SACI-IO HR+ Key Takeaways
Design — Investigator-initiated randomized Phase 2; sacituzumab govitecan (Trodelvy) +/- pembrolizumab (Keytruda), HR+/HER2- metastatic breast cancer, PD-L1 unselected (NCT04448886). Led by Aditya Bardia. (ASCO 2024 LBA1004; ESMO Breast 2026 final)
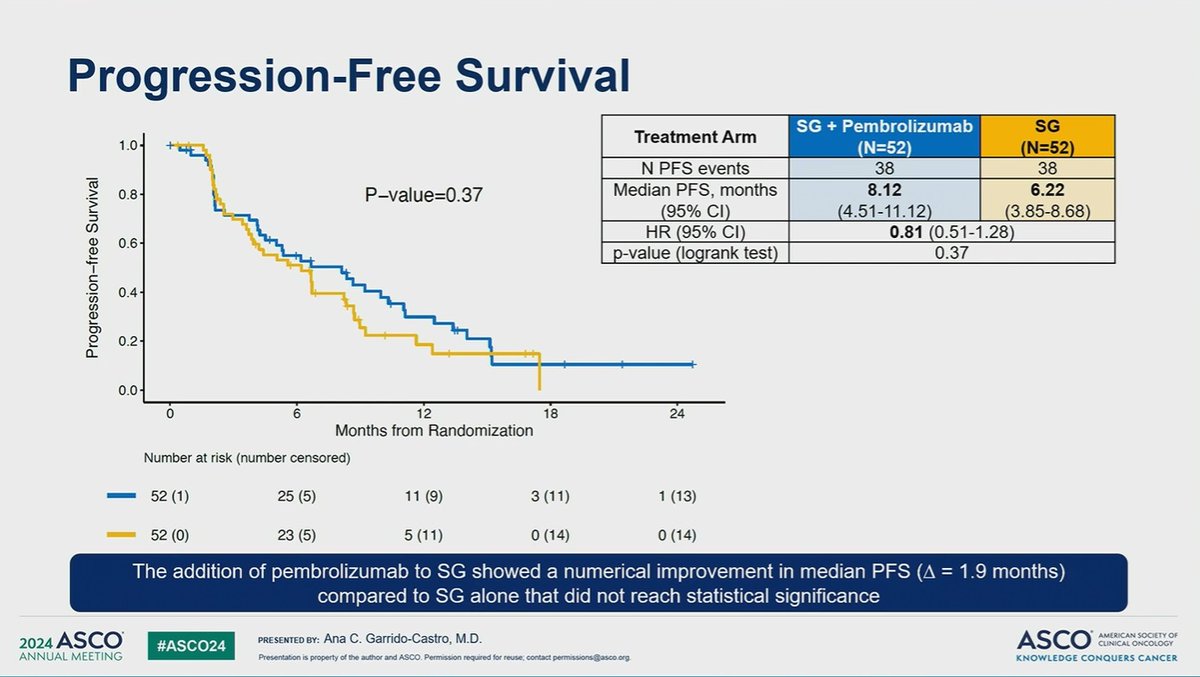
PFS (primary) — NEGATIVE — Primary endpoint NOT met. ASCO 2024: median PFS 8.1 vs 6.2 months (HR 0.81; p=0.37). Final (ESMO Breast 2026, 34.6-mo follow-up): PFS HR 0.78, p=0.12 — not significant in the intent-to-treat population. (ASCO 2024 / ESMO Breast 2026)
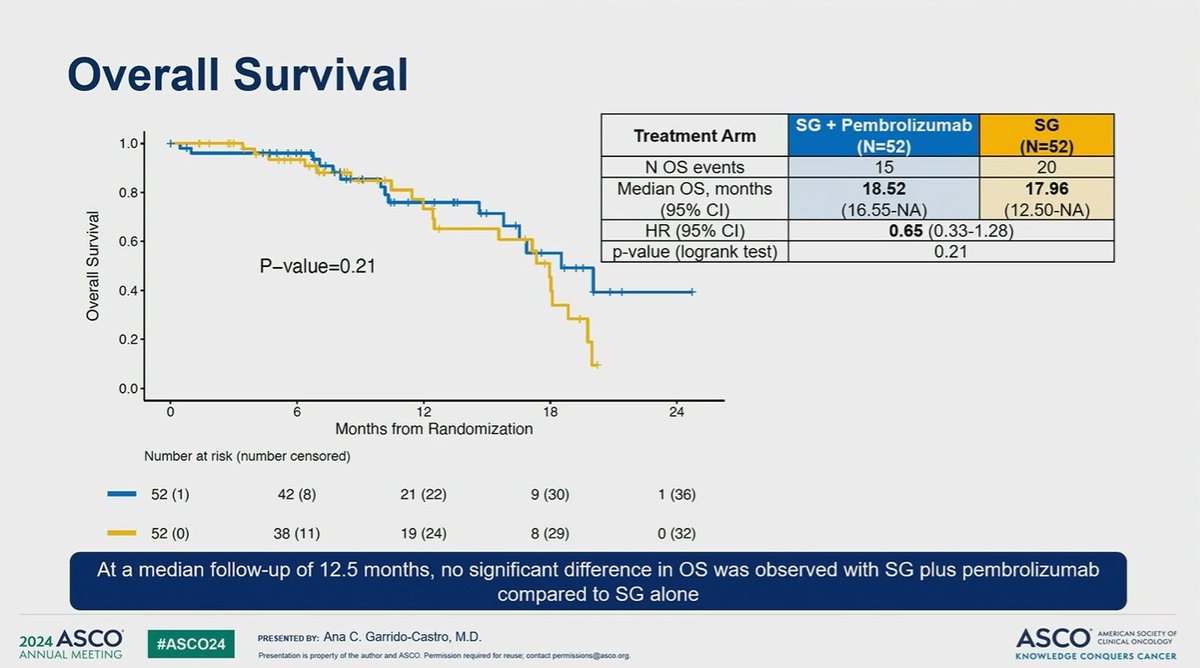
Overall survival — No significant intent-to-treat benefit: OS HR 0.97 at final analysis. (ESMO Breast 2026 / ESMO Open, July 2026)
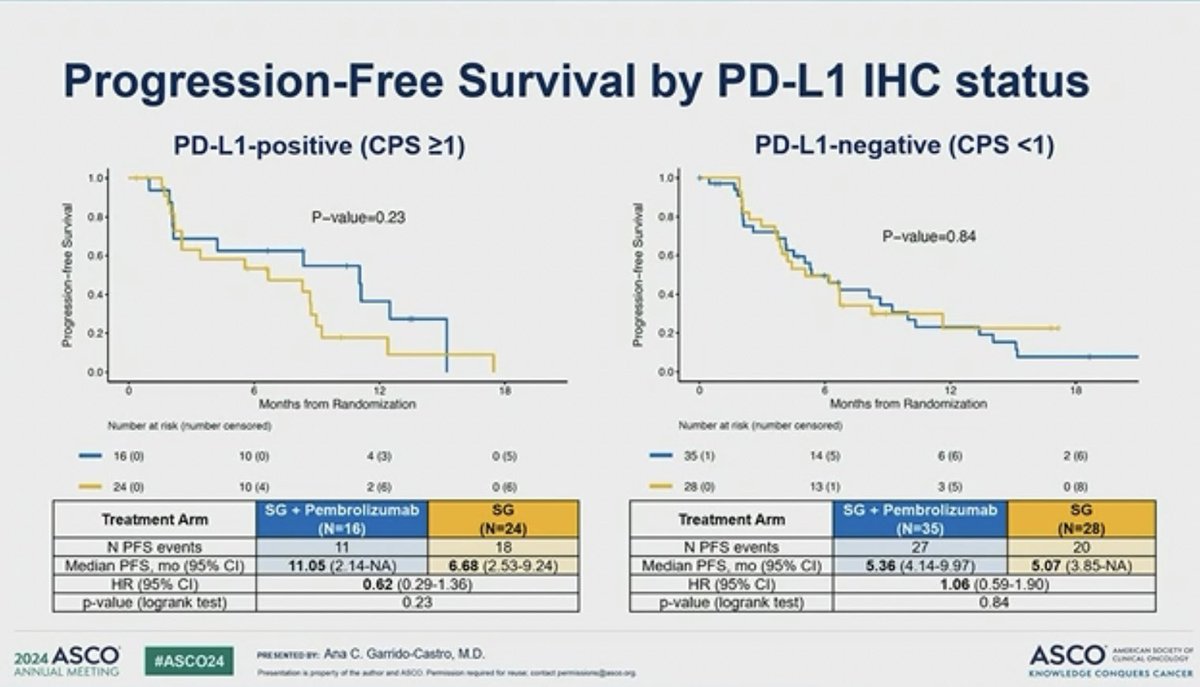
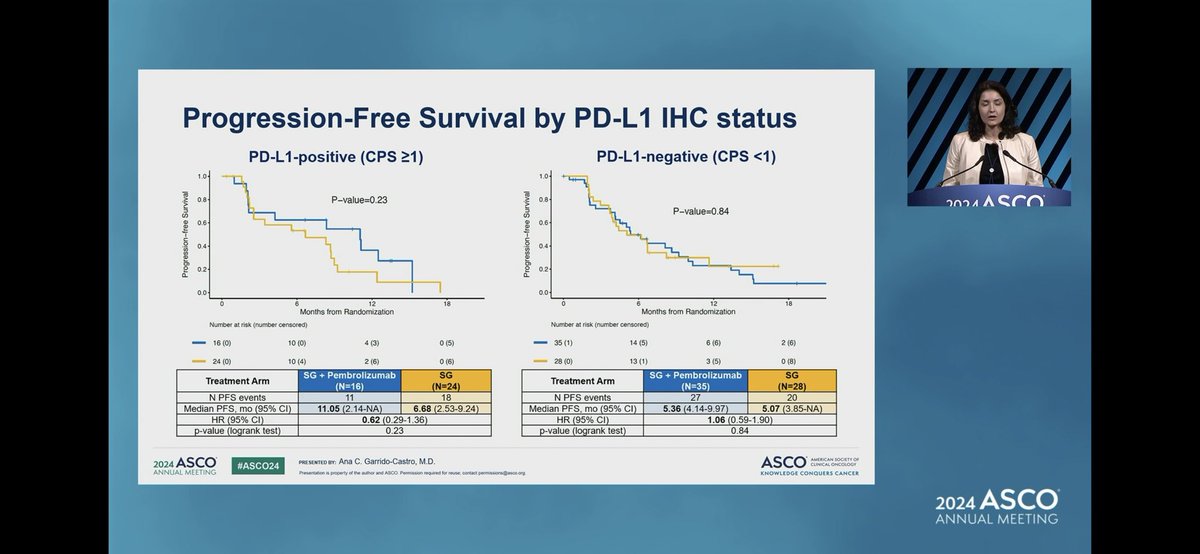
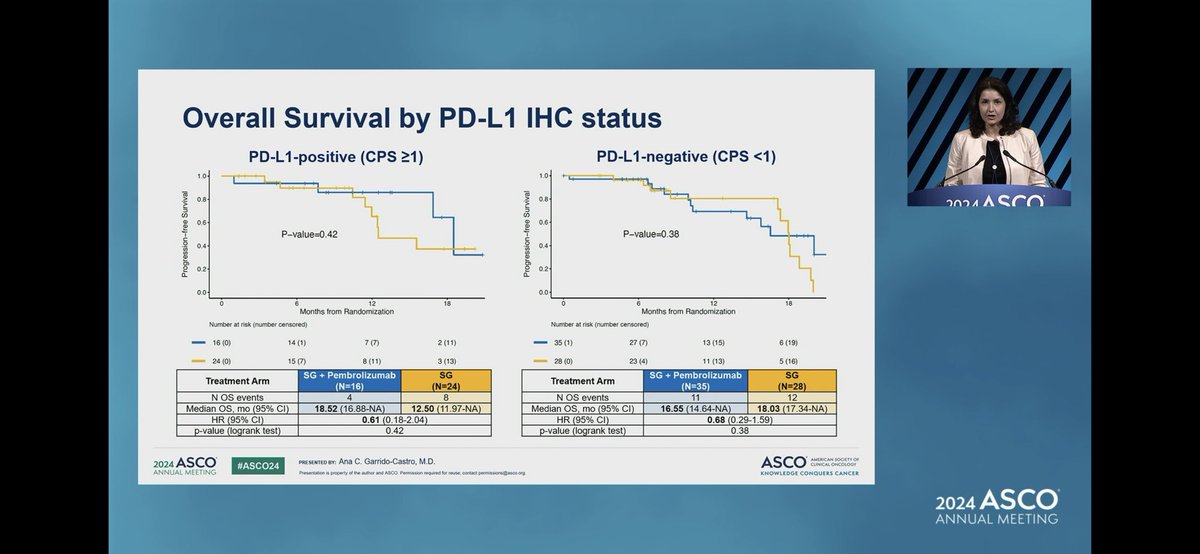
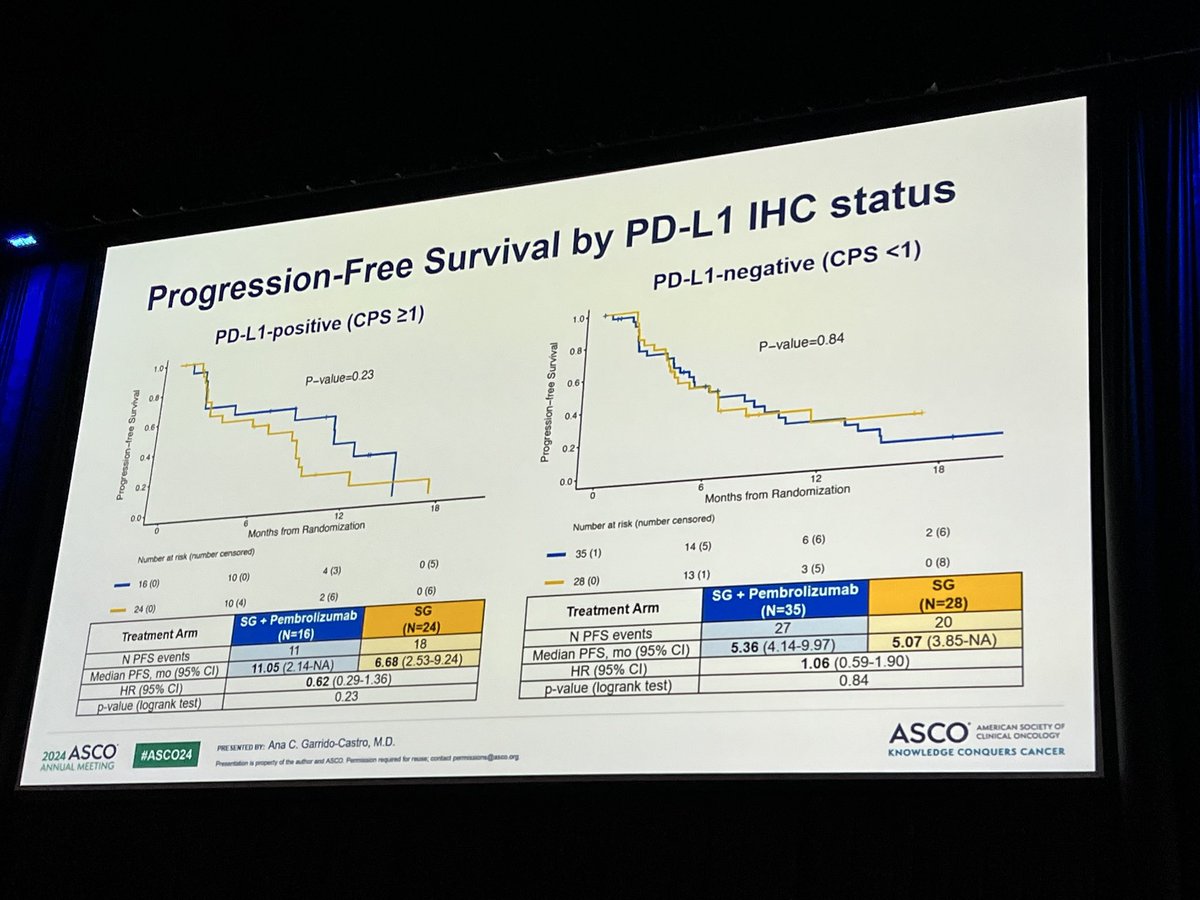
PD-L1 subgroup — A numerical signal favored the combination in the exploratory PD-L1-positive (CPS >=1) subgroup — hypothesis-generating, not confirmatory. (ESMO Breast 2026)
Safety — No new safety signals; consistent with known sacituzumab govitecan and pembrolizumab class effects (including the sacituzumab govitecan neutropenia Boxed Warning). One Grade 5 event (hepatotoxicity) reported in the monotherapy arm. (ESMO Breast 2026)
Regulatory / Sponsor — INVESTIGATIONAL + NEGATIVE — the SG + pembrolizumab combination in HR+/HER2- mBC is not FDA approved. Investigator-initiated (Aditya Bardia), with Gilead Sciences and Merck. (FDA label)
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.
Top KOLs Discussing SACI-IO HR+







SACI-IO HR+ Key Slides & Visuals
Trial slides shared by KOLs at ASCO 2024 LBA1004. Click any image to expand. OCR text extracted via AWS Textract.


[Slide 1] 16:00 - 16:12 GMT-5 ABSTRACT PRESENTATION 4 SACI-IO HR+: A randomized phase II trial of sacituzumab govitecan with or without pembrolizumab in patients with metastatic hormone receptor-positive/HER2-negative breast cancer. Abstract LBA1004 --- [Slide 2] Conclusions: Addition of pembrolizumab to SG showed a non-significant trend toward improved PFS in unselected HR+/HER2- MBC at this preliminary time point. Final PFS and updated os with further follow-up will be presented at the meeting. Exploratory outcome analyses by TROP2 and PD-L1 expression will be reported. Clinical trial information: NCT04448886. --- [Slide 3] CT for MBC. At a median follow-up of 9.2 months (mo), median PFS was 8.4 mo in Arm A vs 6.2 mo in Arm B (HR 0.76, 95% CI 0.47- 1.23, log-rank p=0.26); ORR 21.2% and 17.3%, respectively. os data are immature with only 26 events to date; os was 16.9 mo vs 17.1 mo (HR 0.65, 95% CI 0.30-1.41, log-rank p=0.28),
[Slide 1] SACI-IO HR+: Study Schema Metastatic or locally advanced Treatment continued until progression or unacceptable toxicity Endpoints unresectable breast cancer HR-positive (ER ≥ 1% or PR ≥ 1%), Sacituzumab govitecan (SG) Primary: HER2-negative (IHC 0, 1+, or 2+/ ISH-) 10 mg/kg IV D1, D8 of every 21 days PFS (ITT) + No restriction on PD-L1 status N=110 Pembrolizumab Secondary: ≥1 endocrine therapy for mBC or PFS (PD-L1+)ᵇ R 200 mg IV D1 of every 21 days progression on or within 12 months of OS (ITT, PD-L1+) 1:1 ORR, DOR, TTOR, adjuvant endocrine therapy CBR (ITT, PD-L1+) 0-1 prior chemotherapy for mBC Safety Sacituzumab govitecan (SG) No prior topoisomerase I-inhibitor ADC, 10 mg/kg IV D1, D8 of every 21 days Exploratory: irinotecan, or PD-1/-L1 inhibitor Correlative No known active brain metastases or HRQoL leptomeningeal disease Baseline Cycle 2 Optional NCT04448886 Research Research EOT Biopsy Biopsy Biopsy Study activation date 9/23/2020 Data custut for analysis 3/9/2024 amendment activated in 1/2022 to allow participants with any PO-L1 status to envioti Certral POLT testing performed with PharmOx 22C3 assay LT-positive combined positive score (CPS) at Note There is no approved COX with 22C3 for HR=HER2- MBC Aborevations HR, hormone receptor, ER estrogen receptor, PR progestarone receptor, INC immunohistochemistry ISM n situ hybridization mBC metastatic breast cancer ADC antibody drug conjugate; ITT, intent to treat PFS. progression-bee survival 05, overat survice ORR objective response rate, DOR duration of response, TTOR time to objective response CBR cirical benefit rate, HRGX