Intermediate-risk early breast cancer post-mastectomy (pT1-2 N1; pT3N0; or pT2N0 grade III and/or LVI) — Medical Research Council (MRC) / NIHR partnership; EORTC Breast Cancer Group; Dutch Cancer Society; Cancer Australia; HSBC Trustees; Breast Cancer Institute of Edinburgh; Edinburgh Cancer Centre Endowments; University of Edinburgh
Intermediate-risk early breast cancer post-mastectomy (pT1-2 N1; pT3N0; or pT2N0 grade III and/or LVI)SABCS 2024 GS2-03
Design - Phase 3 international RCT: post-mastectomy chest wall irradiation (CWI) vs no CWI, intermediate-risk early breast cancer (NCT00966888 / ISRCTN61145589), N=1,607; primary 10-year overall survival.
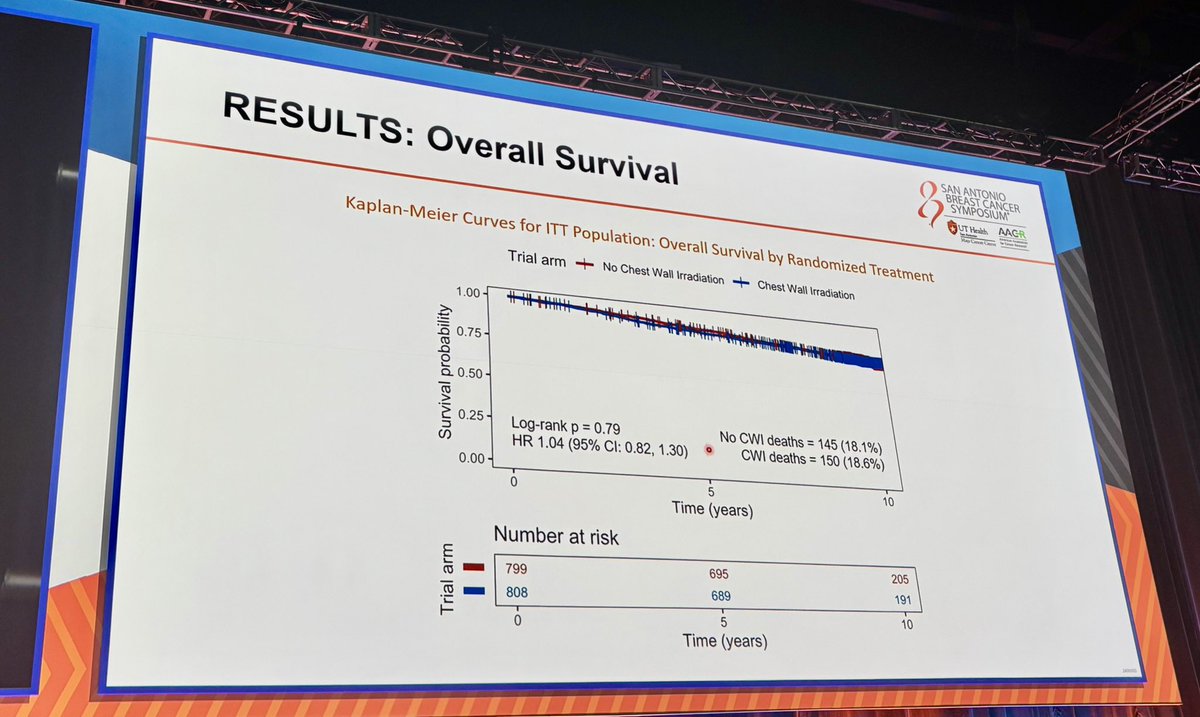
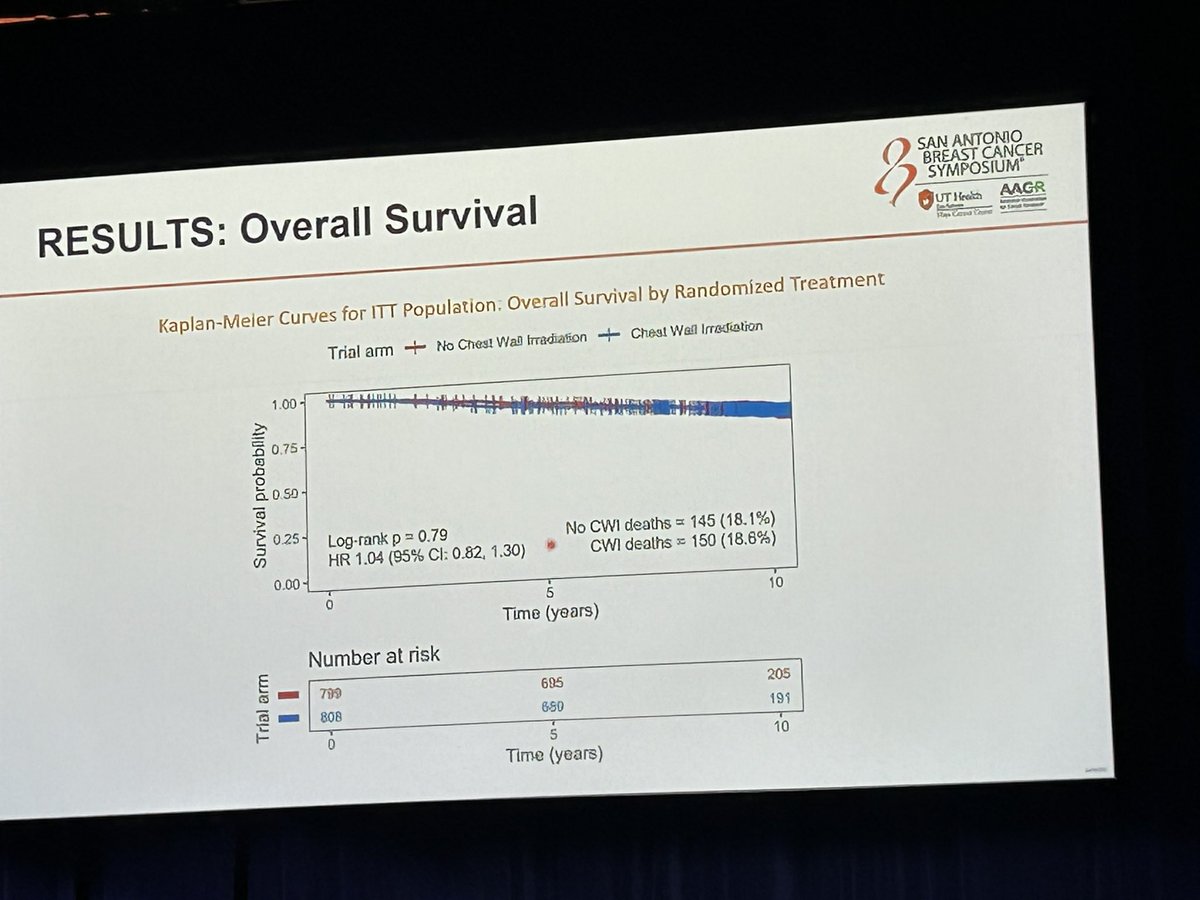
OS at 10 years (primary, NEGATIVE) - 81.4% (CWI) vs 82.0% (no CWI); HR 1.04 (95% CI 0.82-1.30) - no survival benefit from chest wall irradiation.
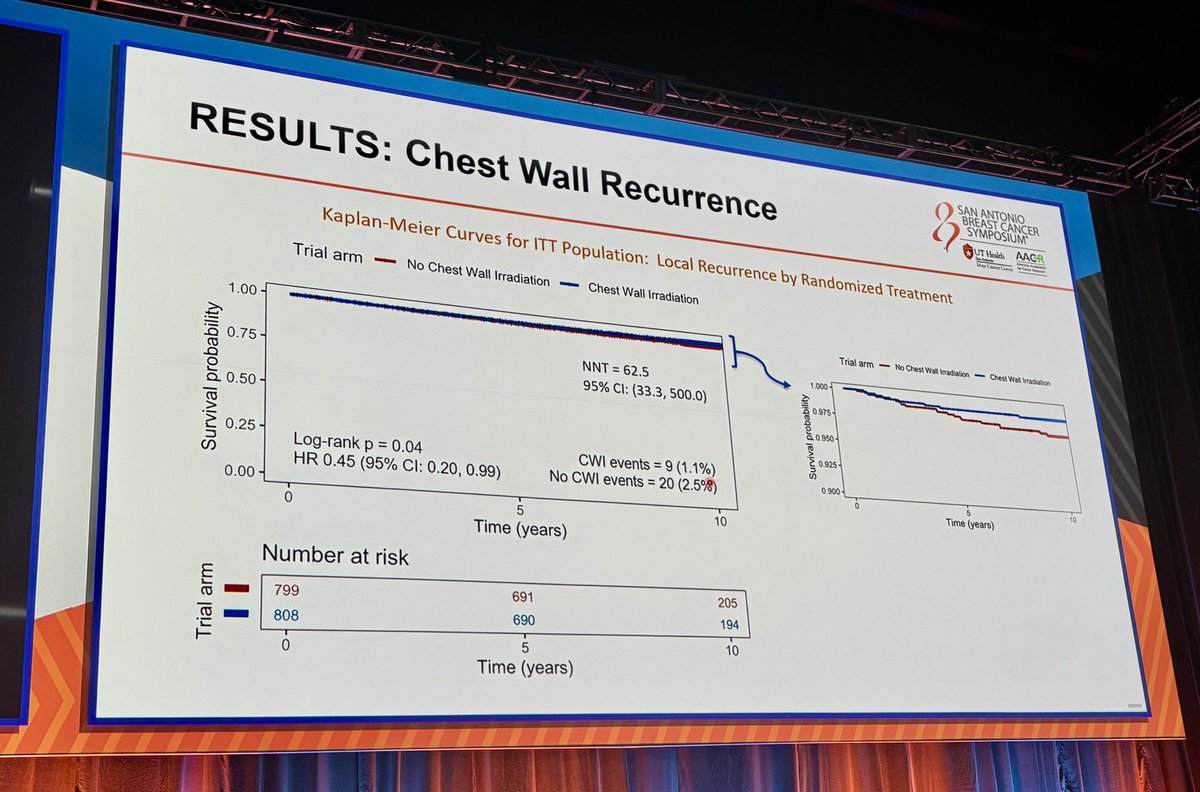
Chest wall recurrence - Few events (29 total: 9 CWI vs 20 no CWI); CWI HR 0.45 (0.20-0.99) but absolute reduction <2%, deemed clinically insignificant.
Safety - Radiotherapy safety well characterized; cardiac and lung RT exposure recorded per protocol.
Regulatory - Radiotherapy-strategy trial - no FDA drug approval; chest wall irradiation may be safely omitted in intermediate-risk disease.
