Phase III capivasertib + fulvestrant in HR+/HER2- AKT-pathway altered metastatic breast cancer. FDA-approved Nov 2023; ESMO Breast 2026 final OS not significant, PFS2 wins.
Discover KOL Sentiment on CAPItello-291 →Design - Phase 3 capivasertib (Truqap, AKT inhibitor) + fulvestrant vs placebo + fulvestrant, HR+/HER2- advanced breast cancer post-endocrine therapy (NCT04305496); primary PFS overall + AKT-pathway-altered subgroup.
PFS (biomarker subgroup) - Median 7.3 vs 3.1 mo, HR 0.50 in the PIK3CA/AKT1/PTEN-altered subgroup (n=289) - the basis for approval.
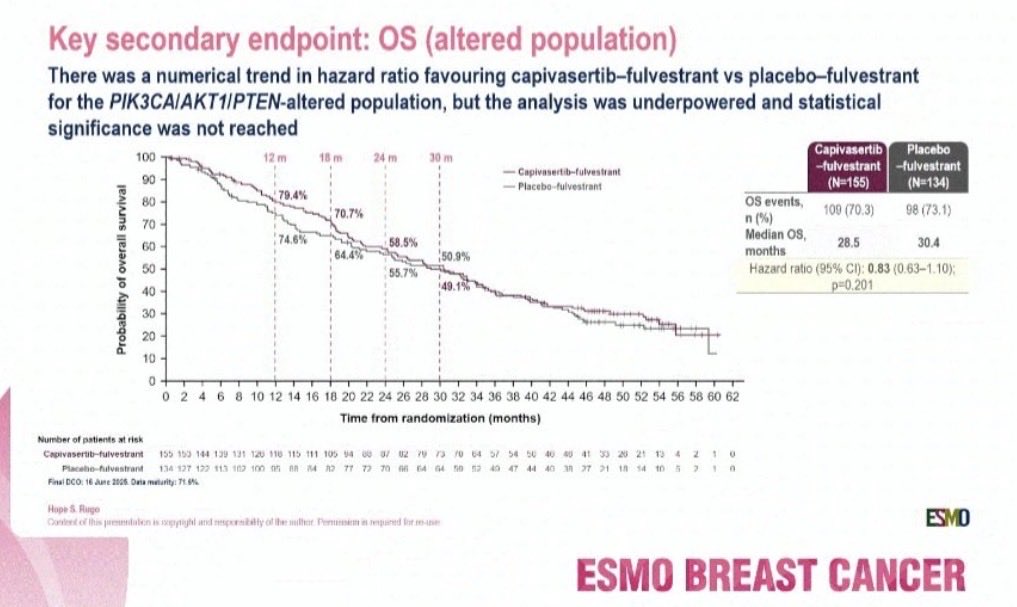
OS (final, ESMO Breast 2026) - Final overall survival update was NOT statistically significant per the page; benefit rests on PFS. PFS2 favorable.
Biomarker - Approval limited to tumors with >=1 PIK3CA, AKT1 or PTEN alteration; companion diagnostic FoundationOne CDx.
Regulatory - FDA approved November 17, 2023 (Truqap + fulvestrant) for the PIK3CA/AKT1/PTEN-altered population.
Sponsor / drug - AstraZeneca; capivasertib (Truqap) + fulvestrant (Faslodex).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.






Trial slides shared by KOLs at ESMO Breast 2026 (#ESMOBreast26). Click any image to expand. OCR text extracted via AWS Textract.
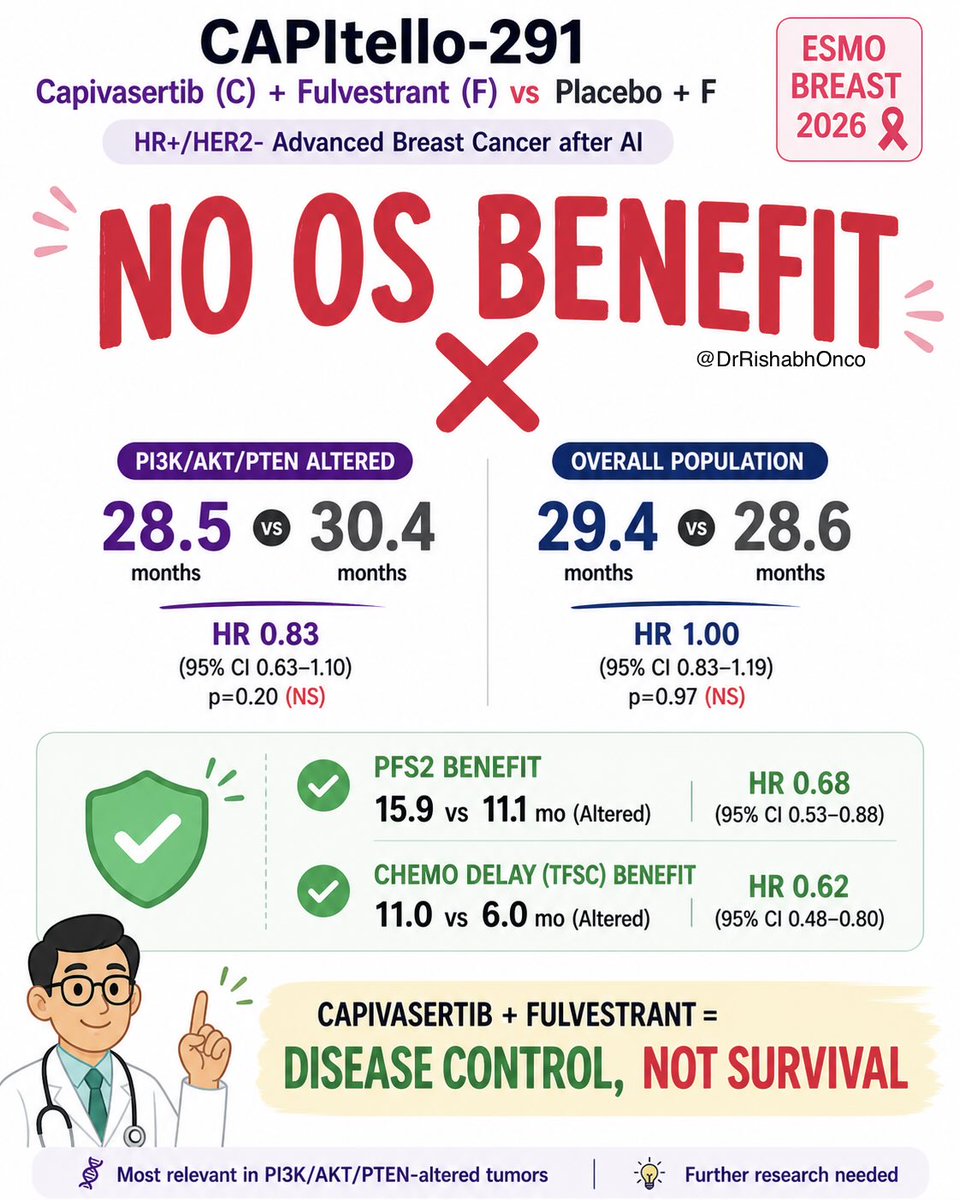
[Slide 1] CAPItello-291 ESMO Capivasertib (C) + Fulvestrant (F) vs Placebo + F BREAST 2026 HR+/HER2- Advanced Breast Cancer after AI & NO OS BENEFIT @DrRishabhOnco PI3K/AKT/PTEN ALTERED OVERALL POPULATION 28.5 vs vs 30.4 29.4 vs vs 28.6 months months months months HR 0.83 HR 1.00 (95% CI 0.63-1.10) (95% CI 0.83-1.19) p=0.20 (NS) p=0.97 (NS) PFS2 BENEFIT HR 0.68 15.9 vs 11.1 mo (Altered) (95% CI 0.53-0.88) CHEMO DELAY (TFSC) BENEFIT HR 0.62 11.0 vs 6.0 mo (Altered) (95% CI 0.48-0.80) CAPIVASERTIB + FULVESTRANT = DISEASE CONTROL, NOT SURVIVAL Most relevant in PI3K/AKT/PTEN-altered tumors Further research needed



[Slide 1] PIK3CA/AKT1/PTEN alteration concordance SAN ANTONIO BREAST CANCER SYMPOSIUM between ctDNA and tissue UT Health AACR - - - - - Map Case Case Comparison of tissue and ctDNA detected ctDNA methylation tumor fraction p<0.0001 Samples (n) 100 OPA PPA 0 50 100 150 200 250 300 350 400 10 Any 83.3 76.7 207 30 42 63 17 PIK3CAIAKT1IPTEN alteration ctDNA TF (%, log scale) 1 0.1 * 0.01 PIK3CA/AKT1/PTEN alterations Not detected Non shedders were detected by ctDNA alone in 72/700 patients (10.3%) Positive by ctDNA Positive tissue only and tissue (non-altered by (n=207) clDNA, n=63) Number of patients by TF %, n (%) Positive by ctDNA Positive ctDNA only Positive ctDNA only N 0 >0-0.1 >0.1-1 >1-10 >10 and tissue (non-altered by tissue) by tissue) ctDNA+/Tissue+ 207 0 (0) 3 (1) 38 (18) 81 (39) 85 (41) Positive tissue only Positive tissue only Tot of patients with available ctDNA-/Tissue+ 63 18 (29) 13 (21) 14 (22) 11 (17) 7 (11) (non-altered by ctDNA) (unknown by ctDNA) tissu NA results: N=558 Concordance calculated using tissue results as the reference, excluding un and PPA calculated based on total number of patients with available tissue and/or ctDNA results (N=700). AKT1, AKT serine/threonine kinase; ctDNA circulating tumor DNA; on reament; PIK3CA, phosphatidy/inositol-4,5-bisphosphate 3-kinase catalytic subunit alpha; PPA, percentage positive agreement; PTEN, phosphatase and tensin hom --- [Slide 2] PIK3CA/AKT1/PTEN alteration concordance SAN ANTONIO BREAST CANCER SYMPOSIUM between ctDNA and tissue UT Health AACR - - - - - Mays CASME Cam Detection of PTEN alterations was the most discordant