health-related quality of the 2024 ASCO #ASCO24 PRS RESENTED RY: Ana C. Garrido-Castro, M.D. ASCO AMERICAN SOCIETY OH CONTAL ONCOLOGY ANNUAL MEETING Presentation . property of the author and ASOO Permission - - - contact KNOWLEDGE CONQUERS CANCER --- [Slide 2] Baseline Characteristics SG + Pembrolizumab SG Total (N=52) (N=52) (N=104) Age, median (range) 56.5 (31.0 - 81.0) 57.0 (27.0 - 80.0) 57.0 (27.0 - 81.0) Sex assigned at birth Female 50 (96.2%) 52 (100.0%) 102 (98.1%) Male 2 (3.8%) 0 (0.0%) 2 (1.9%) Race White 40 (76.9%) 44 (84.6%) 84 (80.8%) Black or African American 4 (7.7%) 3 (5.8%) 7 (6.7%) Asian 4 (7.7%) 1 (1.9%) 5 (4.8%) American Indian or Alaskan Native 1 (1.9%) 0 (0.0%) 1 (1.0%) Other 3 (5.8%) 4 (7.7%) 7 (6.7%) ER status >10% 49 (94.2%) 50 (96.2%) 99 (95.2%) 1-9% 2 (3.8%) 1 (1.9%) 3 (2.9%) Unknown 1 (1.9%) 1 (1.9%) 2 (1.9%) PD-L1 statusᵇ Negative 35 (67.3%) 28 (53.8%) 63 (60.6%) CPS >1 16 (30.8%) 24 (46.2%) 40 (38.5%) CPS 1-9 13 (25.0%) 20 (38.5%) 33 (31.7%) CPS >10 3 (5.8%) 4 (7.7%) 7 (6.7%) Not tested 1 (1.9%) 0 (0.0%) 1 (1.0%) Estrogen receptor (ER) in the most recent available tumor sample prior to study registration ER positive (% unknown) in 2 patients. Central PD-L1 testing performed on the baseline research biopsy (if a research biopsy was not performed, testing was performed on the most recent available archival turnor sample prior to study registration) Tissue was not available for testing in one patient POLI positive defined an combined positive score (CPS) at 2024 ASCO #ASCO24 PRESENTED-BY: Ana C. Garrido-Castro, M.D. ASCO AMERICAN BOCKTH OF CUNICAL ONCOLOGY ANNUAL MEETING Presentation - property of the - and ABOD - required - - KNOWLEDGE CONQUERS CANCER --- [Slide 3] Progression-Free Survival SG + Pembrolizumab SG Treatment Arm 1.0 (N=52) (N=52) N PFS events 38 38 0.8 P-value=0.37 Median PFS, months 8.12 6.22 (95% CI) (4.51-11.12) (3.85-8.68) HR (95% CI) 0.81 (0.51-1.28) 0.6 p-value (logrank test) 0.37 0.4 0.2 0.0 0 6 12 18 24 Months from Randomization Number at risk (number censored) 52 (1) 25 (5) 11 (9) 3 (11) 1 (13) 52 (0) 23 (5) 5 (11) 0 (14) 0 (14) The addition of pembrolizumab to SG showed a numerical improvement in median PFS (A = 1.9 months) compared to SG alone that did not reach statistical significance 2024 ASCO #ASCO24 PRESENTED BY Ana C. Garrido-Castro, M.D. ASCO AMERICAN SOCITY CLINICAL ANNUAL MEETING Presentation . property and ANOO KNOWLEDGE CONQUERS CANCER --- [Slide 4] Progression-Free Survival by PD-L1 IHC status PD-L1-positive (CPS >1) PD-L1-negative (CPS <1) 1.0 1.0 0.8 P-value=0.23 0.8 P-value=0.84 0.6 0.6 0.4 0.4 0.2 02 0.0 0.0 0 6 12 18 0 6 12 18 Months from Randomization Months from Randomization Number at risk (number censored) Number at risk (number censored) 16 (0) 10 (0) 4 (3) (5) 35 (1) 14 (5) (6) 2 (6) 24 (0) 10(4) 2(6) ©(6) 28 (0) 13(1) 3 (5) 0 (8) SG Pembrollzumab SG SG + Pembrolizumab SG Treatment Arm Treatment Arm (N=16) (N=24) (N=35) (N=28) N PFS events 11 18 N PFS events 27 20 Median PFS, mo (95% CI) 11.05 (2.14-NA) 6.68 (2.53-9.24) Median PFS, mo (95% CI) 5.36 (4.14-9.97) 5.07 (3.85-NA) HR (95% CI) 0.62 (0.29-1.36) HR (95% CI) 1.06 (0.59-1.90) p-value (logrank test) 0.23 p-value (logrank test) 0.84 2024 ASCO PRESENTED-FY Ana C. Garrido-Castro M.D. #ASCO24 ASCO ANNUAL MEETING KNOWLEDGE CANCER
[Slide 1] SACI-IO HR+: Study Schema Metastatic or locally advanced Treatment continued until progression or unacceptable toxicity Endpoints unresectable breast cancer HR-positive (ER > 1% or PR > 1%), Sacituzumab govitecan (SG) Primary: 2024ASCO HER2-negative (IHC 0, 1+, or 2+/ ISH-) 10 mg/kg IV D1, D8 of every 21 days PFS (ITT) + No restriction on PD-L1 status N=110 Pembrolizumab Secondary: >1 endocrine therapy for mBC or PFS (PD-L1+)b R 200 mg IV D1 of every 21 days OS (ITT, PD-L1+) progression on or within 12 months of 1:1 ORR, DOR, TTOR, adjuvant endocrine therapy CBR (ITT, PD-L1+) 0-1 prior chemotherapy for mBC Safety Sacituzumab govitecan (SG) No prior topoisomerase I-inhibitor ADC, 10 mg/kg IV D1, D8 of every 21 days Exploratory: irinotecan, or PD-1/-L1 inhibitor Correlative No known active brain metastases or HRQoL leptomeningeal disease Baseline Cycle 2 Optional NCT04448886 Research Research EOT Biopsy Biopsy Biopsy Study activation date 9/23/2020 Data cutoff for analysis 3/9/2024 Protocol amendment activated in 2022 alow participants