Sponsor - MRC/NIHR; EORTC Breast Cancer Group (BIG 2-04).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.
Influence Leaders
Top KOLs Discussing SUPREMO / BIG 2-04 MRC
Elisabetta Bonzano MD, PhD
@to_be_elizabeth
11.8K impressions
M. Bolton
@5_utr
10.1K impressions
Wendy Woodward MDPhD
@IBCradiation
5.5K impressions
Icro Meattini
@Icro_Meattini
4.3K impressions
Chelain Goodman, MD PhD
@ChelainG
3.2K impressions
Harold J. Burstein, MD, PhD, FASCO
@DrHBurstein
2.8K impressions
Conference Presentations
SUPREMO / BIG 2-04 MRC Key Slides & Visuals
Official trial slides and relevant visuals shared by KOLs at SABCS 2024 GS2-03. Click any image to expand.
[Slide 1]
BREAST CANCER
RESULTS: Overall Survival
SYMPOSIUM
UT Health
AACR
to
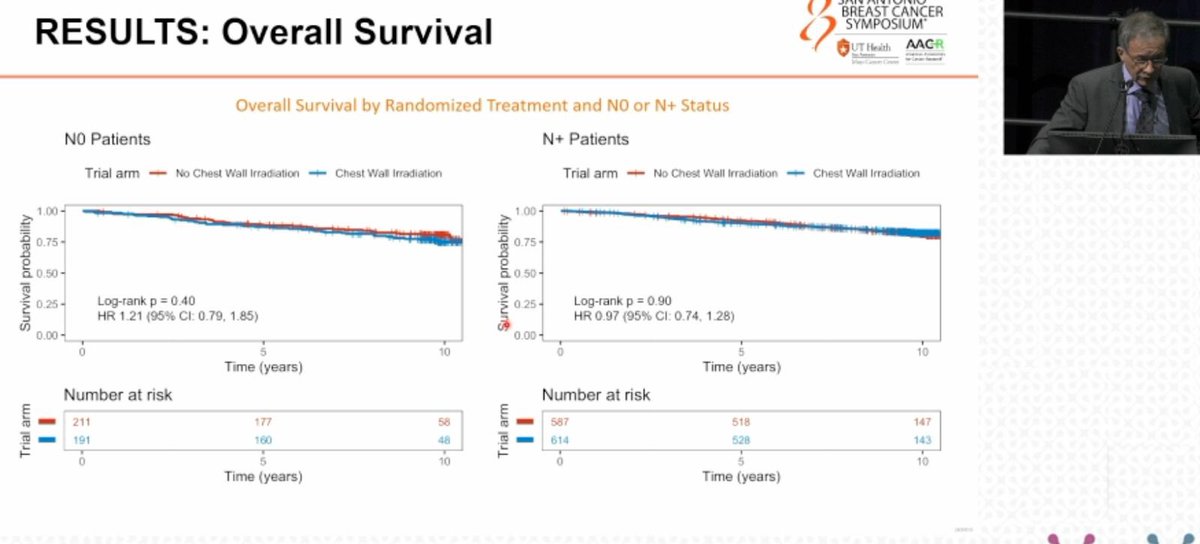
Overall Survival by Randomized Treatment and NO or N+ Status
NO Patients
N+ Patients
Trial arm
No Chest Wall Irradiation
Chest Wall Irradiation
Trial arm
No Chest Wall Irradiation
Chest Wall Irradiation
1.00
1.00
Survival probability
0.75
0.50
0.25
Survival probability
0.75
0.50
Log-rank P = 0.40
0.25
Log-rank P = 0.90
HR 1.21 (95% Cl: 0.79. 1.85)
HR 0.97 (95% CI: 0.74, 1.28)
0.00
0.00
0
5
10
0
5
10
Time (years)
Time (years)
Number at risk
Number at risk
Trial arm
211
177
58
Trial arm
587
518
147
191
160
48
614
528
143
0
5
10
0
5
10
Time (years)
Time (years)
---
[Slide 2]
SAN ANTONIO
BREAST CANCER
RESULTS: Regional Recurrence
SYMPOSIUM
UT Health
AACR
-
I
I
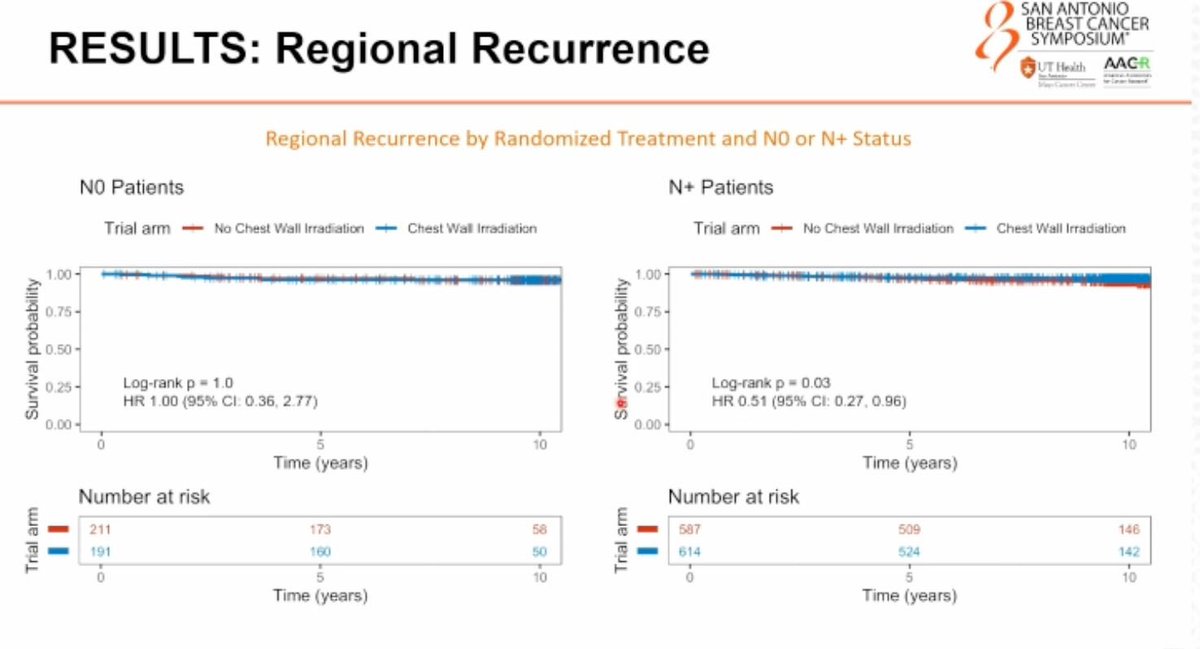
Regional Recurrence by Randomized Treatment and NO or N+ Status
NO Patients
N+ Patients
Trial arm
No Chest Wall Irradiation
Chest Wall Irradiation
Trial arm
No Chest Wall Irradiation
Chest Wall Irradiation
1.00
1.00
Survival probability
0.75
0.50
Log-rank P - 1.0
Servival probability
0.75
0.50
0.25
0.25
Log-rank P - 0.03
HR 1.00 (95% Cl: 0.36, 2.77)