between methods Samples (n) OPA PPA 0 50 100 150 200 250 300 350 400 Positive 21% ctDNA only Any 83.3 76.7 207 51% 30 42 63 17 (29 patients/ 21% PIK3CAIAKT1/PTEN alteration 43 alterations) 7% PIK3CA 88.9 77.1 155 16 33 46 16 AKT1 98.7 83.8 31 6 Positive 57% 12 PTEN 90.9 54.2 26 29 13 22 2 tissue only 4% (22 patients/ 23 alterations) 39% Positive by ctDNA Positive ctDNA only Positive ctDNA only and tissue (non-altered by tissue) by tissue) Large genomic Indel Homozygous SNV Positive tissue only Positive tissue only Tota patients with available rearrangement deletion (non-altered by ctDNA) (unknown by ctDNA) tissu NA results: N=558 Concordance calculated using tissue results as the reference, excluding and PPA calculated based on total number of patients with available Essue and/or ctDNA results (N=700). AKT1, AKT serine/threonine kinase; ctDNA, circulating tumor DNA: NGS, next-generation sequencing; OPA, overall percentage agreement; PIK3CA, phosphatidylinositol-4 5-bisphosphate 3-kinase catalytic subunit alpha; PPA percentage phosphatase and tensin homolog: SNV, single nucleotide variant. --- [Slide 3] SAN ANTONIO BREAST CANCER Summary of PFS by ctDNA alteration status SYMPOSIUM® UT Health AACR - - - - Hep Canner - Median PFS (months) Capivasertib Placebo n HR (95% CI) + fulvestrant + fulvestrant Overall CAPItello-291 population 708 7.2 3.6 0,60 (0.51-0.71) PIK3CA/AKT1/PTEN-altered by tissue 289 7.3 3.1 0.50 (0.38-0.65) All patients with a ctDNA result 658 7.2 3.5 0.59 (0.50-0.71) PIK3CAIAKT1IPTEN alteration detected in ctDNA 279 5.6 2.1 0.43 (0.33-0.56) ESR1m co-mutation 149 5.5 2.1 0.52 (0.36-0.76) No ESR1m detected 130 7.4 2.6 0.36 (0.23-0.54) PIK3CAIAKT1/PTEN alteration not detected in ctDNA 379 7.3 3.7 0.76 (0.60-0.95) PIK3CAIAKT1/PTEN alteration detected in either tissue or ctDNA 359 7.2 2.8 0.49 (0.38-0.62) PIK3CAIAKT1/PTEN alteration not detected (either both methods 335 7.2 3.7 0.74 (0.58-0.95) or with one unknown) 0.1 1.0 10.0 Favors capivasertib Hazard ratio Favors placebo plus fulvestrant (95% CI) plus fulvestrant Data cutoff: August 15 2022. AKT1, AKT serine/threonine kinase; CI, CO ctDNA, circulating turnor DNA; ESR1m, estrogen receptor gene mutation; HR, hazard ratio; PFS, progression-free survival; PIK3CA, phosphatidylinositol-4,5-bisphosphate 3-kinase cat / phosphatase and tensin homolog. --- [Slide 4] SAN ANTONIO BREAST CANCER Conclusions SYMPOSIUM® UT Health AACR - - - May - - ctDNA analysis offers a minimally invasive option to identify PIK3CAIAKT1/PTEN alterations in HR+ ABC, particularly for patients without suitable tumor tissue analysis PIK3CAIAKT1/PTEN alterations were detected by ctDNA only (non-altered or unknown by tissue) in ~10% of patients, and by tissue only in ~11% of patients Compared with tissue-based assessment of PTEN, more large genomic rearrangements but fewer homozygous deletions were detected by ctDNA Assessment of tumor fraction by methylation may improve the ability to identify patients with low ctDNA shedding, where ctDNA testing alone may miss alterations Clinical benefit (PFS) of capivasertib + fulvestrant in the ctDNA-altered group was consistent with the primary tissue-based analysis and irrespective of ESR1m ABC, advanced breast cancer; AKT1, AKT serine/threonine kinas DNA: ESR1m, estrogen receptor gene mutation; HR+, hormone receptor-positive; OPA, overall percentage agreement; PFS, progression-free survival; PIK3CA, phosphatidy kinase catalytic subunit alpha; PTEN, phosphatase and tensin homolog: TF, tumor fraction.