with any PD-L1 status to error Central POLI testing performed with Pharm(s) 2203 assay POL 1-positive combined positive score (CPS) 11. Note There no approved COx with 2203 for *R*HER2 mbC Activiviations HR, hormone receptor, ER, estroges receptor, PR progesterone receptor INC. ISM nec metastatic treast cancer, ADC antibody drug compate ITT, intent-in treat, PFS, progression-tree survival, os, overall survival, ORR, stigetive response rate COR, duration if response, TTOR time to objective response CBR cirical benefit rate HROX health-nelated related quality 2024 ASCO #ASCO24 PRESENTED (PY) Ana C. Garrido-Castro, M.D. ASCO AMERICAN SOCIETY CUNICAL ONCOLOGY ANNUAL MEETING Presentation property author and ABCO Permission request to - KNOWLEDGE CONQUERS CANCER 2024 ASCO ANNUAL MEETING --- [Slide 2] Baseline Characteristics SG + Pembrolizumab SG Total (N=52) (N=52) (N=104) Age, median (range) 56.5 (31.0 81.0) 57.0 (27.0 80.0) 57.0 (27.0 81.0) Sex assigned at birth Female 50 (96.2%) 52 (100.0%) 102 (98.1%) 2024ASCO Male 2 (3.8%) 0 (0.0%) 2 (1.9%) Race White 40 (76.9%) 44 (84.6%) 84 (80.8%) Black or African American 4 (7.7%) 3 (5.8%) 7 (6.7%) Asian 4 (7.7%) 1 (1.9%) 5 (4.8%) American Indian or Alaskan Native 1 (1.9%) 0 (0.0%) 1 (1.0%) Other 3 (5.8%) 4 (7.7%) 7 (6.7%) ER status >10% 49 (94.2%) 50 (96.2%) 99 (95.2%) 1-9% 2 (3.8%) 1 (1.9%) 3 (2.9%) Unknown 1 (1.9%) 1 (1.9%) 2 (1.9%) PD-L1 statusb Negative 35 (67.3%) 28 (53.8%) 63 (60.6%) CPS >1 16 (30.8%) 24 (46.2%) 40 (38.5%) CPS 1-9 13 (25.0%) 20 (38.5%) 33 (31.7%) CPS >10 3(5.8%) 4 (7.7%) 7 (6.7%) Not tested 1 (1.9%) 0 (0.0%) 1 (1.0%) Estrogen receptor (ER) in the most recent available turnor sample prior to shudy registration ER positive % unknown) patients *Central POLI testing performed on the baseline research biopsy of research biopsy was not performed, testing was performed on the most recent available archival tumor sample prior to study registration) Tissue was not available for testing in one patient PDL positive defined as combined positive score (CPS) at 2024 ASCO #ASCO24 PRESENTED BY: Ana C. Garrido-Castro, M.D. ASCO AMERICAN ANNUAL MEETING I property and ASCO - KNOWLEDGE CONQUERS CANCER 2024 ASCO ANNUAL MEETING --- [Slide 3] Progression-Free Survival by PD-L1 IHC status PD-L1-positive (CPS ≥1) PD-L1-negative (CPS <1) 1.0 1.0 0.8 P-value=0.23 0.8 2024 AS Progression-free Survival 0.6 0.4 Progression-free Survival P-value=0. 0.6 0.4 0.2 0.2 0.0 0.0 0 6 12 18 0 6 12 18 Months from Randomization Months from Randomization Number at risk (number censored) Number at risk (number censored) 16(0) 10(0) 4(3) 0(5) 35(1) 14(5) 6 (6) 2 (6) 24(0) 10(4) 2(6) 0 (6) 28(0) 13(1) 3(5) 0 (8) SG + Pembrolizumab SG SG + Pembrolizumab SG Treatment Arm Treatment Arm (N=16) (N=24) (N=35) (N=28) N PFS events 11 18 N PFS events 27 20 Median PFS, mo (95% CI) 11.05 (2.14-NA) 6.68 (2.53-9.24) Median PFS, mo (95% CI) 5.36 (4.14-9.97) 5.07 (3.85-NA) HR (95% CI) 0.62 (0.29-1.36) HR (95% CI) 1.06 (0.59-1.90) p-value (logrank test) 0.23 p-value (logrank test) 0.84 2024 ASCO #ASCO24 PRESENTED BY Ana C. Garrido-Castro, M.D. ASCO AMERICAN SOCIETY DE CLINICAL ONCOLOGY ANNUAL MEETING Presentation I and ABOD Permission - contact.permason@asce.org KNOWLEDGE CONQUERS CANCER AS --- [Slide 4] Overall Survival by PD-L1 IHC status PD-L1-positive (CPS ≥1) PD-L1-negative (CPS <1) 1.0- 1.0- 0.8 0.8 202 A Progression-free Survival 0.6 P-value=0.42 0.4 Progression-free Survival 0.6 P-value=0.38 0.4 0.2 0.2 0.0 0.0 0 6 12 18 0 6 12 18 Months from Randomization Months from Randomization Number at risk (number censored) Number at risk (number censored) 16(0) 14(1) 7 (7) 2(11) 35(1) 27 (7) E 13(15) 6(19) 24(0) 15(7) 8(11) 3(13) 28(0) 23(4) 11(13) 5(16) SG + Pembrolizumab SG SG + Pembrolizumab SG Treatment Arm Treatment Arm (N=16) (N=24) (N=35) (N=28) N OS events 4 8 N OS events 11 12 Median OS, mo (95% CI) 18.52 (16.88-NA) 12.50 (11.97-NA) Median OS, mo (95% CI) 16.55 (14.64-NA) 18.03 (17.34-NA) HR (95% CI) 0.61 (0 18-2.04) HR (95% CI) 0.68 (0 29-1.59) p-value (logrank test) 0.42 p-value (logrank test) 0.38 2024 ASCO #ASCO24 PRESENTED BY: Ana C. Garrido-Castro, M.D. ASCO AMERICAN SOCIETY OF CURICAL OHCOLOGY ANNUAL MEETING Presentation property author and ABOO Permission required for - contact permissors@asco.org KNOWLEDGE CONQUERS CANCER A
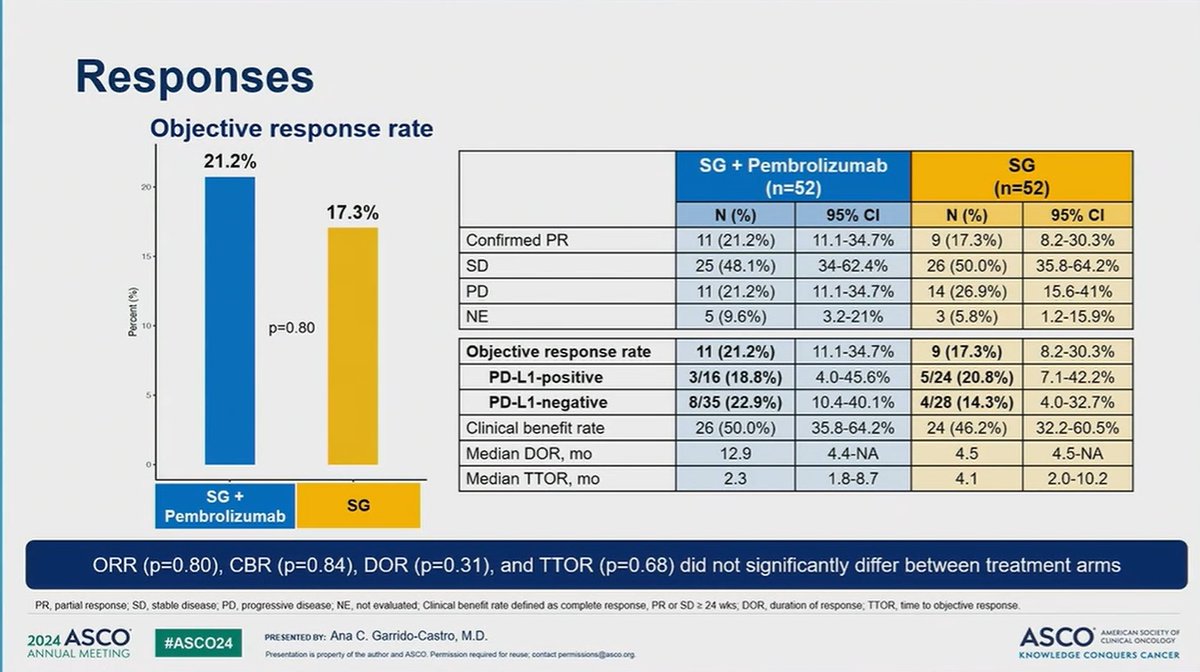