HR 0.51 (95% Cl: 0.27. 0.96)
0.00
0.00
0
5
10
0
5
10
Time (years)
Time (years)
Number at risk
Number at risk
Trial arm
211
173
58
Trial arm
587
509
146
191
160
50
614
524
142
0
5
10
0
5
10
Time (years)
Time (years)
---
[Slide 3]
BREAST CANCER
SYMPOSIUM
RESULTS: Metastasis-free & Disease-free Survival
UT Health AACR
-
December 10-13, 2024
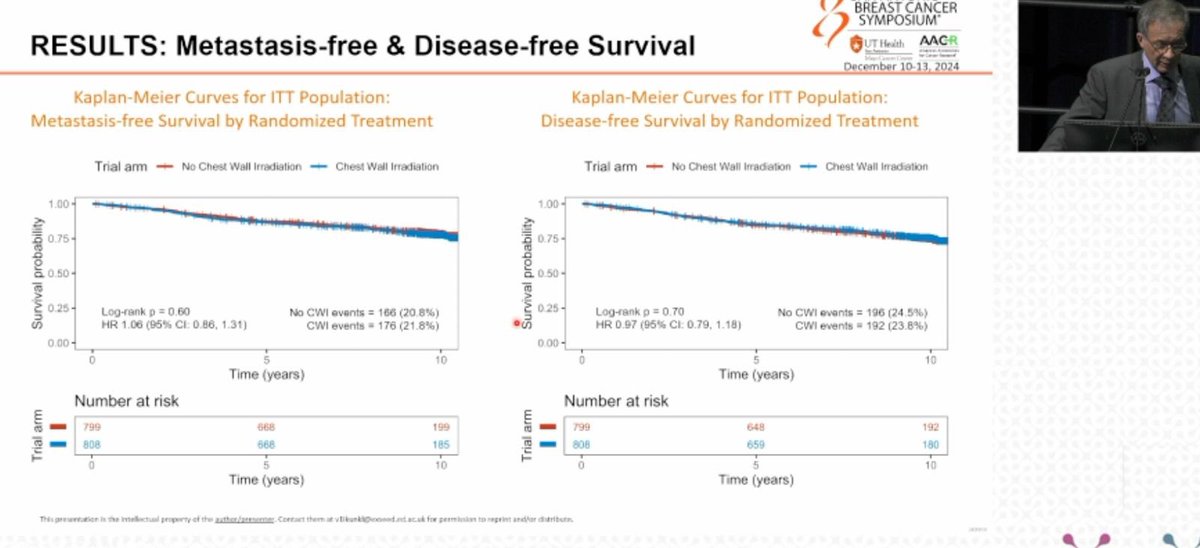
Kaplan-Meier Curves for ITT Population:
Kaplan-Meier Curves for ITT Population:
Metastasis-free Survival by Randomized Treatment
Disease-free Survival by Randomized Treatment
Trial arm
No Chest Wall Irradiation
Chest Wall Irradiation
Trial arm
No Chest Wall Irradiation
Chest Wall Irradiation
1.00
1.00
Survival probability
0.75
0.50
Survival probability
0.75
0.50
0.25
Log-rank D = 0.60
No CWI events = 166 (20.8%)
0.25
Log-rank p = 70
No CWI events = 196 (24.5%)
HR 1.06 (95% CI: 0.86, 1.31)
CWI events - 176 (21.8%)
HR 0.97 (95% CI: 0.79. 1.18)
CWI events - 192 (23.8%)
0.00
0.00
0
5
10
0
5
10
Time (years)
Time (years)
Number at risk
Number at risk
Trial arm
799
668
199
Trial arm
799
648
192
808
668
185
808
659
180
0
5
10
0
5
10
Time (years)
Time (years)
This presentation is the intellectual property of the author/prenerner Contact them - nt for perminare to reprint and/or distribute
---
[Slide 4]
SAN ANTONIO
BREAST CANCER
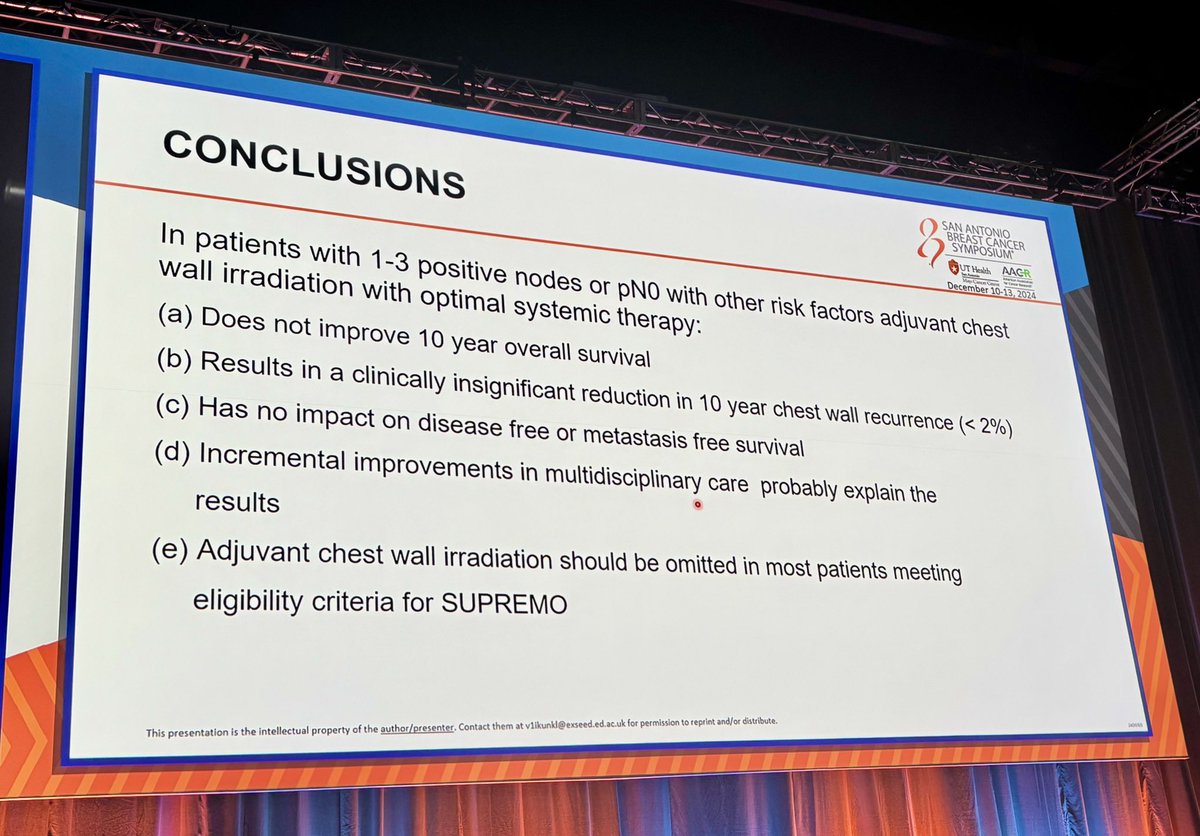
CONCLUSIONS
SYMPOSIUM
UT Health AACR
-
Internal
- -
December 10-13, 2024
In patients with 1-3 positive nodes or pN0 with other risk factors adjuvant chest
wall irradiation with optimal systemic therapy:
(a) Does not improve 10 year overall survival
(b) Results in a clinically insignificant reduction in 10 year chest wall recurrence (< 2%)
(c) Has no impact on disease free or metastasis free survival
(d) Incremental improvements in multidisciplinary care probably explain the