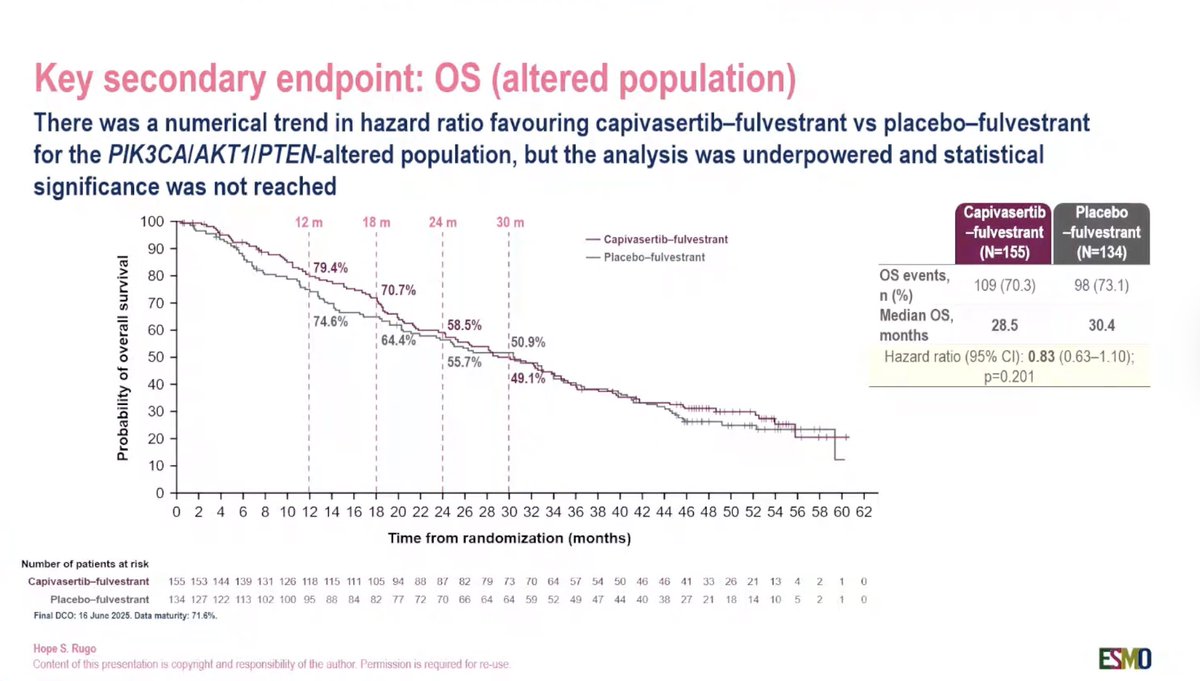

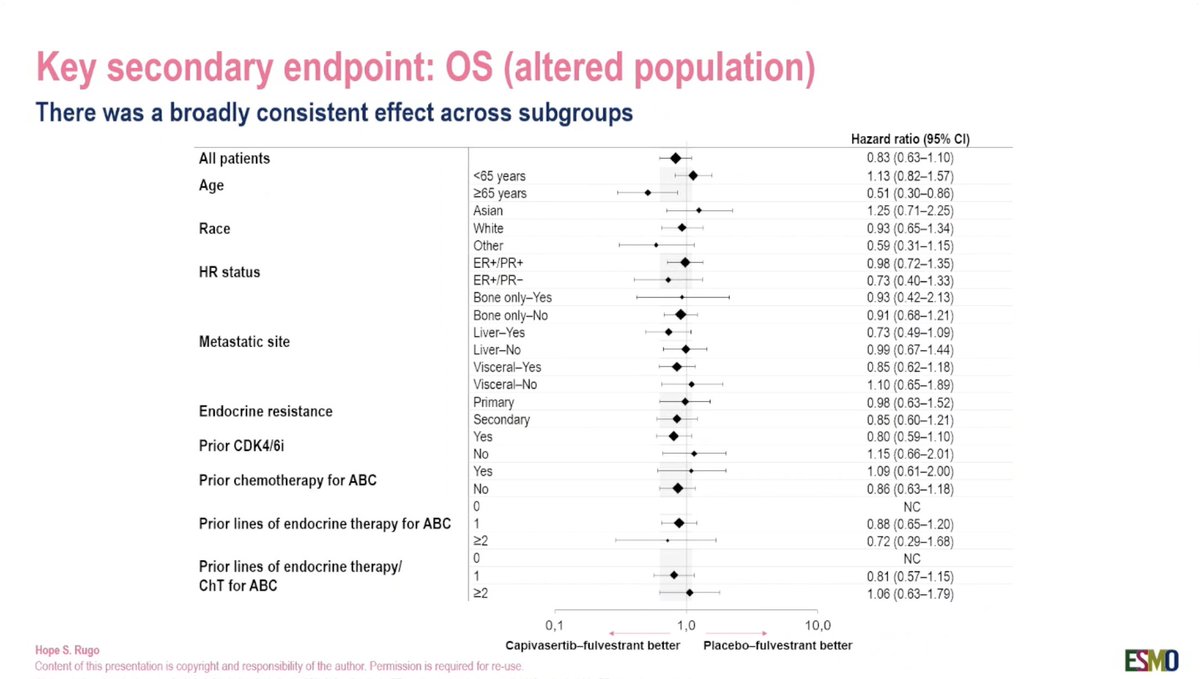
[Slide 1] 2026 ESMO BREAST CANCER Annual Congress Capivasertib and fulvestrant for patients with HR+/HER2- advanced breast cancer: Final overall survival results from the Phase 3 CAPItello-291 trial Hope S. Rugo,¹ Mafalda Oliveira,2 Sacha Howell,3 Florence Dalenc,⁴ Javier Cortes,⁵ Henry Gomez,⁶ Xichun Hu,⁷ Komal Jhaveri,8 Sibylle Loibl,9 Serafin Morales Murillo,10 Zbigniew Nowecki, 11 Meena Okera, 12 Yeon Hee Park, 13 Joo Hyuk-Sohn,14 Masakazu Toi, 15 Lyudmila Zhukova, 16 lan Wadsworth, 17 Marta Fulford, 18 Vijay Bhagawati Prasad,¹ 17 Nicholas C. Turner19 1 City of Hope Comprehensive Cancer Contor Duarte CA USA*; 2 Medical Oncology Department Vall d'Hebron University Hospital Barcelona Spain 3 The Christie NHS Foundation Trust, Manchester, UK, 4. Institut Universitaire du Cancer de Toulouse Oncopole Toulouse, France 5. 08 Madrid, Institute of Oncology. Madrid Spain, 6. Instituto Nacional de Enfermedades Neoplásicas, INEN, Departamento de Oncologia Médica, Lima, Peru 7. Shanghai Cancer Center Fudan University, Shanghai China, 8 Memorial Sloan Kettering Cancer Center New York NY, USA: 9. GBG Forschungs GmbH Neu-Isenburg Germany 10. Institut de Recerca Biomédica Barcelona, Spain: 11 The Mana Sklodowska Curie Memorial Cancer Center and Institute of Oncology. Warsaw Poland 12 ICON Cancer Centre. Adelaide Australia 13 Sungkyunkwan University School of Medicine Samsung Medical Center, Seoul, Republic of Korea, 14. Yonsei University College of Medicine Yonsei Cancer Center Seoul Republic of Korea 15. Kyoto University Hospital Kyoto, Japan; 16. Loginov Moscow Clinical Scentic Center, Moscow, Russia 17. Oncology R&D. AstraZeneca, Cambridge UK 18 Oncology R&D. AstraZeneca Warsaw Poland 19 Royal Marsden Hospital Institute of Cancer Research London, UK Affiliation at the time of study Division of Hematology and Oncology, University of California San Francisco Helen Diller Family Comprehensive Cancer Center San Francisco, CA USA Hope S. Rugo Content of this presentation is copyright and responsibility of the author Permission is required for re-use ESMO --- [Slide 2] Key secondary endpoint: OS (altered population) There was a numerical trend in hazard ratio favouring capivasertib-fulvestrant vs placebo-fulvestrant for the PIK3CA/AKT1/PTEN-altered population, but the analysis was underpowered and statistical significance was not reached Capivasertib Placebo 100 12 m 18 m 24 m 30 m -fulvestrant -fulvestrant — Capivasertib-fulvestrant 90 — Placebo-fulvestrant (N=155) (N=134) 79.4% 80 OS events, 70.7% 109 (70.3) 98 (73.1) Probability of overall survival 70 n (%) 74.6% Median OS, 60 58.5% 28.5 30.4 64.4% 50.9% months 50 55.7% Hazard ratio (95% CI): 0.83 (0.63-1.10); 40 49.1% p=0.201 30 20 10 0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 54 56 58 60 62 Time from randomization (months) Number of patients at risk Capivasertib-fulvestrant 155 153 144 139 131 126 118 115 111 105 94 88 87 82 79 73 70 64 57 54 50 46 46 41 33 26 21 13 4 2 1 0 Placebo-fulvestrant 134 127 122 113 102 100 95 88 84 82 77 72 70 66 64 64 59 52 49 47 44 40 38 27 21 18 14 10 5 2 1 0 Final DCO: 16 June 2025. Data maturity: 71.6% Hope S. Rugo Content of this presentation is copynght and responsibility of the author Permission is required for re-use ESMO --- [Slide 3] Subsequent treatments (altered population) In the PIK3CA/AKT1/PTEN-altered population, multiple subsequent treatment lines and imbalances in the use of targeted therapies may have contributed to the reduced treatment effect beyond PFS PIK3CA/AKT1/PTEN-altered population PIK3CA/AKT1/PTEN-altered population Total Number of lines, Capivasertib-fulvestrant Placebo-fulvestrant Cytotoxic Capecitabine n (%) (N=155) (N=134) chemotherapy Paclitaxel 1 32 (20.6) 31 (23.9) Total Fulvestrant 2 28 (18.1) 26 (19.4) Capivasertib-fulvestrant Hormone Exemestane Placebo-fulvestrant 3 34 (21.9) 20 (14.9) therapy Anastrozole Letrozole >3 33 (21.3) 38 (28.4) Tamoxifen Total Targeted CDK4/6i Treatment type, Capivasertib-fulvestrant Placebo-fulvestrant therapy Everolimus n (%) (N=155) (N=134) Alpelisib Any 127 (81.9) 115 (85.8) Anti-angiogenic therapy Cytotoxic ChT 117 (75.5) 100 (74.6) Experimental therapy Hormone therapy 59 (38.1) 63 (47.0) Biologic therapy PARP inhibitor Targeted therapy 40 (25.8) 57 (42.5) Other 0 20 40 60 80 100 Patients, % ChT, chemotherapy PARP, poly-ADP