+ landscape alongside lorlatinib (CROWN, PFS HR 0.19), alectinib (ALEX), and brigatinib (ALTA-1L). While ensartinib's PFS HR of 0.56 vs crizotinib is clinically meaningful, the comparator was crizotinib rather than a next-gen ALK TKI, limiting direct cross-trial interpretation. Ensartinib's strong CNS activity (59% intracranial ORR) is notable. Key debates include positioning versus lorlatinib (which showed deeper PFS benefit), the significance of the rash profile (66% vs lorlatinib's CNS/metabolic AEs), and whether ensartinib offers a differentiated safety-efficacy balance for specific patient populations.