results
(e) Adjuvant chest wall irradiation should be omitted in most patients meeting
eligibility criteria for SUPREMO
This presentation is the intellectual property of the author/presentes Contact them if ed acade for permission to reprint and/or distribute.
[Slide 1]
SAN ANTONIO
BREAST CANCER
CONCLUSIONS
SYMPOSIUM
UT Health AACR
-
I
-
-
December 10-13, 2024
In patients with 1-3 positive nodes or pNO with other risk factors adjuvant chest
wall irradiation with optimal systemic therapy:
(a) Does not improve 10 year overall survival
(b) Results in a clinically insignificant reduction in 10 year chest wall recurrence (< 2%)
(c) Has no impact on disease free or metastasis free survival
(d) Incremental improvements in multidisciplinary care probably explain the
results
(e) Adjuvant chest wall irradiation should be omitted in most patients meeting
eligibility criteria for SUPREMO
This presentation is the Intellectual property of the author/presenter. Contact them at v1ikunki@exseed.ed.ac.uk for permission to reprint and/or distribute.
[Slide 1]
SAN ANTONIO
CONCLUSIONS
BREAST CANCER
SYMPOSIUM
UT Health
AACR
-
December 10-13, 2024
In patients with 1-3 positive nodes or pNO with other risk factors adjuvant chest
wall irradiation with optimal systemic therapy:
(a) Does not improve 10 year overall survival
(b) Results in a clinically insignificant reduction in 10 year chest wall recurrence (< 2%)
(c) Has no impact on disease free or metastasis free survival
(d) Incremental improvements in multidisciplinary care probably explain the
results
(e) Adjuvant chest wall irradiation should be omitted in most patients meeting
eligibility criteria for SUPREMO
This presentation is the intellectual property of the author/presenter. Contact them at v1ikunkl@exseed.ed.ac.uk for permission to reprint and/or distribute.