ribose polymerase Hope S. Rugo In the CDK4/6i naive population (n=81), 43.9% of patients in the capivasertib arm Content of this presentation is copyright and responsibility of the author. Permission is required for re-use versus 62.5% in the placebo arm received a CDK4/6i post-progression ESMO --- [Slide 4] Key secondary endpoint: OS (altered population) There was a broadly consistent effect across subgroups Hazard ratio (95% CI) All patients 0.83 (0.63-1.10) <65 years 1.13 (0.82-1.57) Age >65 years 0.51 (0.30-0.86) Asian 1.25 (0.71-2.25) Race White 0.93 (0.65-1.34) Other 0.59 (0.31-1.15) ER+/PR+ HR status 0.98 (0.72-1.35) ER+/PR- 0.73 (0.40-1.33) Bone only-Yes 0.93 (0.42-2.13) Bone only-No 0.91 (0.68-1.21) Liver-Yes 0.73 (0.49-1.09) Metastatic site Liver-No 0.99 (0.67-1.44) Visceral-Yes 0.85 (0.62-1.18) Visceral-No 1.10 (0.65-1.89) Endocrine resistance Primary 0.98 (0.63-1.52) Secondary 0.85 (0.60-1.21) Yes Prior CDK4/6i 0.80 (0.59-1.10) No 1.15 (0.66-2.01) Yes 1.09 (0.61-2.00) Prior chemotherapy for ABC No 0.86 (0.63-1.18) 0 NC Prior lines of endocrine therapy for ABC 1 0.88 (0.65-1.20) >2 0.72 (0.29-1.68) 0 NC Prior lines of endocrine therapy/ 1 ChT for ABC 0.81 (0.57-1.15) >2 1.06 (0.63-1.79) 0,1 1,0 10,0 Hope S. Rugo Capivasertib-fulvestrant better Placebo-fulvestrant better Content of this presentation is copyright and responsibility of the author. Permission is required for re-use ESMO


[Slide 1] CAPItello-291 study design Phase 3, randomised, double-blind, placebo-controlled study (NCT04305496) Patients with 400 mg twice daily, Dual primary endpoints HR-positive/HER2-negative* ABC Capivasertib 4 days on, 3 days off PFS by investigator assessment in: Primary DCO PIK3CA/AKT1/PTEN-allered Men and pre-/post-menopausal women Overall population Recurrence or progression while on. Fulvestrant 500 mg: Cycle 1, Days 1 & or <12 months from end of, adjuvant Al, 15; then every 4 weeks Key secondary endpoint or progression while on prior Al for ABC OS <2 lines of prior endocrine therapy for ABC Stratification factors: S1 line of chemotherapy for ABC R1:1 iver metastases (yes/no) (N=708) Prior CDK4/61 (yes/no) Secondary endpoints Prior CDK4/6i allowed (at least 51% required) Region PFS2 Final DCO Safety No prior SERD mTOR inhibitor, PI3K inhibitor, or AKT inhibitor Placebo Twice daily, 4 days on, 3 days off Exploratory endpoints HbA1c <8.0% (63 mmol/mol) and TTFSC diabetes not requiring insulin allowed FFPE tumour sample from the Fulvestrant 500 mg: Cycle 1, Days 1 & OS in patients who had received prior 15; then every 4 weeks CDK4/6 primary/recurrent cancer available for retrospective central molecular testing All listed endpoints assessed in: PIK3CA/AKT1/PTEN-altered Overall population Pm. or - - inkning - agreed - to details of - chady involved seas regative - that 11 Tage 1. United Stake Asshm Campan Audress and know Region I - scope and Thanks - Region 1 Ass V. 000 data - of FIFE ford permits entedided HE ISLL - and MICR rechies: trans on - assistal ITS progression the NEW FFDZ. the from unit second programs . that the " any - K. NEW schedule costrogon monter together TIPSC time to vst subsequent therethoropy Hope & Ruge Content of this presentation is copyright and responsibility of the author Permission n required for re-ute ESMD ESMO BREAST CANCER --- [Slide 2] Key secondary endpoint: OS (altered population) There was a numerical trend in hazard ratio favouring capivasertib-fulvestrant vs placebo-fulvestrant for the PIK3CA/AKT1/PTEN-altered population, but the analysis was underpowered and statistical significance was not reached Capivasertib Placebo 100 12m 18m 24 m 30m Capivasertib-fulvestrant -fulvestrant -fulvestrant 90 Placebo-fulvestrant (N=155) (N=134) 80 79.4% OS events, 70.7% n (%) 109 (70.3) 98(73.1) Probability of overall survival 70 74.6% 60 58.5% Median OS, 28.5 30.4 64.4% 50.9% months 50 55.7% Hazard ratio (95% CI): 0.83 (0.63-1.10): 40 49.1% p=0.201 30 20 10 0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 54 56 58 60 62 Time from randomization (months) Number of patients at risk Capivasertitb-fulvestrant 155 150 144 139 131 120 110 115 111 105 94 00 07 02 79 is to 64 57 54 50 40 40 41 33 20 21 13 4 2 1 Placebo-fulvestrant 134 127 122 113 102 100 05 na M R2 77 72 70 66 64 G4 50 52 40 47 44 40 " 77 21 in 14 to 5 7 1 n Final DCO: 16 June 2025 Date maturity: 71. % Hope 5. Ruge Content of this presentation is applytight and responsibility of