[Slide 1] SACI-IO HR+: Study Schema Metastatic or locally advanced Treatment continued until progression or unacceptable toxicity Endpoints unresectable breast cancer HR-positive (ER ≥ 1% or PR ≥ 1%), Sacituzumab govitecan (SG) Primary: HER2-negative (IHC 0, 1+, or 2+/ ISH-) 10 mg/kg IV D1, D8 of every 21 days PFS (ITT) + No restriction on PD-L1 status N=110 Secondary: Pembrolizumab ≥1 endocrine therapy for mBC or PFS (PD-L1+)b R 200 mg IV D1 of every 21 days OS (ITT, PD-L1+) progression on or within 12 months of 1:1 ORR, DOR, TTOR, adjuvant endocrine therapy CBR (ITT, PD-L1+) 0-1 prior chemotherapy for mBC Safety Sacituzumab govitecan (SG) No prior topoisomerase I-inhibitor ADC, 10 mg/kg IV D1, D8 of every 21 days Exploratory: irinotecan, or PD-1/-L1 inhibitor Correlative No known active brain metastases or HRQoL leptomeningeal disease Baseline Cycle 2 Optional NCT04448886 Research Research EOT Biopsy Biopsy Biopsy Study activation date: 9/23/2020 Data cutoff for analysis: 3/9/2024 . Protocol amendment activated in 1/2022 to allow participants with any PD-L1 status to enroll 0 Central PD-L1 testing performed with PharmDx 22C3 assay. PD-L1-positive combined positive score (CPS) 21. Note: There is no approved CDx with 22C3 for HR+/HER2- mBC. Abbreviations: HR, hormone receptor; ER, estrogen receptor; PR, progesterone receptor; IHC, immunohistochemistry; ISH, in situ hybridization; mBC, metastatic breast cancer; ADC, antibody drug conjugate; ITT, intent-to-treat; PFS, progression-free survival; OS, overall survival; ORR, objective response rate; DOR, duration of response; TTOR. time to objective response; CBR, clinical benefit rate; HRQoL, health-related quality of life. 2024 ASCO #ASCO24 PRESENTED BY: Ana C. Garrido-Castro, M.D. ASCO AMERICAN SOCIETY OF CLINICAL ONCOLOGY ANNUAL MEETING Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.org KNOWLEDGE CONQUERS CANCER --- [Slide 2] Progression-Free Survival SG + Pembrolizumab SG Treatment Arm 1.0 (N=52) (N=52) N PFS events 38 38 0.8 P-value=0.37 Median PFS, months 8.12 6.22 Progression-free Survival (95% CI) (4.51-11.12) (3.85-8.68) HR (95% CI) 0.81 (0.51-1.28) 0.6 p-value (logrank test) 0.37 0.4 0.2 0.0 0 6 12 18 24 Months from Randomization Number at risk (number censored) 52 (1) 25 (5) 11 (9) 3 (11) 1 (13) 52 (0) 23 (5) 5 (11) 0 (14) 0 (14) The addition of pembrolizumab to SG showed a numerical improvement in median PFS (4 = 1.9 months) compared to SG alone that did not reach statistical significance 2024 ASCO PRESENTED BY: Ana C. Garrido-Castro, M.D. ASCO AMERICAN SOCIETY OF #ASCO24 CLINICAL ONCOLOGY ANNUAL MEETING Presentation is property of the author and ASCO Permission required for reuse, contact permissions@asco.co org. KNOWLEDGE CONQUERS CANCER --- [Slide 3] Overall Survival SG + Pembrolizumab SG Treatment Arm 1.0 (N=52) (N=52) N OS events 15 20 0.8 Median OS, months 18.52 17.96 (95% CI) (16.55-NA) (12.50-NA) Overall Survival HR (95% CI) 0.65 (0.33-1.28) 0.6 p-value (logrank test) 0.21 P-value=0.21 0.4 0.2 0.0 0 6 12 18 24 Months from Randomization Number at risk (number censored) 52 (1) 42 (8) 21 (22) 9 (30) 1 (36) 52 (0) 38 (11) 19 (24) 8 (29) 0 (32) At a median follow-up of 12.5 months, no significant difference in OS was observed with SG plus pembrolizumab compared to SG alone 2024 ASCO #ASCO24 PRESENTED BY: Ana C. Garrido-Castro, M.D. ASCO AMERICAN SOCIETY OF CLINICAL ONCOLOGY ANNUAL MEETING Presentation IS property of the author and ASCO Permission required for reuse, contact permissions@asco.o KNOWLEDGE CONQUERS CANCER --- [Slide 4] Responses Objective response rate 21.2% SG + Pembrolizumab SG 20 (n=52) (n=52) 17.3% N (%) 95% CI N (%) 95% CI Confirmed PR 11 (21.2%) 11.1-34.7% 9 (17.3%) 8.2-30.3% 15 SD 25 (48.1%) 34-62.4% 26 (50.0%) 35.8-64.2% PD 11 (21.2%) 11.1-34.7% 14 (26.9%) 15.6-41% Percent (%) NE 5 (9.6%) 3.2-21% 3 (5.8%) 1.2-15.9% 10 p=0.80 Objective response rate 11 (21.2%) 11.1-34.7% 9 (17.3%) 8.2-30.3% PD-L1-positive 3/16 (18.8%) 4.0-45.6% 5/24 (20.8%) 7.1-42.2% 5 PD-L1-negative 8/35 (22.9%) 10.4-40.1% 4/28 (14.3%) 4.0-32.7% Clinical benefit rate 26 (50.0%) 35.8-64.2% 24 (46.2%) 32.2-60.5% Median DOR, mo 12.9 4.4-NA 4.5 4.5-NA 0 Median TTOR, mo 2.3 1.8-8.7 4.1 2.0-10.2 SG + SG Pembrolizumab ORR (p=0.80), CBR (p=0.84), DOR (p=0.31), and TTOR (p=0.68) did not significantly differ between treatment arms PR, partial response; SD, stable disease; PD, progressive disease; NE, not evaluated; Clinical benefit rate defined as complete response, PR or SD 2 24 wks; DOR, duration of response; TTOR, time to objective response. 2024 ASCO #ASCO24 PRESENTED BY: Ana C. Garrido-Castro, M.D. ASCO AMERICAN SOCIETY OF CLINICAL ONCOLOGY ANNUAL MEETING Presentation is property of the author and ASCO Permission required for reuse; contact permissions@asco.org KNOWLEDGE CONQUERS CANCER