---
[Slide 2]
SAN ANTONIO
RESULTS: Overall Survival
BREAST CANCER
SYMPOSIUM
UT Health
AACR
before
Rej Case Center
Kaplan-Meier Curves for ITT Population: Overall Survival by Randomized Treatment
Trial arm
No Chest Wall Irradiation
Chest Wall Irradiation
1.00
0.75
0.50
0.25
Log-rank p = 0.79
No CWI deaths = 145 (18.1%)
HR 1.04 (95% CI: 0.82, 1.30)
CWI deaths = 150 (18.6%)
0.00
0
5
10
Time (years)
Number at risk
799
695
205
808
689
191
0
5
10
Time (years)
---
[Slide 3]
SAN ANTONIO
BREAST CANCER
RESULTS: Chest Wall Recurrence
SYMPOSIUM?
UT Health
AACR
Kaplan-Meier Curves for ITT Population: Local Recurrence by Randomized Treatment
Trial arm
-
No Chest Wall Irradiation
Chest Wall Irradiation
1.00
Trial arm - No Chest Wall Irradiation - Chest Wall Irradiation
0.75
NNT = 62.5
1,000
95% CI: (33.3, 500.0)
0.975
0.50
0.950
0.25
0.925
Log-rank p = 0.04
CWI events = 9 (1.1%)
HR 0.45 (95% CI: 0.20, 0.99)
No CWI events = 20 (2.5%)
0.900
0
5
10
0.00
Time (years)
0
5
10
Time (years)
Number at risk
799
691
205
808
690
194
0
5
10
Time (years)
---
[Slide 4]
SAN ANTONIO
BREAST CANCER
SYMPOSIUM
DECEMBER 10-13, 2024
AAGR
HENRY a. GONZALE CONVENTION CENTER SAN ANTONIO, TX
UT Health
Does postmastectomy radiotherapy in 'intermediate-risk' breast cancer
impact overall survival? 10 year results of the BIG 2-04 MRC randomized
trial on behalf of the SUPREMO trial investigators
lan Kunkler, FRCR
Institute of Genetics and Cancer
University of Edinburgh
Medical
Research
MRC
Council
11/11
---
[Slide 5]
SAN ANTONIO
BREAST CANCER
RESULTS: Overall Survival
SYMPOSIUM*
UT Health
AAGR
-
-
-
I I I
Kaplan-Meier Curves for ITT Population: Overall Survival by Randomized Treatment
Trial arm
No Chest Wall Irradiation
+
Chest Wall Irradiation
1.00
Survival probability
0.75
0.50
0.25
Log-rank p = 0.79
No CWI deaths = 145 (18.1%)
HR 1.04 (95% Cl: 0.82, 1.30)
CWI deaths = 150 (18.6%)
0.00
0
5
10
Time (years)
Number at risk
Trial arm
799
695
205
808
689
191
0
5
10
Time (years)
---
[Slide 6]
SAN ANTONIO
BREAST CANCER
RESULTS: Chest Wall Recurrence
SYMPOSIUM*
UT Health
AACR
I
-
- -
I I
Kaplan-Meier Curves for ITT Population: Local Recurrence by Randomized Treatment
Trial arm
No Chest Wall Irradiation
Chest Wall Irradiation
1.00
Trial arm
No Chest Wall Irradiation
Chest Wall Irradiation
NNT = 62.5
1.000
Survival probability
0.75
95% Cl: (33.3, 500.0)
Survival probability
0.975
0.50
0.950
0.925
0.25
Log-rank p = 0.04
CWI events = 9 (1.1%)
HR 0.45 (95% Cl: 0.20, 0.99)
No CWI events = 20 (2.5%)
0.900
0
5
10
0.00
Time (years)
0
5
10
Time (years)
Number at risk
Trial arm
799
691
205
808
690
194
0
5
10
Time (years)
---
[Slide 7]
SAN ANTONIO
BREAST CANCER
CONCLUSIONS
SYMPOSIUM*
UT Health AACR
-
Market
I I I
- -
December 10-13, 2024
In patients with 1-3 positive nodes or pN0 with other risk factors adjuvant chest
wall irradiation with optimal systemic therapy:
(a) Does not improve 10 year overall survival
(b) Results in a clinically insignificant reduction in 10 year chest wall recurrence (< 2%)
(c) Has no impact on disease free or metastasis free survival
(d) Incremental improvements in multidisciplinary care probably explain the
results
(e) Adjuvant chest wall irradiation should be omitted in most patients meeting
eligibility criteria for SUPREMO
This presentation is the intellectual property of the author/presenter. Contact them at v1ikunkl@exsed.ed.ac.uk for permission to reprint and/or distribute.