the milher Permission in required lot re-use MD ESMO BREAST CANCER --- [Slide 3] Secondary endpoint: PFS2 Capivasertib-fulvestrant continued to demonstrate lasting treatment benefit retained through progression on next-line treatment*, which was numerically improved in both the altered and overall populations PIK3CA/AKT1/PTEN-altered population Overall population Capivasertib- Placebo- Capivasertib- Placebo- fulvestrant fulvestrant fulvestrant fulvestrant 100 (N=155) (N=134) 100 (N=355) (N=353) 90 50 PFS2 events, n 134 118 PFS2 events, n 306 303 00 a Median PFS2, Median PFS2, re 15.9 11.1 70 15.4 12.7 months months Probability of PF32 60 Hazard ratio (95% CI): 0.68(0.53-0.88) Probability of PFS2 no Hazard ratio (95% CI) 0.85 (0.72-1.00) 50 50 40 3 30 30 20 20 10 Capivasertib-fulvestrant 10 Capivasertib-fulvestrant Placebo-fulvestrant Placebo-fulvestrant 0 0 0 2 I 0 10 12 14 22 24 26 28 30 R 34 36 30 2 42 48 50 52 54 56 50 8 0 2 4 10 12 22 24 or 32 34 36 30 40 42 44 48 52 54 5068 60 8 Time from randomization (months) Time from randomization (months) Number of publicate Number patients Placeto I .. Placetso falvestrate *PF82 - defined - the length if time from to second progressive on most - treatment an the earliest of other Smith of progression event following bestment start after Int progressions Hope S Ruge Content of the presentation is copyright and responsibility of the author Permison is required for re-use ESMO 8 ESMO BREAST CANCER --- [Slide 4] Summary & conclusions Capivasertib-fulvestrant achieved statistically significant, clinically meaningful PFS benefits in both the overall and PIK3CA/AKT1/PTEN-altered HR-positive/HER2-negative populations The OS hazard ratio (0.83) indicated a numerical trend in favour of capivasertib-fulvestrant in the PIK3CA/AKT1/PTEN-altered population, but did not reach statistical significance As a key secondary endpoint with 53% power, the study was considered underpowered to potentially detect a benefit in OS for the PIK3CA/AKT1/PTEN-altered population Extensive post-progression therapy likely confounded OS, with a high burden of subsequent treatment lines and greater use of targeted therapies in the placebo-fulvestrant arm versus the capivasertib-fulvestrant arm, potentially diluting the treatment effect Per study design, OS was not formally tested in the overall population, where no numerical difference in risk of death was observed (hazard ratio: 1.00) At final analysis, the combination showed sustained, meaningful benefit beyond PFS, evidenced by improvements in PFS2 (hazard ratio: 0.68, altered) and delayed TTFSC (hazard ratio: 0.62, altered) across both the PIK3CA/AKT1/PTEN-altered and overall populations Clinically relevant subgroup signal: In PIK3CA/AKT1/PTEN-altered. patients with prior CDK4/6 inhibitor therapy, the OS hazard ratio was 0.78 Safety remained consistent and manageable with no new safety signals Capivasertib-fulvestrant provides lasting treatment benefit versus placebo-fulvestrant, with manageable safety; OS interpretation is limited by study power and post-progression treatment confounding Hope $ Rugo Content of this presentation a copyright and responsibility of the author Permission a request for more ESMO 8 ESMO BREAST CANCER

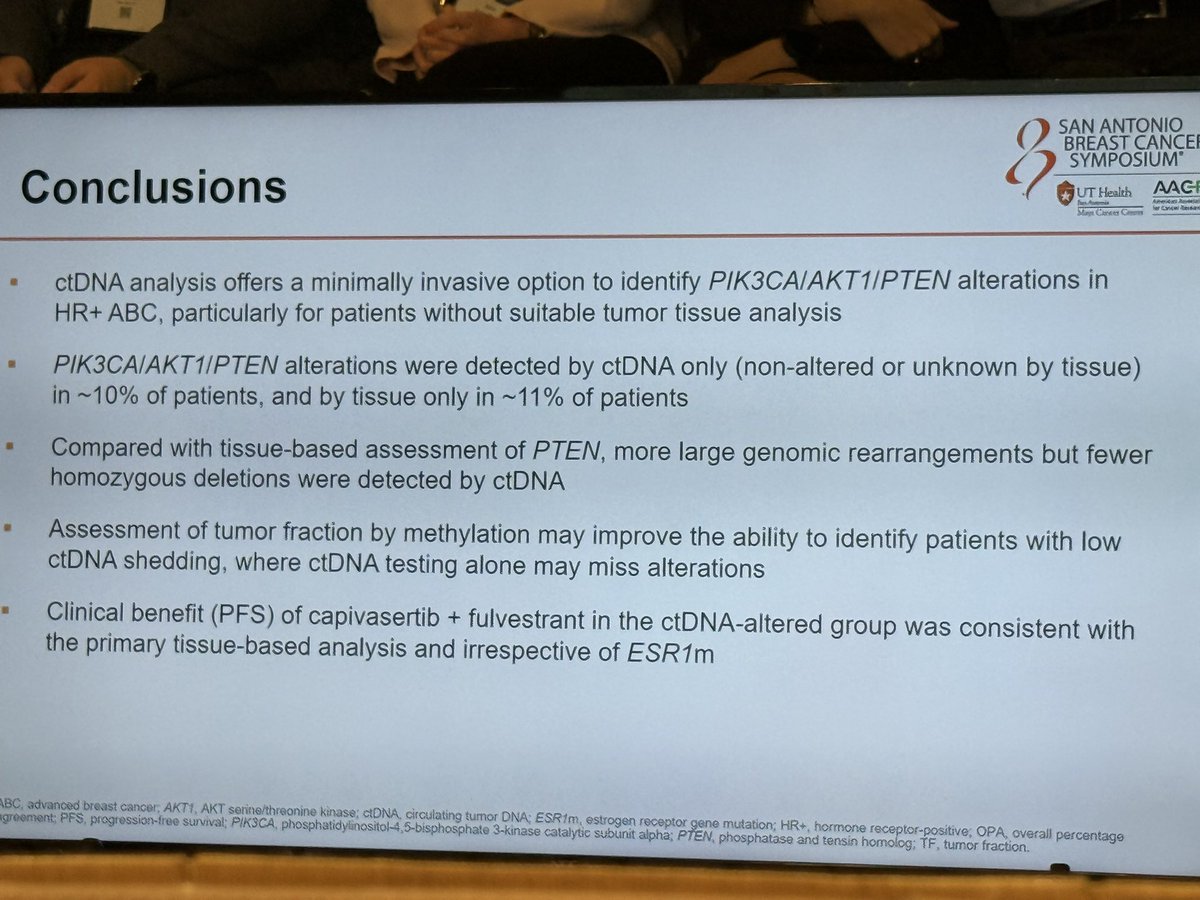
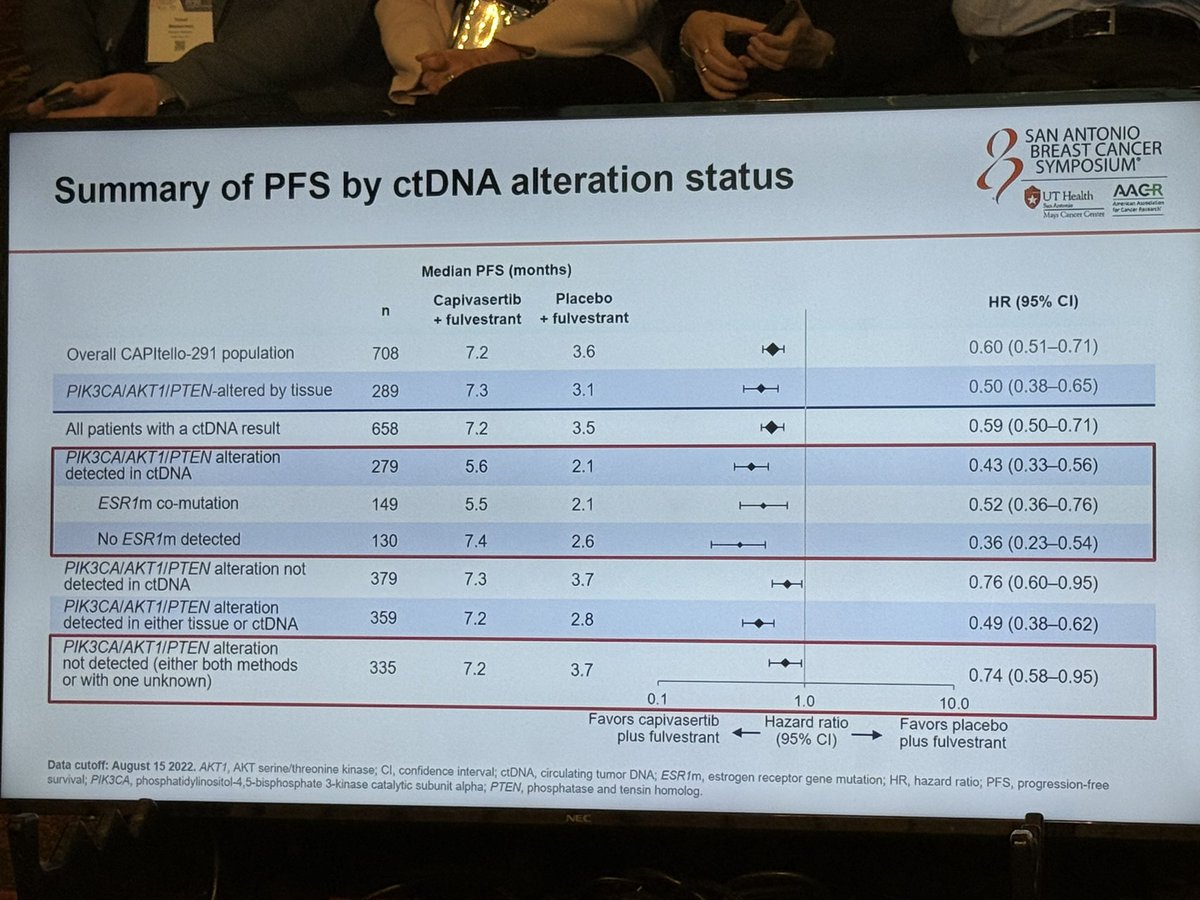
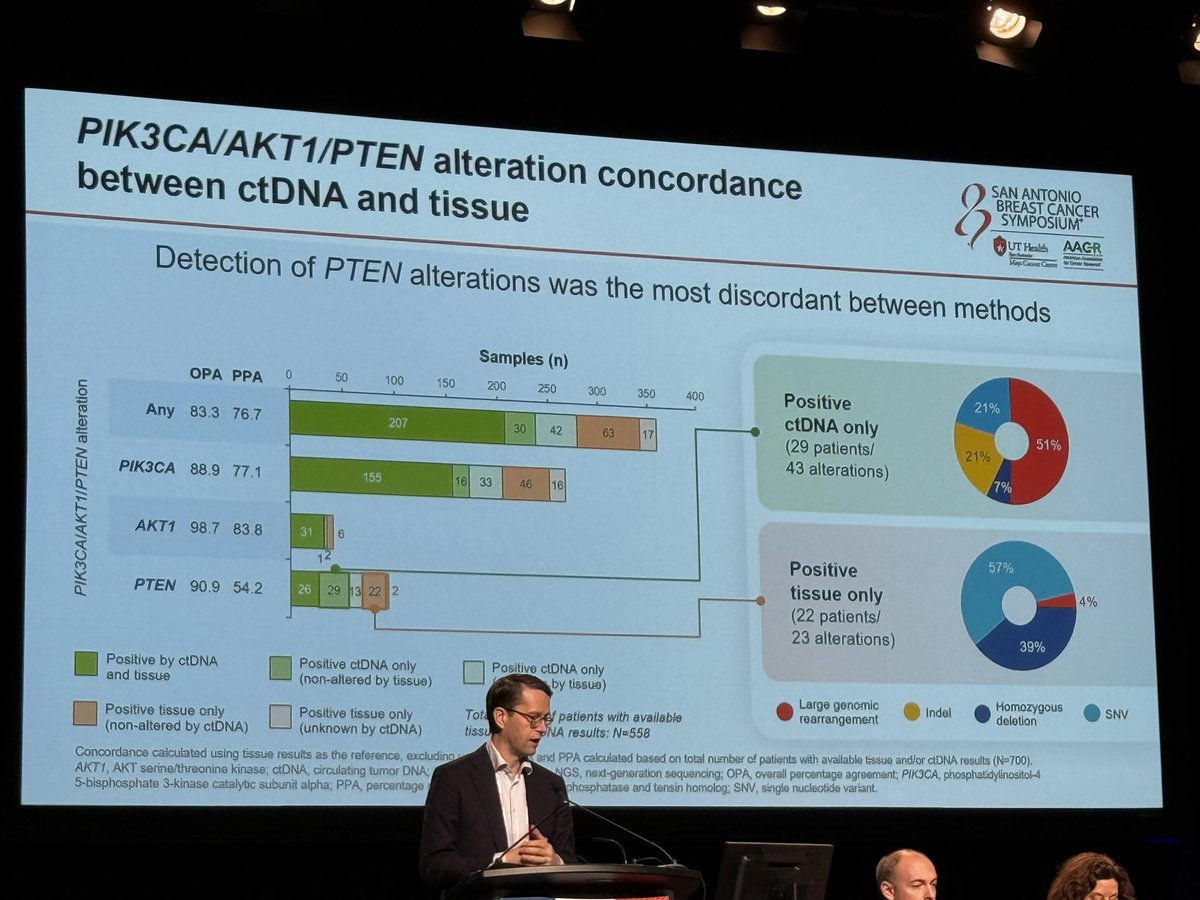
[Slide 1] PIK3CA/AKT1/PTEN alteration concordance SAN ANTONIO BREAST CANCER SYMPOSIUM® between ctDNA and tissue UT Health AACR American Appeacan Cancer Research Mays Cancer Center Comparison of tissue and ctDNA detected ctDNA methylation tumor fraction p<0.0001 Samples (n) 100 OPA PPA 0 50 100 150 200 250 300 350 400 10 1 Any 83.3 76.7 207 30 42 63 17 PIK3CAIAKT1IPTEN alteration ctDNA TF (%, log scale) 111 0.1 ÷ 0.01 PIK3CA/AKT1/PTEN alterations Not detected Non shedders were detected by ctDNA alone in 72/700 patients (10.3%) Positive by ctDNA Positive tissue only and tissue (non-altered by (n=207) ctDNA, n=63) Number of patients by TF %, n (%) Positive by ctDNA Positive ctDNA only Positive ctDNA only N 0 >0-0.1 >0.1-1 >1-10 >10 and tissue (non-altered by tissue) (unknown by tissue) ctDNA+/Tissue+ 207 0 (0) 3 (1) 38 (18) 81 (39) 85 (41) Positive tissue only Positive tissue only Total number of patients with available ctDNA-/Tissue+ 63 18 (29) 13 (21) 14 (22) 11 (17) 7 (11) (non-altered by ctDNA) (unknown by ctDNA) tissue and ctDNA results: N=558 Concordance