[Slide 1] 2024ASCO ANNUAL MEETING ASCO® AMERICAN SOCIETY OF CLINICAL ONCOLOGY --- [Slide 2] SACI-IO HR+: Study Schema Metastatic or locally advanced Treatment continued until progression or unacceptable toxicity Endpoints unresectable breast cancer HR-positive (ER ≥ 1% or PR ≥ 1%), Sacituzumab govitecan (SG) Primary: HER2-negative (IHC 0, 1+, or 2+/ ISH-) 10 mg/kg IV D1, D8 of every 21 days PFS (ITT) + No restriction on PD-L1 status N=110 Secondary: Pembrolizumab PFS (PD-L1+)b ≥1 endocrine therapy for mBC or R 200 mg IV D1 of every 21 days OS (ITT, PD-L1+) progression on or within 12 months of 1:1 ORR, DOR, TTOR, adjuvant endocrine therapy CBR (ITT, PD-L1+) 0-1 prior chemotherapy for mBC Safety Sacituzumab govitecan (SG) No prior topoisomerase I-inhibitor ADC, 10 mg/kg IV D1, D8 of every 21 days Exploratory: irinotecan, or PD-1/-L1 inhibitor Correlative No known active brain metastases or HRQoL leptomeningeal disease Baseline Cycle 2 Optional NCT04448886 Research Research EOT Biopsy Biopsy Biopsy Study activation date: 9/23/2020 Data cutoff for analysis 3/9/2024 Protocol amendment activated in 1/2022 to allow participants with any PD-L1 status to enroll Central PD-L1 testing performed with PharmDx 22C3 assay PD-L1 -positive, combined positive score (CPS) 21 Note: There is no approved CDx with 22C3 for HR+/HER2-mBC Abbreviations HR, hormone receptor; ER estrogen receptor, PR, progesterone receptor IHC, immunohistochemistry, ISH, in situ hybridization mBC, life metastatic breast cancer; ADC. antibody drug conjugate; ITT. intent-to-treat PFS, progression- free survival; OS, overall survival ORR, objective response rate, DOR, duration of response, TTOR time to objective response, CBR, clinical benefit rate: HRQoL. health-related quality of 2024 ASCO ASCO AMERICAN SOCIETY OF PRE SENTED BY: Ana C. Garrido-Castro, M.D. CLINICAL ONCOLOGY #ASCO24 Presentation is property of the author and ASCO. Permission required for reuse, contact permissions@asco.org KNOWLEDGE CONQUERS CANCER ANNUAL MEETING --- [Slide 3] Progression-Free Survival SG + Pembrolizumab SG 1.0 Treatment Arm (N=52) (N=52) N PFS events 38 38 0.8 P-value=0.37 Median PFS, months 8.12 6.22 Progression-free Survival (95% CI) (4.51-11.12) (3.85-8.68) 0.6 HR (95% CI) 0.81 (0.51-1.28) p-value (logrank test) 0.37 0.4 0.2 0.0 0 6 12 18 24 Months from Randomization Number at risk (number censored) 52 (1) 25 (5) 11 (9) 3 (11) 1 (13) 52 (0) 23 (5) 5 (11) 0 (14) 0 (14) The addition of pembrolizumab to SG showed a numerical improvement in median PFS (A = 1.9 months) compared to SG alone that did not reach statistical significance 2024 ASCO #ASCO24 PRESENTED DT: Ana C. Garrido-Castro, M.D. ASCO AMERICAN SOCIETY OF CLINICAL ONCOLOGY ANNUAL MEETING Preventation a property of the author and ASCO Permission required for - contact KNOWLEDGE CONQUERS CANCER --- [Slide 4] Progression-Free Survival by PD-L1 IHC status PD-L1-positive (CPS ≥1) PD-L1-negative (CPS <1) 1.0 1.0 0.8 P-value=0.23 0.8 Progression-free Survival Progression-free Survival P-value=0.84 0.6 0.6 0.4 0.4 0.2 0.2 0.0 0.0 0 6 12 18 0 6 12 Months from Randomization 18 Months from Randomization Number at risk (number censored) Number at risk (number censored) 16 (0) 10 (0) 4 (3) (5) 35 (1) 14(5) 6 (6) 2 (6) 24 (0) 10 (4) 2 (6) 0 (6) 28 (0) 13(1) 3(5) 0 (8) SG + Pembrolizumab SG Treatment Arm Treatment Arm SG + Pembrolizumab SG (N=16) (N=24) (N=35) (N=28) N PFS events 11 18 N PFS events 27 20 Median PFS, mo (95% CI) 11.05 (2.14-NA) 6.68 (2.53-9.24) Median PFS, mo (95% CI) 5.36 (4.14-9.97) 5.07 (3.85-NA) HR (95% CI) 0.62 (0.29-1.36) HR (95% CI) 1.06 (0.59-1.90) p-value (logrank test) 0.23 p-value (logrank test) 0.84 2024 ASCO #ASCO24 PRE SENTED BY: Ana C. Garrido-Castro, M.D. ASCO AMERICAN SOCIETY OF CLINICAL ONCOLOGY ANNUAL MEETING Presentation a property of the author and ASCO Permission required for reuse, contact permissions@asco.org KNOWLEDGE CONQUERS CANCER