[Slide 1]
SAN ANTONIO
BREAST CANCER
CONCLUSIONS
SYMPOSIUM
UT Health
AAGR
-
- -
-
December 10-13, 2024
In patients with 1-3 positive nodes or pNO with other risk factors adjuvant chest
wall irradiation with optimal systemic therapy:
(a) Does not improve 10 year overall survival
(b) Results in a clinically insignificant reduction in 10 year chest wall recurrence (< 2%)
(c) Has no impact on disease free or metastasis free survival
(d) Incremental improvements in multidisciplinary care probably explain the
results
(e) Adjuvant chest wall irradiation should be omitted in most patients meeting
eligibility criteria for SUPREMO
This proventation b Do interfection property of the Contact Non d United adadas - perovasion to reprint tritter distribute
---
[Slide 2]
SAN ANTONIO
BREAST CANCER
RESULTS: Overall Survival
SYMPOSIUM"
UT Health
AAGR
-
- - -
Tax Cana Charge
Kaplan-Meler Curves for ITT Population: Overall Survival by Randomized Treatment
Trial arm
+
No Chest Wall Irradiation
Chest Wall Imediation
1.00
Survival probability
0.75
0.50
0.25
Log-rank P = 0.79
No CWI deaths = 145 (18.1%)
HR 1.04 (95% Cl: 0.82, 1.30)
CWI deaths = 150 (18.6%)
0.00
0
5
10
Time (years)
Number at risk
Trial arm
799
695
205
808
680
191
0
5
10
Time (years)
---
[Slide 3]
Main eligibility criteria
SAN ANTONIO
BREAST CANCER
SYMPOSIUM
UT Isalth
AAGR
-
- -
-
-
December 10-13, 2024
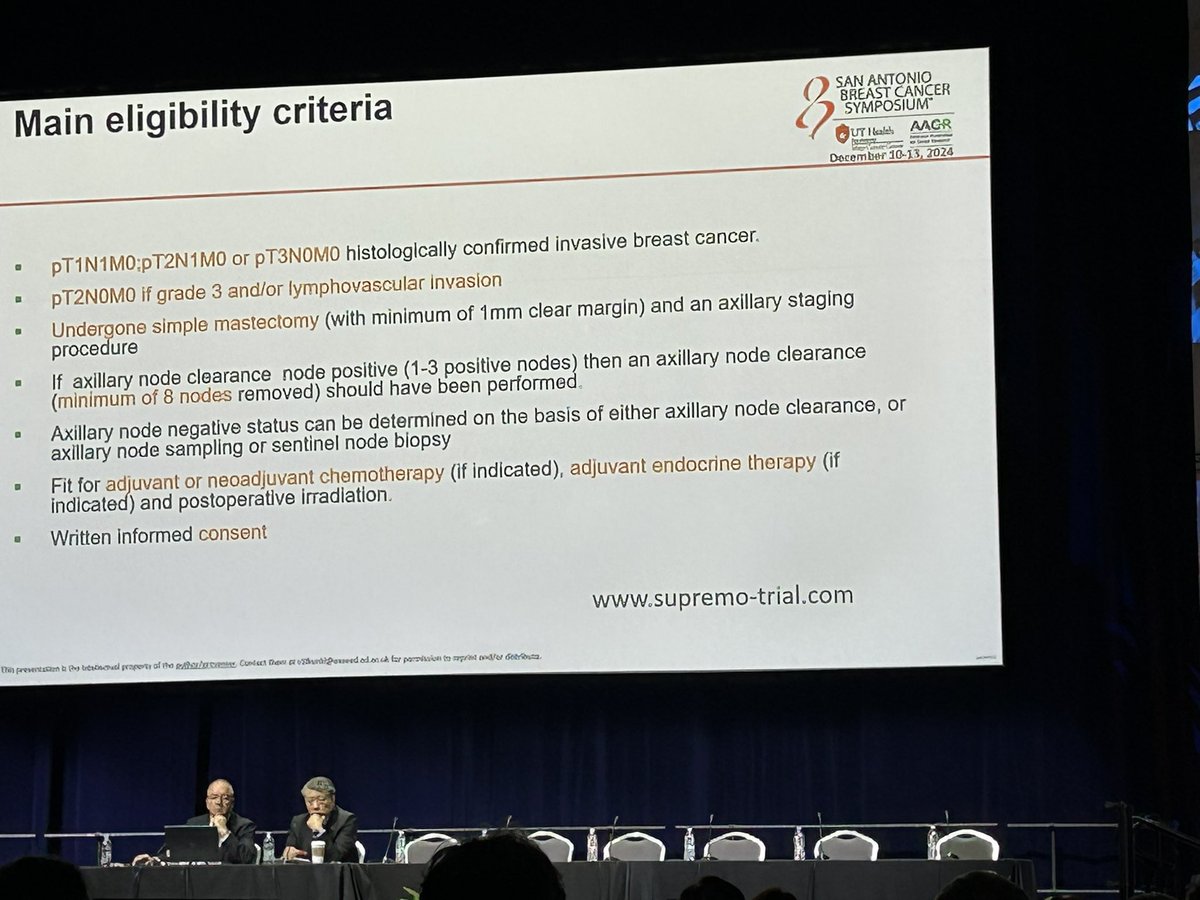
pT1N1M0;pT2N1M0 or pT3NOMO histologically confirmed invasive breast cancer.
pT2N0M0 if grade 3 and/or lymphovascular invasion
Undergone simple mastectomy (with minimum of 1mm clear margin) and an axillary staging
procedure
If axillary node clearance node positive (1-3 positive nodes) then an axillary node clearance
(minimum of 8 nodes removed) should have been performed.
Axillary node negative status can be determined on the basis of either axillary node clearance, or
axillary node sampling or sentinel node biopsy
Fit for adjuvant or neoadjuvant chemotherapy (if indicated), adjuvant endocrine therapy (if
indicated) and postoperative irradiation.