calculated using tissue results as the reference, excluding unknown; OPA and PPA calculated based on total number of patients with available tissue and/or ctDNA results (N=700). AKT1, AKT serine/threonine kinase; ctDNA, circulating tumor DNA; OPA, overall percentage agreement; PIK3CA, phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha; PPA, percentage positive agreement; PTEN, phosphatase and tensin homolog: TF, tumor fraction. --- [Slide 2] SAN ANTONIO BREAST CANCE SYMPOSIUM® Conclusions UT Health AAG - - - Lancel ter Mays Classes Crems ctDNA analysis offers a minimally invasive option to identify PIK3CAIAKT1/PTEN alterations in HR+ ABC, particularly for patients without suitable tumor tissue analysis PIK3CAIAKT1/PTEN alterations were detected by ctDNA only (non-altered or unknown by tissue) in ~10% of patients, and by tissue only in ~11% of patients Compared with tissue-based assessment of PTEN, more large genomic rearrangements but fewer homozygous deletions were detected by ctDNA Assessment of tumor fraction by methylation may improve the ability to identify patients with low ctDNA shedding, where ctDNA testing alone may miss alterations Clinical benefit (PFS) of capivasertib + fulvestrant in the ctDNA-altered group was consistent with the primary tissue-based analysis and irrespective of ESR1m BC, advanced breast cancer, AKT1, AKT senne/threonine kinase; ctDNA circulating tumor DNA; ESR1m, estrogen receptor gene mutation; HR+, hormone receptor-positive; OPA, overall percentage greement; PFS, progression-free survival; PIKSCA, phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha; PTEN, phosphatase and tensin homolog; TF, tumor fraction. --- [Slide 3] SAN ANTONIO BREAST CANCER Summary of PFS by ctDNA alteration status SYMPOSIUM® UT Health AACR Service Aperican Ausorian for Lence Mays Cancer Center Median PFS (months) Capivasertib Placebo n HR (95% CI) + fulvestrant + fulvestrant Overall CAPItello-291 population 708 7.2 3.6 0.60 (0.51-0.71) PIK3CA/AKT1/PTEN-altered by tissue 289 7.3 3.1 0.50 (0.38-0.65) All patients with a ctDNA result 658 7.2 3.5 H 0.59 (0.50-0.71) PIK3CAIAKT1/PTEN alteration detected in ctDNA 279 5.6 2.1 0.43 (0.33-0.56) ESR1m co-mutation 149 5.5 2.1 0.52 (0.36-0.76) No ESR1 1m detected 130 7.4 2.6 0.36 (0.23-0.54) PIK3CAIAKT1/PTEN alteration not detected in ctDNA 379 7.3 3.7 0.76 (0.60-0.95) PIK3CAIAKT1/PTEN alteration detected in either tissue or ctDNA 359 7.2 2.8 0.49 (0.38-0.62) PIK3CAIAKT1/PTEN alteration not detected (either both methods 335 7.2 3.7 0.74 (0.58-0.95) or with one unknown) 0.1 1.0 10.0 Favors capivasertib Hazard ratio Favors placebo plus fulvestrant (95% CI) plus fulvestrant Data cutoff: August 15 2022. AKT1, AKT serine/threonine kinase; CI, confidence interval; ctDNA, circulating tumor DNA; ESR fm, estrogen receptor gene mutation; HR, hazard ratio; PFS, progression-free survival; PIK3CA, phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha; PTEN, phosphatase and tensin homolog. --- [Slide 4] PIK3CA/AKT1/PTEN alteration concordance SAN ANTONIO BREAST CANCER SYMPOSIUM between ctDNA and tissue UT Health AACR Sex Antonio American for Cancer Research Mays Cancer Center Detection of PTEN alterations was the most discordant between methods Samples (n) OPA PPA 0 50 100 150 200 250 300 350 400 Positive 21% ctDNA only Any 83.3 76.7 207 30 42 63 51% 17 (29 patients/ 21% PIK3CAIAKT1/PTEN alteration 43 alterations) 7% PIK3CA 88.9 77.1 155 16 33 46 16 AKT1 98.7 83.8 31 6 12 Positive 57% PTEN 90.9 54.2 26 29 13 22 2 tissue only 4% (22 patients/ 23 alterations) 39% Positive by ctDNA Positive ctDNA only Positive ctDNA only and tissue (non-altered by tissue) (unknown by tissue) Large genomic Indel Homozygous Positive tissue only Positive tissue only Total number of patients with available SNV rearrangement deletion (non-altered by ctDNA) (unknown by ctDNA) tissue and ctDNA results: N=558 Concordance calculated using tissue results as the reference, excluding unknown; OPA and PPA calculated based on total number of patients with available tissue and/or ctDNA results (N=700). AKT1, AKT serine/threonine kinase; ctDNA, circulating tumor DNA; indel, Insertion/deletion; NGS, next-generation sequencing; OPA, overall percentage agreement; PIK3CA, phosphatidylinositol-4 5-bisphosphate 3-kinase catalytic subunit alpha; PPA, percentage positive agreement; PTEN, phosphatase and tensin homolog; SNV, single nucleotide variant.