[Slide 1] 2024 ASCO ANNUAL MEETING Enfortumab Vedotin in the HR+/HER2- and Triple-Negative Breast Cancer Cohorts of EV-202 Antonio Giordano, MD. PhD:' Art All Awan, MD:3 Justine Yang Bruce, MD:3 Hope S. Rugo, MD:⁴ Jenn R Diamond, MD:³ Yelena Novik, MD: Joaquina Saranda MD:7 Kei Muro, MD. PhD;° Makiko Ono, M Rita Nanda, MD: Jason Kaplan, MD:" Seema Gora, MD:" Shubin Liu, MSc;" Michele Wozniak, P! Anthony Lee, PharmD: 12 Tiffany Traina. MD 2 I I I I I I I I I 1 I I I I 1 I . I - USA United d - to CA - - Center Autora, on USA Langure - New NY USA United of - Maintal Caster Retern a Takya The OF - - Charago L - - - - USA - Cassuer - - USA 2024 ASCO - - NO - ASCO --- [Slide 2] 2024 ASCO Dana-Farber ANNUAL MEETING Cancer Institute SACI-IO HR+: A randomized phase II trial of sacituzumab govitecan with or without pembrolizumab in patients with metastatic hormone receptor-positive HER2-negative breast cancer Ana C. Garrido-Castro', Se Eun Kim2, Jennifer Desrosiers Rts Nanda³, Yara Abdou Amy S. Clark Ruth Sacks Thoma O'Connor', Natalie Sinclair', Steve Lo Amy Thomas Elean Mirabel Tess O'Meara', Nancy U. Lin', Harold J. Burstein¹, Mengni He', David Rmm Elizabeth A Mitandorf Nabhah Sara M. Tolaney - Oreging Program, Date Fatestington and Numer's Cancer Cardon - - Dear of Department of Cata Scenom Dana Farter Cancer institute too Department if Medicine Section of The University of Cheese, - L Underge Compensive Cancer Certer Obsision of Unity north Carolina Chapel Ha, NC Osign of Hemetacy Onessinge University If - - FA Department d Hematology and Medical Onesiogy Wrship Cancer the Enery University Adama GA Stambers Hospital, Stanted C7, Department of Putsing - I - If Medicine, New - CT. 2014 ASCO #ASCO24 Ana c MD. WEETING ASCO ENDOLLEDGE CONQUERS CAMILES --- [Slide 3] - for . A Tuo GU P - - Now A - - .111 Decology 0ncology You nuwwy or a à incology à SU Encology 000 PO 000 U


[Slide 1 — Study Schema]
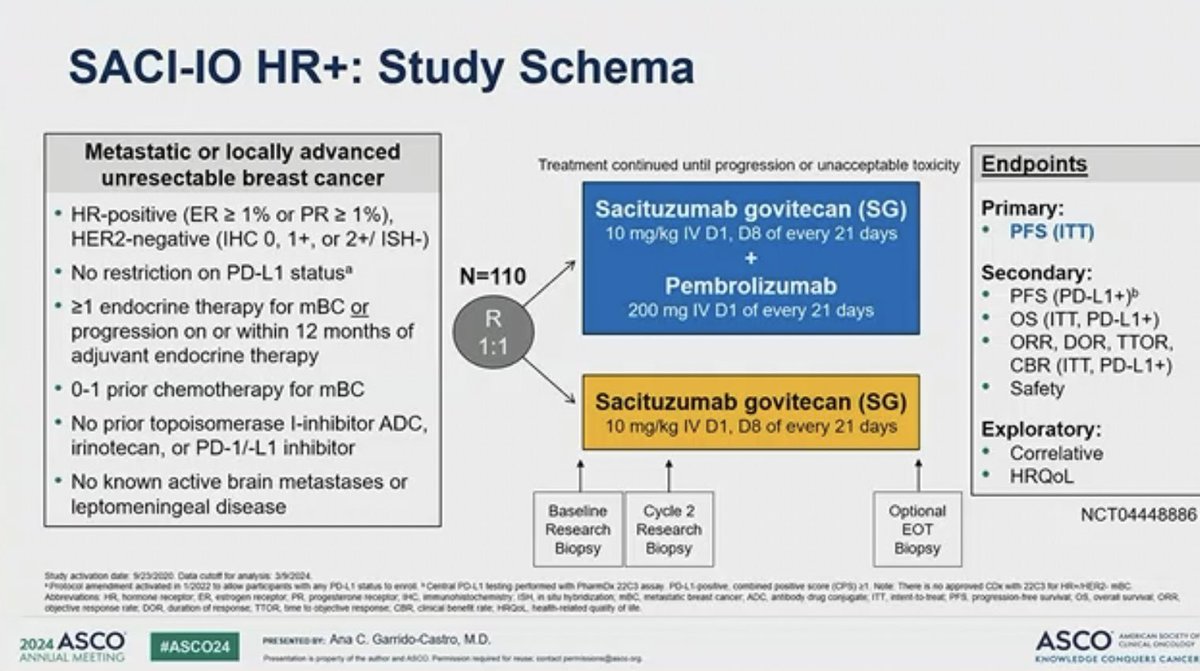
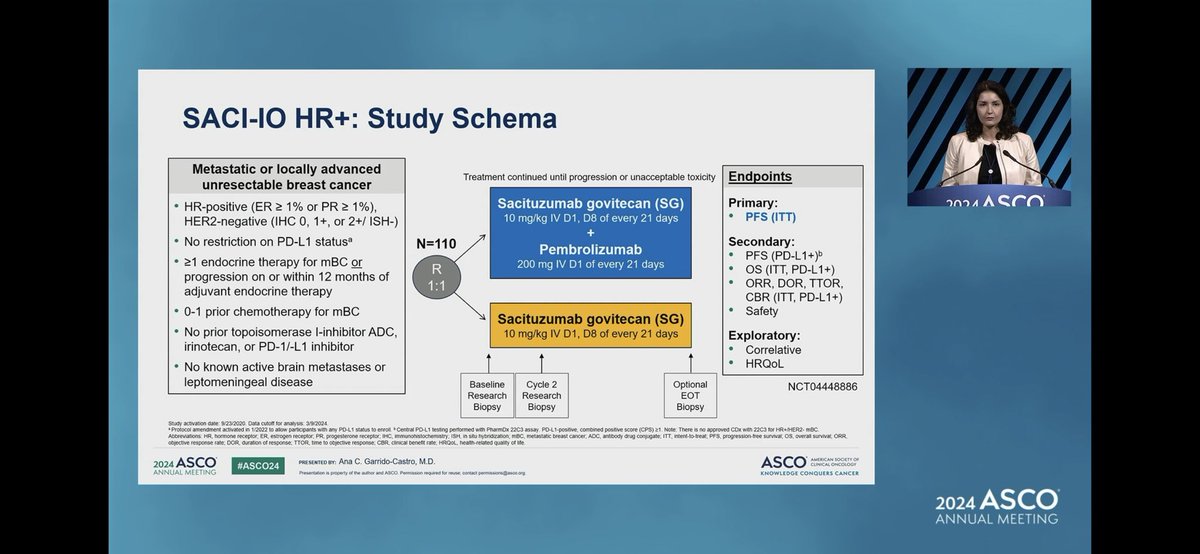
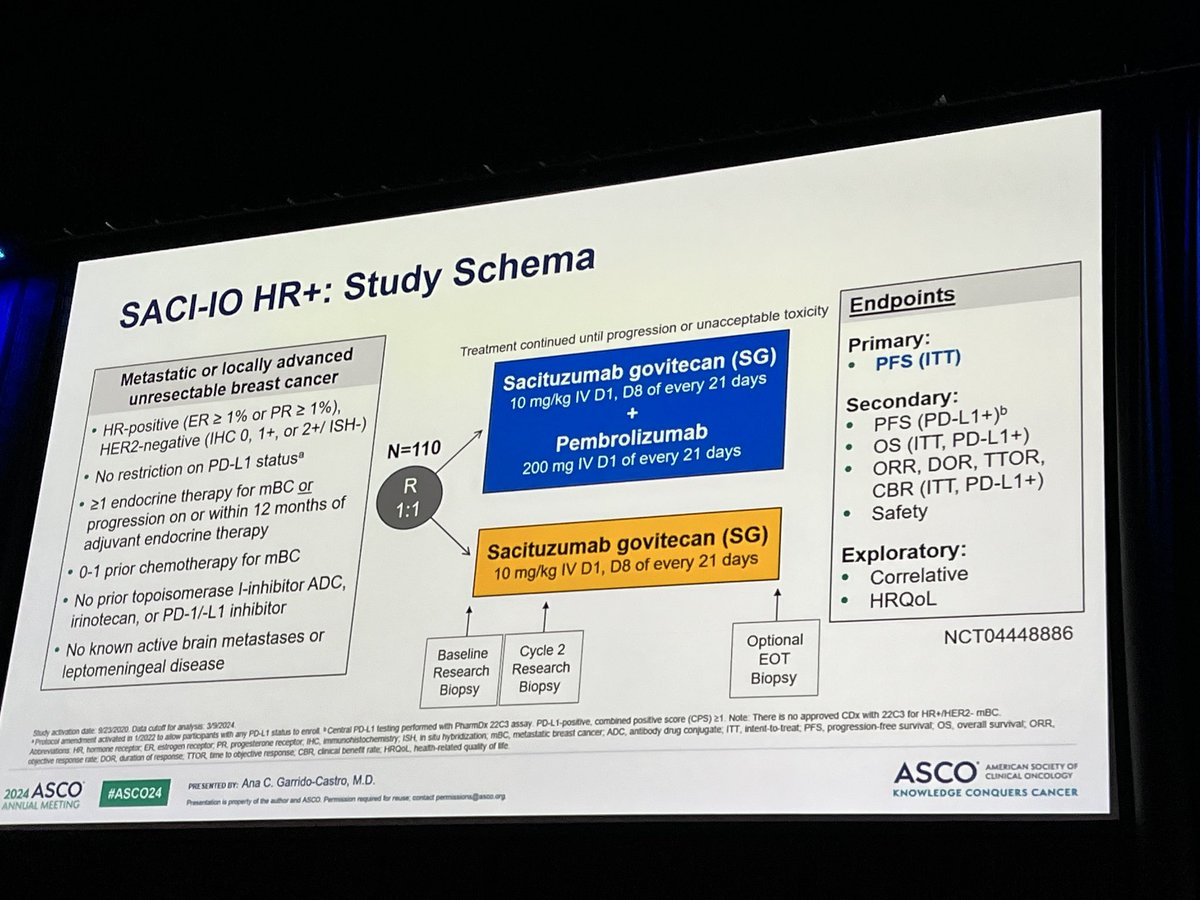
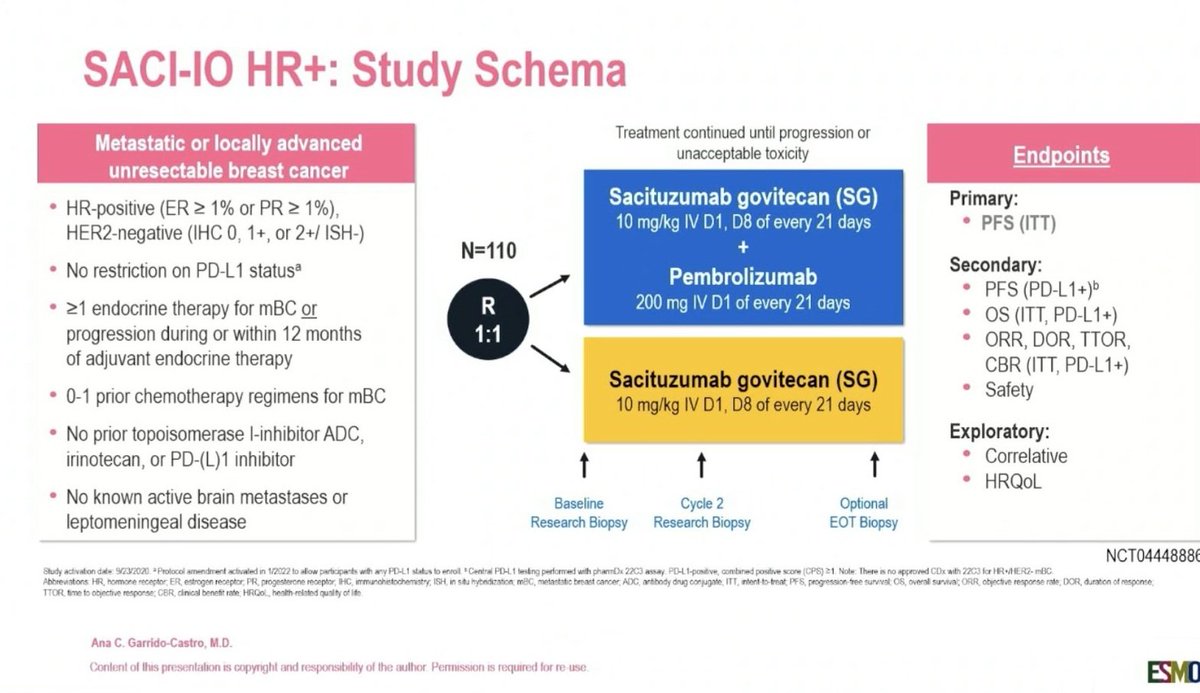
SACI-IO HR+: Study Schema
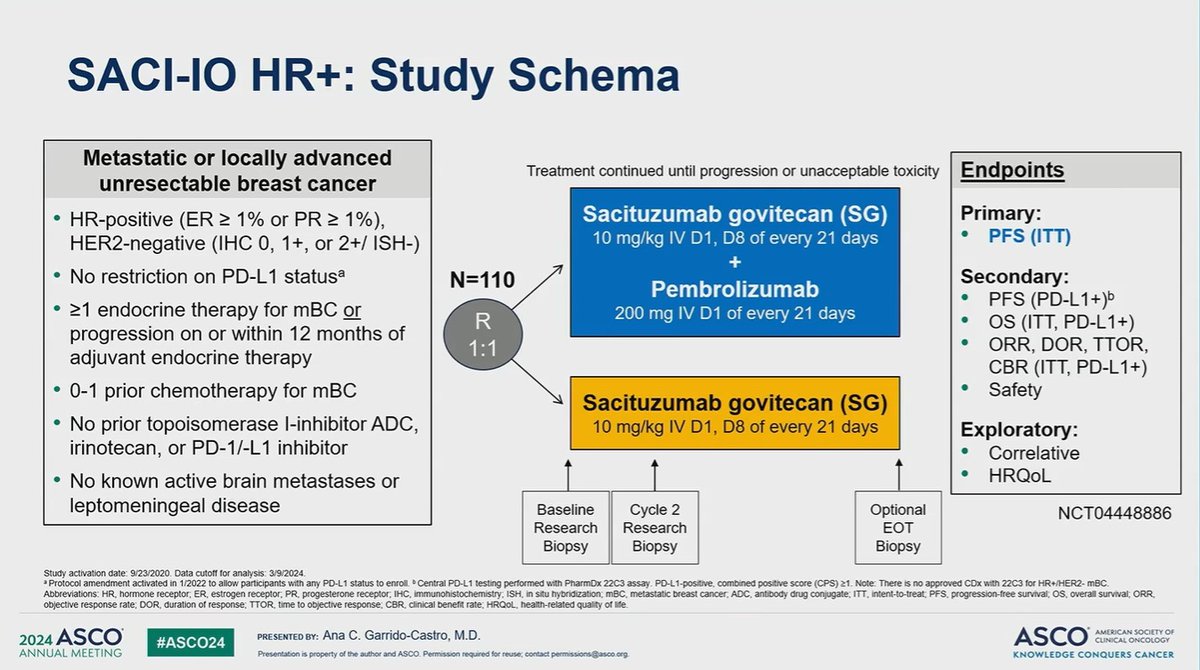
Metastatic or locally advanced unresectable breast cancer; HR-positive (ER ≥ 1% or PR ≥ 1%), HER2-negative (IHC 0, 1+, or 2+/ISH-); no restriction on PD-L1 status; ≥1 endocrine therapy for mBC or progression during or within 12 months of adjuvant endocrine therapy; 0-1 prior chemotherapy regimens for mBC; no prior topoisomerase I-inhibitor ADC, irinotecan, or PD-(L)1 inhibitor; no known active brain metastases or leptomeningeal disease.
N=110, randomized 1:1.
Arm A: Sacituzumab govitecan (SG) 10 mg/kg IV D1, D8 of every 21 days + Pembrolizumab 200 mg IV D1 of every 21 days
Arm B: Sacituzumab govitecan (SG) 10 mg/kg IV D1, D8 of every 21 days (monotherapy)
Treatment continued until progression or unacceptable toxicity.
Endpoints — Primary: PFS (ITT). Secondary: PFS (PD-L1+), OS (ITT, PD-L1+), ORR, DOR, TTOR, CBR, Safety. Exploratory: Correlative, HRQoL.
Study activation date 9/23/2020. Protocol amendment activated in 1/2022 to allow participants with any PD-L1 status to enroll. Central PD-L1 testing performed with pharmDx 22C3 assay. PD-L1-positive: combined positive score (CPS) ≥1.
NCT04448886
Ana C. Garrido-Castro, MD
[Slide 2 — FINAL ANALYSIS (ITT)]
PFS — Median PFS: 8.4 vs 6.7 months; p=0.12
SG + Pembrolizumab (N=52) SG (N=52)
N PFS events 46 45
Median PFS, mo (95% CI) 8.4 (4.5-12.5) 6.7 (3.8-8.7)
HR (95% CI) 0.78 (0.52-1.19)
p-value (log-rank test) 0.12
OS — Median OS: 22.2 vs 22.1 months; p=0.46
SG + Pembrolizumab (N=52) SG (N=52)
N OS events 37 36
Median OS, mo (95% CI) 22.2 (17.3-31.2) 22.1 (18.0-27.4)
HR (95% CI) 0.97 (0.61-1.54)
p-value (log-rank test) 0.46
Data cutoff: 12/3/2025; Median follow-up: 34.6 months.
[Slide 3 — FINAL ANALYSIS (PD-L1+ CPS ≥1, N=39)]
PFS — Median PFS: 9.7 vs 5.6 months; p=0.11
SG + Pembrolizumab (N=19) SG (N=20)
N PFS events 17 18
Median PFS, mo (95% CI) 9.7 (4.2-15.7) 5.6 (2.5-8.7)
HR (95% CI) 0.56 (0.28-1.14)
p-value (log-rank test) 0.11
OS — Median OS: 24.3 vs 17.7 months; p=0.34
SG + Pembrolizumab (N=19) SG (N=20)
N OS events 12 15
Median OS, mo (95% CI) 24.3 (17.0-NR) 17.7 (12.4-33.0)
HR (95% CI) 0.69 (0.32-1.48)
p-value (log-rank test) 0.34
Data cutoff: 12/3/2025; Median follow-up: 34.6 months. NR, not reached.