Written informed consent
www.supremo-trial.com
this prevention b (he interved property of the Condect Dear a od and for permission to reprint Getributz
SUPREMO is the definitive Phase 3 trial evaluating whether post-mastectomy chest wall irradiation (CWI) is needed for intermediate-risk breast cancer (1-3 positive nodes, or node-negative with high-risk features like grade 3 / LVI). At 9.6 years median follow-up, NO survival benefit from CWI (81.4% vs. 82.0% 10-yr OS, HR 1.04). Although CWI reduced chest wall recurrence risk by half, the absolute benefit was <2% — clinically insignificant. Results important for shared decision-making: many eligible patients may safely AVOID CWI. Reinforces the movement to minimize radiation exposure in intermediate-risk BC, complementing PRIME II (RT omission in 65+), CALGB 9343 (70+), and IDEA (RT omission by genomic risk).
Median: 81.4 % 10-year OS (chest wall irradiation (CWI)) vs. 82.0 % 10-year OS (no CWI). HR 1.04 (95% CI 0.82-1.30) 10-year OS rate: 81.4% (CWI) vs. 82.0% (no CWI). Median follow-up (years) rate: 9.6% (years). Phase 3 international RCT (ISRCTN61145589). N=1,607 randomized (CWI 808, no CWI 799) between April 2006 and April 2013. Population: intermediate-risk post-mastectomy BC — pT1-2 N1; pT3N0; or pT2N0 grade III and/or LVI. CWI: 50 Gy/25 fx or 40 Gy/15 fx equivalent. Median follow-up 9.6 years. Primary endpoint 10-year OS: 81.4% (CWI) vs. 82.0% (no CWI), HR 1.04 (95% CI 0.82-1.30) — NO difference. Endpoint NOT MET. No survival benefit from CWI in this population. Kunkler et al., SABCS 2024 GS2-03.
❌ 10-yr OS 81.4% CWI vs 82.0% no CWI (HR 1.04, not significant)
HR 1.04 (95% CI 0.82-1.30) Primary 10-year OS endpoint not met (see above). Secondary: chest wall recurrence events only 29 total (9 CWI, 20 no CWI); CWI HR 0.45 (95% CI 0.20-0.99), but absolute rate reduction <2% — investigator deemed clinically insignificant. 98.8% vs. 97.1% chest wall recurrence-free survival. No differential treatment effect in pN1 vs. pN0 (P for interaction = 0.13). Limitations: low accrual of pT3N0 disease, better-than-anticipated overall survival.
Radiotherapy safety well-characterized. Specific CWI acute/late toxicity endpoints (skin reactions, pneumonitis, cardiac events, secondary malignancy) not emphasized in primary results — focus was OS. Cardiac and lung RT exposure were recorded per protocol.
❌ Negative: Post-mastectomy CWI has no impact on 10-year OS in intermediate-risk BC. Omission may be safe. SUPREMO is the definitive Phase 3 trial evaluating whether post-mastectomy chest wall irradiation (CWI) is needed for intermediate-risk breast cancer (1-3 positive nodes, or node-negative with high-risk features like grade 3 / LVI). At 9.6 years median follow-up, NO survival benefit from CWI (81.4% vs. 82.0% 10-yr OS, HR 1.04). Although CWI reduced chest wall recurrence risk by half, the absolute benefit was <2% — clinically insignificant. Results important for shared decision-making: many eligible patients may safely AVOID CWI. Reinforces the movement to minimize radiation exposure in intermediate-risk BC, complementing PRIME II (RT omission in 65+), CALGB 9343 (70+), and IDEA (RT omission by genomic risk).
Frequently Asked Questions
SUPREMO / BIG 2-04 MRC FAQ
What is the SUPREMO trial?
SUPREMO (BIG 2-04) is a Phase 3 international randomized trial (NCT00966888; ISRCTN61145589) that tested whether post-mastectomy chest wall irradiation improves outcomes in intermediate-risk early breast cancer (for example, 1-3 positive nodes, or node-negative disease with high-risk features). About 1,607 patients were randomized, and 10-year overall survival was the primary endpoint.
Did SUPREMO show a benefit from chest wall irradiation?
No. SUPREMO was negative for its primary endpoint. Ten-year overall survival was 81.4% with chest wall irradiation versus 82.0% without it (HR 1.04; 95% CI 0.82-1.30) - no survival difference - suggesting that chest wall irradiation may be safely omitted in this intermediate-risk group.
What about local (chest wall) recurrence?
Chest wall recurrence events were very few (29 total: 9 with irradiation versus 20 without). While the hazard ratio favored irradiation (HR 0.45; 95% CI 0.20-0.99), the absolute reduction was less than 2%, which the investigators judged clinically insignificant given the lack of any overall-survival benefit.
Is there a drug or FDA approval involved in SUPREMO?
No. SUPREMO is a radiotherapy-strategy trial with no drug and no FDA approval question. Its findings inform radiation oncology practice - specifically, when post-mastectomy chest wall irradiation can be omitted in intermediate-risk early breast cancer.
Which patients does SUPREMO apply to?
SUPREMO enrolled intermediate-risk early breast cancer after mastectomy - pT1-2 with 1-3 positive nodes (pN1), pT3N0, or pT2N0 with grade III and/or lymphovascular invasion. The results should not be extrapolated to higher-risk disease (for example, 4 or more positive nodes), where post-mastectomy radiotherapy remains standard.