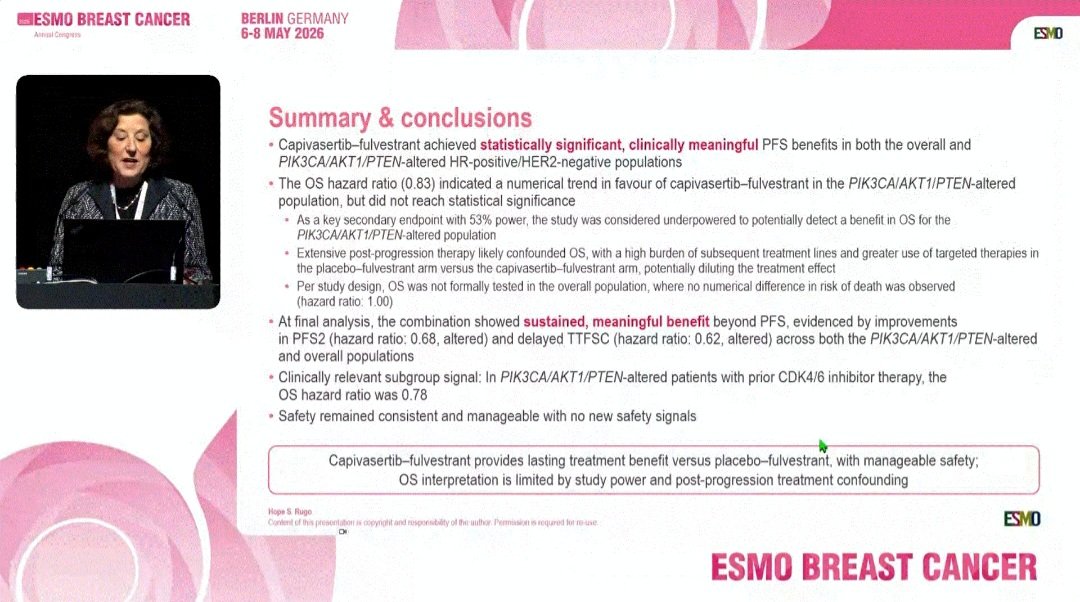
[Slide 1] ESMO BREAST CANCER BERLIN GERMANY Amail Corgress 6-8 MAY 2026 ESMO CAPItello-291 study design Phase 3, randomised, double-blind, placebo-controlled study (NCT04305496) Patients with HR-positive/HER2-negative* ABC Capivasertib 400 mg twice daily, Dual primary endpoints 4 days on, 3 days off PFS by investigator assessment in: Primary DCO PIK3CA/AKT1/PTEN-altered Men and pre-/post-menopausal women Overall population Recurrence or progression while on, Fulvestrant 500 mg: Cycle 1, Days 1& or <12 months from end of, adjuvant AI, 15; then every 4 weeks Key secondary endpoint or progression while on prior AI for ABC OS 52 lines of prior endocrine therapy for ABC Stratification factors: S1 line of chemotherapy for ABC R1:1 iver metastases (yes/no) (N=708) Prior CDK4/6i (yes/no) Secondary endpoints Prior CDK4/6i allowed (at least 51% required) Region PFS2 Final DCO Safety No prior SERD mTOR inhibitor, PI3K inhibitor, or AKT inhibitor Placebo Twice daily, 4 days on, 3 days off Exploratory endpoints HbA1c <B 0% (63. mmol/mol) and TTFSC diabetes not requiring insulin allowed FFPE tumour sample from the Fulvestrant 500 mg: Cycle 1, Days 1 & OS in patients who had received prior primary/recurrent cancer available for 15; then every 4 weeks CDK4/6i retrospective central molecular testing All listed endpoints assessed in: PIK3CA/AKT1/PTEN-altered Overall population - or - unine - agence - his design of the date instruct MERS regative *** I " 11 or FUSH- Rajin United States Westom Temper Audress and nat Region 2 America petern unge and Formsts Region Asia A/ their 000 sea FFFE formale food persion entedded HC IS ni rechares: larget CO. overall survival FTS. progremen the survive IT 37. time from rundomision unit second program " dout the to any - R. NERD TIPSC the to VII subsiquent chemotheropy Hope Rugo Content of this presentation is copyright and responsibility of the subser Permission n required for re-uin ESMO ESMO BREAST CANCER --- [Slide 2] ESMO BREAST CANCER BERLIN GERMANY Annual Corgress 6-8 MAY 2026 ESMO Key secondary endpoint: OS (altered population) There was a numerical trend in hazard ratio favouring capivasertib-fulvestrant vs placebo-fulvestrant for the PIK3CA/AKT1/PTEN-altered population, but the analysis was underpowered and statistical significance was not reached Capivasertib Placebo 100 12m m 18 m 24 m 30m -fulvestrant -fulvestrant Capivasertib-fulvestrant 90 Placebo-fulvestrant (N=155) (N=134) 79.4% 80 OS events, 70.7% 70 (%) 109 (70.3) 98 (73.1) Probability of overall survival 74.6% Median OS, 60 58.5% 28.5 30.4 64.4% (50.9% months 50 55.7% Hazard ratio (95% CI): 0.83 (0.63-1.10); 40 49.1% p=0.201 30 20 10 0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 54 56 58 60 62 Time from randomization (months) Number of patients at risk Capivasertib-fulvestrant 155 150 144 139 131 120 116 115 111 105 94 00 07 02 (9) 73 ru 04 57 54 50 40 40 41 33 20 21 13 4 2 1 0 Placebo-fulvestrant 134 127 122 113 102 100 as AR A4 32 77 72 70 66 64 64 50 52 40 47 44 40 n 27 21 18 14 to 6 2 1 0 Final DCO: 16 June 2025 Date milurity: 71. 6% Hope Rugo Content of this presentation is copyright and responsibility of the withor Permission 8 required for re-use ESMO ESMO BREAST CANCER --- [Slide 3] ESMO BREAST CANCER BERLIN GERMANY Annual Congress 6-8 MAY 2026 ESMO Secondary endpoint: PFS2 Capivasertib-fulvestrant continued to demonstrate lasting treatment benefit retained through progression on next-line treatment*, which was numerically improved in both the altered and overall populations PIK3CA/AKT1/PTEN-altered population Overall population Capivasertib- Placebo- Capivasertib- Placebo- fulvestrant fulvestrant fulvestrant fulvestrant 100 100 (N=155) (N=134) (N=355) (N=353) 90 50 PFS2 events, n 134 118 PFS2 events, n 306 303 as 83 Median PFS2, Median PFS2, 70 15.9 11.1 70 15.4 12.7 months months Probability of PF32 60 Probability of PFS2 60 Hazard ratio (95% Cl): 0. 