Source: ESMO Breast 2026 Abstract 424RO, Garrido-Castro, May 8, 2026 (Dana-Farber Cancer Institute / Harvard Medical School). Tweet capture via @dr_yakupergun.SACI-IO HR+ Top Tweets







Top Discussion Threads
Highest-engagement tweets about this trial, ranked by KOL discussant count (replies + quote-tweets). Replies in green, quote-tweets in blue. Wall Street, stock-promo, and non-substantive replies excluded.

SACI-IO HR+: Adding pembrolizumab to SG did not improve PFS or OS overall in HR+ MBC, but a promising signal was seen in the PD-L1+ subgroup (CPS ≥1). More exploration needed. #ESMOBreast26 https://t.co/BLTrPHWVcn







Can we add pembrolizumab to SG for metastatic HR postive Her2 negative MBC? Not much benifit of PFS . 8.4 months vs 6.2 months . Not much useful strategy. @ASCO @OncoAlert #asco24 @Larvol https://t.co/quNLaziErI





SACI-IO HR+ in pts w/PDL1 unselected HR+ MBC, pembrolizumab + sacituzumab govitecan (SG) did not improve mPFS vs SG alone (8.1 vs 6.2 months, HR 0.81, p=0.37). a non-significant trend seen among patients w/ PD-L1+ (CPS ≥1) Larger trials ongoing #ASCO24 @OncoAlert https://t.co/





Ana garrida-castro presents Saci-IO in HR+ MBC. Intriguing trend towards improved PFS and OS in CPS+ disease with SG Pembo vs SG, underpowered for significance. HR neg study ongoing! #ASCO24 @OncoAlert https://t.co/pzs5Ccjsws



Ana Garrido-Castro from @DFCI_BreastOnc presents the results of SACI-IO HR+ investigator-initiated trial. Adding pembro to SG did not improve PFS in unselected pts with HR+ MBC (8.1 vs 6.2 mo, HR 0.81), although an intriguing trend in PFS and OS was seen in the PDL1+ subgroup. ht



#ASCO24 SACI-IO: SG w/wo Pembro in pts with metastatic HR+/HER2-BC 🔍≥1 prior ET and 0-1 ChT for MBC PFS➡️8.1 vs 6.2 mo (HR 0.76 but NS) OS➡️18.5 vs 17.9 mo (immature) Addition of Pembro to SG showed a non-significant trend toward improved PFS @OncoAlert https://t.co/Hf

About the SACI-IO HR+ Trial
SACI-IO HR+ is an investigator-initiated, multicenter, randomized Phase II trial evaluating whether the addition of pembrolizumab to sacituzumab govitecan (SG, anti-Trop-2 ADC) improves outcomes versus SG alone in patients with HR+/HER2- metastatic breast cancer who had received ≥1 prior endocrine therapy and 0–1 prior lines of chemotherapy. Primary results were reported at ASCO 2024 (LBA1004, Garrido-Castro), where the trial did not meet its primary endpoint: adding pembrolizumab did not significantly improve PFS in the PD-L1-unselected ITT population (8.1 vs 6.2 months; HR 0.81; p=0.37). Final results with extended follow-up were presented at ESMO Breast Cancer 2026 (Abstract 424RO, Garrido-Castro, 8 May 2026; data cutoff 3 December 2025, median follow-up 34.6 months) and are now published in full in ESMO Open (Jul 2026), confirming no significant ITT benefit (PFS HR 0.78, p=0.12; OS HR 0.97), with the early suggestive OS trend (HR 0.65) maturing to essentially flat. A numerical, underpowered signal persisted in the exploratory PD-L1+ (CPS ≥1) subgroup. This combination is investigational: sacituzumab govitecan (Trodelvy, Gilead) monotherapy is FDA-approved in pretreated HR+/HER2- MBC (TROPiCS-02), but SG + pembrolizumab (Keytruda, Merck) is not approved in this or any setting.
SACI-IO HR+ Methodology & Results
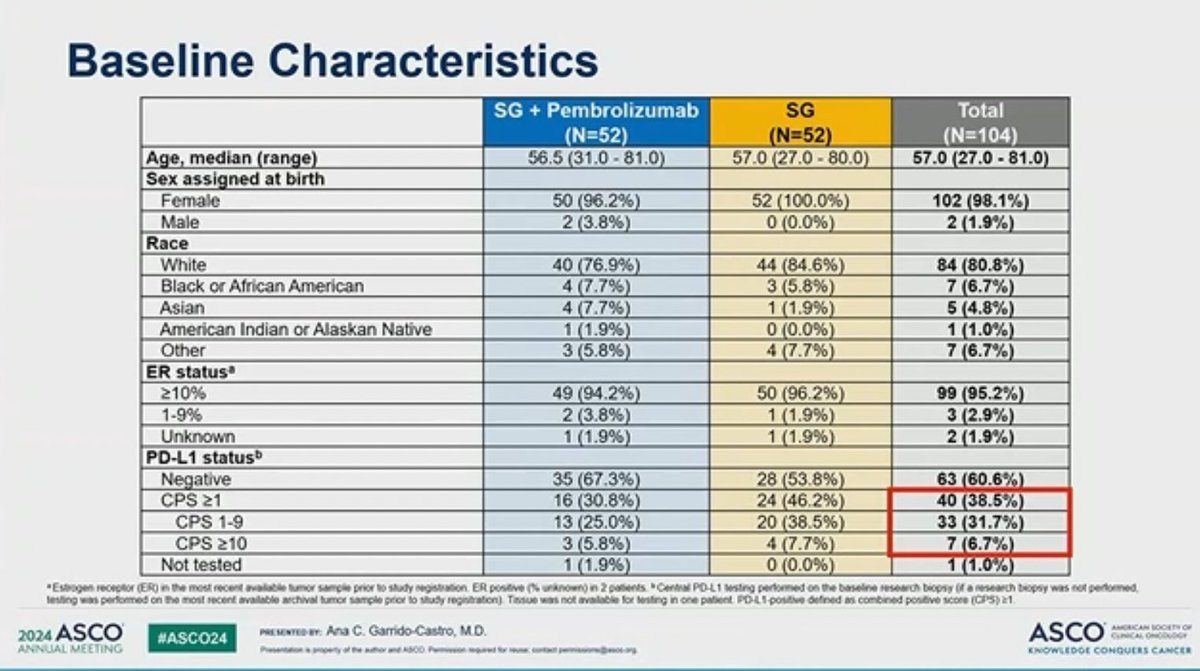
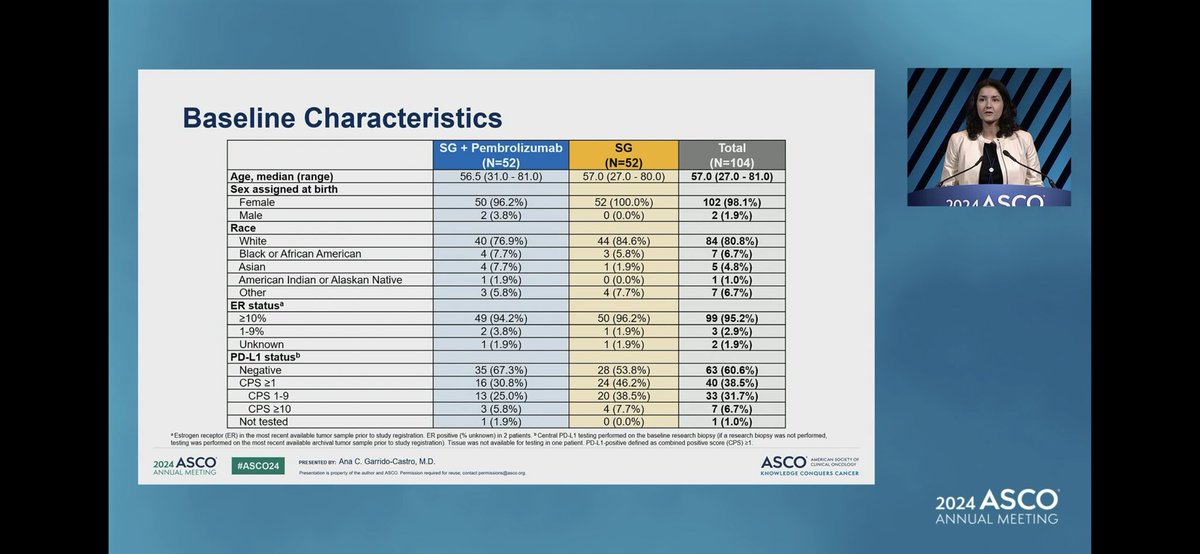
Population: Adults with HR+ (ER ≥1% and/or PR ≥1%), HER2-negative, unresectable locally advanced or metastatic breast cancer. Prior endocrine therapy ≥1 line required. 0–1 prior chemotherapy lines for metastatic disease. Excluded: prior TOPO1-inhibitor ADCs, irinotecan, or PD-1/PD-L1 inhibitors. Baseline: median age 57, 77% prior CDK4/6 inhibitor, 56% no prior chemotherapy for metastatic disease.
Interventions: Arm A: Sacituzumab govitecan 10 mg/kg IV on Days 1 and 8 + pembrolizumab 200 mg IV on Day 1 of each 21-day cycle. Arm B: Sacituzumab govitecan 10 mg/kg IV on Days 1 and 8 of each 21-day cycle (monotherapy). Treatment continued until progression or unacceptable toxicity.
Endpoints: Primary: PFS in the overall population. Secondary: PFS in PD-L1+ (CPS ≥1 by 22C3); OS; ORR; safety. Exploratory: TROP2 / PD-L1 expression correlatives.
Efficacy — ASCO 2024 primary analysis (LBA1004): primary PFS endpoint NOT met
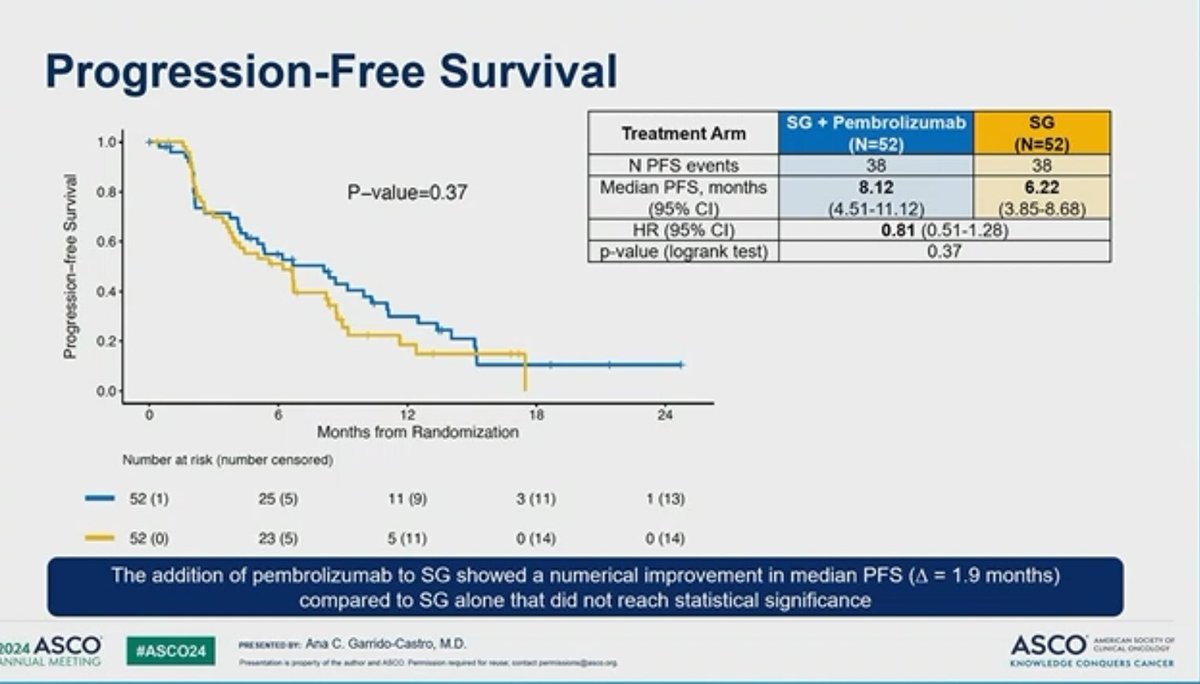
At the primary analysis (median follow-up 12.5 months), adding pembrolizumab to sacituzumab govitecan did not significantly improve PFS in the PD-L1-unselected ITT HR+/HER2- MBC population. Median PFS 8.1 vs 6.2 months; HR 0.81 (95% CI 0.51–1.28); p=0.37. Overall survival at this cut was not significant (HR 0.65, 95% CI 0.33–1.28). [ASCO 2024 LBA1004, Garrido-Castro; corroborated by @DrSGraff & @Dr_Oncologista slide OCR]
Efficacy — ESMO Breast 2026 conference final analysis (extended OS follow-up): ITT not significant (PFS HR 0.78 p=0.12; OS HR 0.97 p=0.46); PD-L1+ subgroup signal persists
ITT population (N=52 vs N=52) at final analysis: median PFS 8.4 months (95% CI 4.5–12.5) with SG + pembrolizumab vs 6.7 months (95% CI 3.8–8.7) with SG alone; HR 0.78 (95% CI 0.52–1.19); p=0.12 (log-rank); PFS events 46 vs 45. Median OS 22.2 months (95% CI 17.3–31.2) vs 22.1 months (95% CI 18.0–27.4); HR 0.97 (95% CI 0.61–1.54); p=0.46 (log-rank); OS events 37 vs 36. ORR 21.2% vs 17.3% (ASCO 2024 cut). [ESMO Breast 2026 424RO, DCO 12/3/25, FU 34.6 mo]
PD-L1+ subgroup (CPS ≥1, N=39: 19 vs 20): median PFS 9.7 months (95% CI 4.2–15.7) vs 5.6 months (95% CI 2.5–8.7); HR 0.56 (95% CI 0.28–1.14); p=0.11 (log-rank); PFS events 17 vs 18. Median OS 24.3 months (95% CI 17.0–NR) vs 17.7 months (95% CI 12.4–33.0); HR 0.69 (95% CI 0.32–1.48); p=0.34 (log-rank); OS events 12 vs 15. Numerically favourable but underpowered; not statistically significant. [ESMO Breast 2026 424RO, DCO 12/3/25, FU 34.6 mo]
Data evolution note: between the ASCO 2024 preliminary cut (DCO 1/12/2024, median FU 9.2 months) and the ESMO Breast 2026 final analysis (DCO 12/3/2025, median FU 34.6 months), the ITT OS HR moved from 0.65 (suggestive trend) to 0.97 (essentially flat). PD-L1+ subgroup signals remained directionally consistent.
Safety & Tolerability — No new safety signals; consistent with known SG and pembrolizumab class effects
"The safety profile of SG plus pembrolizumab was similar to that expected with either agent and no new safety signals were reported." One Grade 5 TEAE was reported in the SG monotherapy arm: hepatic failure (n=1), unlikely related to SG per investigator-assessed attribution. [ESMO Breast 2026 424RO, DCO 12/3/25, FU 34.6 mo]
Treatment-Emergent AEs ≥15% (Grade ≥2 / Grade 3-4), SG + Pembrolizumab (N=52) vs SG (N=52):
- Neutrophil count decreased: 69.2% (53.8%) vs 61.5% (46.2%)
- Alopecia: 44.2% vs 38.5%
- Fatigue: 38.5% (3.8%) vs 34.6% (5.8%)
- Anemia: 36.5% (7.7%) vs 28.8% (9.6%)
- WBC decreased: 28.9% (23.1%) vs 15.4% (7.7%)
- Nausea: 30.8% (3.8%) vs 32.7% (9.6%)
- Diarrhea: 25.0% (5.8%) vs 40.4% (7.7%)
- Lymphocyte count decreased: 17.3% (11.5%) vs 0% (0%) — higher in doublet
- Alk phos increased: 15.4% (1.9%) vs 11.5% (1.9%)
- Dyspnea: 15.4% (3.8%) vs 0% (0%) — higher in doublet
- Anorexia: 13.5% (0%) vs 17.3% (0%)
Clinical Implications
Interpretation (ASCO 2024 primary + ESMO Breast 2026 final analysis): The primary endpoint was negative — adding pembrolizumab did not significantly improve ITT PFS (ASCO 2024: 8.1 vs 6.2 mo, HR 0.81, p=0.37; ESMO Breast 2026 final: HR 0.78, p=0.12). With mature 34.6-month follow-up, the ITT OS hazard ratio moved from an early 0.65 to 0.97 (p=0.46) — the suggestive trend did not bear out. The PD-L1+ (CPS ≥1) subgroup signal persists numerically (PFS HR 0.56, OS HR 0.69) but remains underpowered and not statistically significant. KOL commentary below reflects the ASCO 2024 data cut and should be read in that context.
Stephanie Graff reported the SACI-IO HR+ topline cleanly: “in pts w/PDL1 unselected HR+ MBC, pembrolizumab + sacituzumab govitecan (SG) did not improve mPFS vs SG alone (8.1 vs 6.2 months, HR 0.81, p=0.37),” while flagging “a non-significant trend seen among patients w/ PD-L1+ (CPS ≥1).” Hope Rugo framed the same data more permissively, noting an “Intriguing trend towards improved PFS and OS in CPS+ disease with SG Pembo vs SG, underpowered for significance,” with the companion “HR neg study ongoing.” Paolo Tarantino similarly described “an intriguing trend in PFS and OS… seen in the PDL1+ subgroup.” Abi Siva polled the implications directly — “promising signal was seen in the PD-L1+ subgroup (CPS ≥1). More exploration needed.” Yakup Ergün noted the “Addition of Pembro to SG showed a non-significant trend toward improved PFS.” Suyog Amol Akhade dissented on practicality, calling the SG+pembro PFS gain “Not much benifit” and the regimen not a useful strategy.
SACI-IO HR+ FAQ
What is the SACI-IO HR+ trial?
SACI-IO HR+ (NCT04448886) is an investigator-initiated, randomized Phase 2 trial of the TROP-2-directed antibody-drug conjugate sacituzumab govitecan (Trodelvy), with or without the anti-PD-1 antibody pembrolizumab (Keytruda), in hormone-receptor-positive, HER2-negative metastatic breast cancer (PD-L1 unselected). It was led by Ana C. Garrido-Castro (Dana-Farber), part of the SACI-IO program by Aditya Bardia.
Did SACI-IO HR+ meet its primary endpoint?
No. SACI-IO HR+ did not meet its primary progression-free-survival endpoint. At ASCO 2024 median PFS was 8.1 versus 6.2 months (HR 0.81; p=0.37), and the final analysis (ESMO Breast 2026; 34.6-month follow-up) confirmed no significant intent-to-treat benefit (PFS HR 0.78, p=0.12; overall survival HR 0.97). Only a numerical signal favored the combination in the PD-L1-positive subgroup.
Is sacituzumab govitecan plus pembrolizumab FDA approved for HR+/HER2- breast cancer?
No. The sacituzumab govitecan (Trodelvy) plus pembrolizumab (Keytruda) combination studied in SACI-IO HR+ is investigational and not FDA approved, and the trial was negative on its primary endpoint. Sacituzumab govitecan is separately approved as monotherapy in HR+/HER2- and triple-negative metastatic breast cancer, and pembrolizumab in certain breast cancer settings, but not this combination in HR+/HER2- disease.
What does the SACI-IO HR+ PD-L1 subgroup signal mean?
Although the overall trial was negative, a numerical benefit favored adding pembrolizumab in the exploratory PD-L1-positive (CPS >=1) subgroup. This is hypothesis-generating rather than confirmatory: the subgroup was exploratory and not powered for a definitive conclusion, so it does not establish efficacy and would require prospective testing.
Is SACI-IO HR+ the same as the triple-negative SACI-IO trial?
No. This page covers the HR-positive/HER2-negative SACI-IO cohort. There is a separate SACI-IO trial in triple-negative breast cancer. The two studies address different breast cancer subtypes, and the results and interpretation for the HR-positive/HER2-negative population described here should not be conflated with the triple-negative study.
SACI-IO HR+ in the News
SACI-IO HR+: Sacituzumab Govitecan ± Pembrolizumab in HR+/HER2- MBC — Final Peer-Reviewed Results
PUBSACI-IO HR+ Final Analysis — ESMO Breast Cancer 2026 Congress Abstract
PUBSACI-IO HR+: Sacituzumab Govitecan ± Pembrolizumab in HR+/HER2- mBC (ASCO 2024 LBA1004)
MEDIAAntibody-Drug Conjugate + Checkpoint Inhibitor for PD-L1+ HR+/HER2- Breast Cancer
MEDIAGarrido-Castro Update on SACI-IO HR+ Metastatic Breast Cancer Trial
MEDIAPembrolizumab + SG: Non-Significant Trend Toward Improved PFS in HR+ Breast Cancer
TRIALClinicalTrials.gov — SACI-IO HR+ (NCT04448886)
Key KOL Sentiments — SACI-IO HR+
See how oncologists are reacting across the Trodelvy program: Physician Sentiment on TRODELVY® →