68 (0.53-0.88) Hazard ratio (95% CI): 0.85 (0.72-1.00) 50 50 40 10 30 30 20 20 10 Capivasertib-fulvestrant 10 Capivasertib-fulvestrant Placebo- fulvestrant Placebo-fulvestrant 0 0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 R 34 35 38 60 42 44 46 48 50 52 54 56 58 60 62 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 54 56658 60 62 Time from randomization (months) Time from randomization (months) I I I Number patients at mk Capital - 551 142 ⑉ 129 100 12 73 29 6 - deleastment IM MI us 204 264 100 161 34 907 - is 77 - 3 53 " - 24 19 " 11 0 Placetion 134 " is " - 11 " 47 " " 14 31 17 24 13 13 13 13 = Placebo falvostrant 350 177 " 11 73 00 50 11 40 " " 00 0 * 25 19 17 0. - PI PF52 was Inflace - the longth of time from rendomization second progression on and - bottment se the earlod of signer Seath progression a following about treatment start shor first progression Hope S. Rugo Content of this presentation is copyright and responsibility of the author Permission 8 required for re-use ESMO 5 ESMO BREAST CANCER --- [Slide 4] ESMO BREAST CANCER BERLIN GERMANY Assist Congress 6-8 MAY 2026 ESMD Summary & conclusions Capivasertib-fulvestrant achieved statistically significant, clinically meaningful PFS benefits in both the overall and PIK3CA/AKT1/PTEN-altered HR-positive/HER2-negative populations The OS hazard ratio (0.83) indicated a numerical trend in favour of capivasertib-fulvestrant in the PIK3CA/AKT1/PTEN-altered population, but did not reach statistical significance As a key secondary endpoint with 53% power, the study was considered underpowered to potentially detect a benefit in OS for the PIK3CA/AKT1/PTEN-altered population Extensive post-progression therapy likely confounded OS, with a high burden of subsequent treatment lines and greater use of targeted therapies in the placebo-fulvestrant arm versus the capivasertib-fulvestrant arm, potentially diluting the treatment effect Per study design, OS was not formally tested in the overall population, where no numerical difference in risk of death was observed (hazard ratio: 1.00) At final analysis, the combination showed sustained, meaningful benefit beyond PFS, evidenced by improvements in PFS2 (hazard ratio: 0.68, altered) and delayed TTFSC (hazard ratio: 0.62, altered) across both the PIK3CA/AKT1/PTEN-altered and overall populations Clinically relevant subgroup signal: In PIK3CA/AKT1/PTEN-altered patients with prior CDK4/6 inhibitor therapy, the OS hazard ratio was 0.78 Safety remained consistent and manageable with no new safety signals Capivasertib-fulvestrant provides lasting treatment benefit versus placebo-fulvestrant, with manageable safety; OS interpretation is limited by study power and post-progression treatment confounding Hope Rugo Content of this presentation . copyngent and responsibility of the author Permission is required for re-use ESMO o ESMO BREAST CANCER

Highest-engagement tweets about this trial, ranked by KOL discussant count (replies + quote-tweets). Replies in green, quote-tweets in blue. Wall Street, stock-promo, and non-substantive replies excluded.
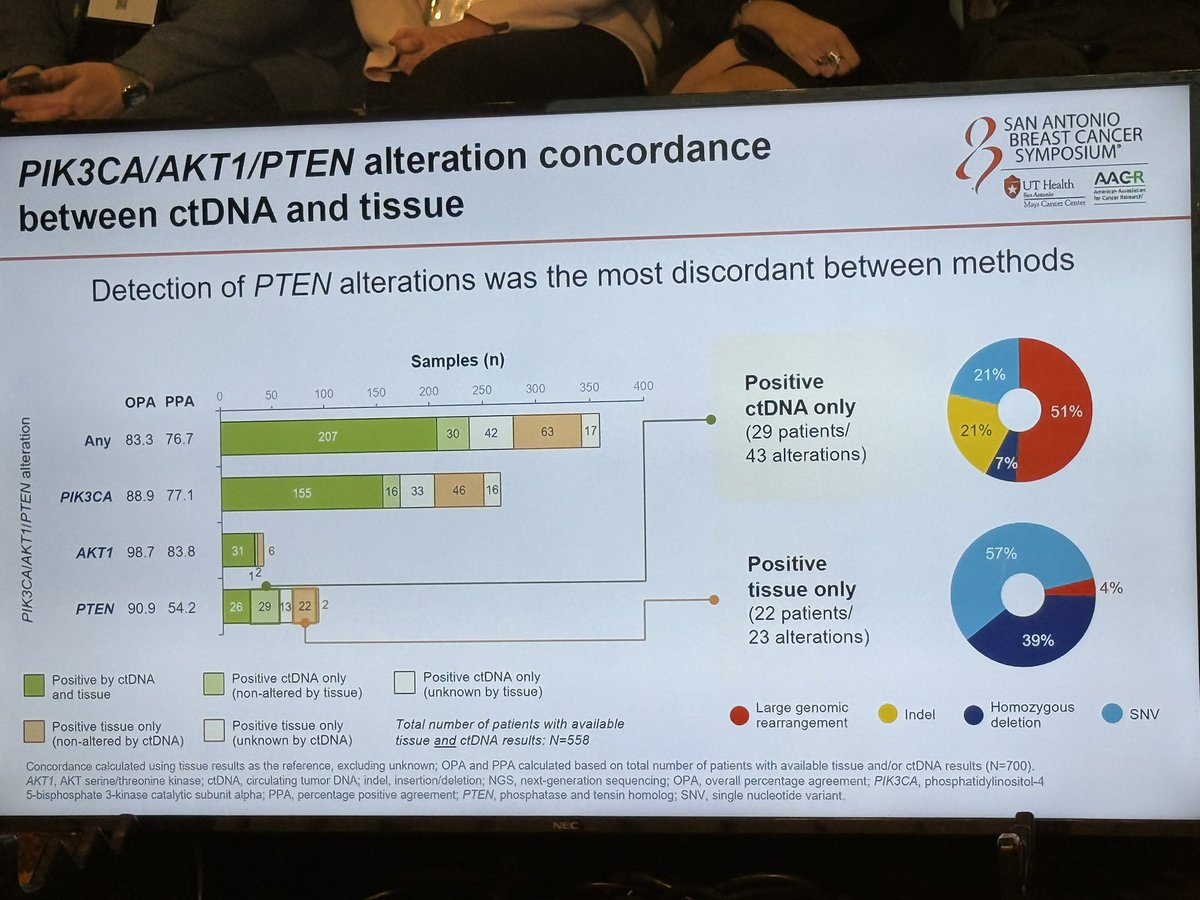
Interesting ctDNA sub-analysis from CAPItello291. Most PIK3CA/AKT/PTEN alterations are found both on tissue and ctDNA, but about 10% are found only on one of the two methods. PTEN alterations the most discordant. #SABCS25 https://t.co/DhqxbknPdh






 +4
+4
🔥 Does capivasertib actually improve survival? CAPItello-291 final OS just answered this 👇 Trial: Capivasertib + fulvestrant vs placebo + fulvestrant Setting: HR+/HER2- ABC post-AI 👥 Study population 708 pts Biomarker cohort: PI3K/AKT/PTEN altered 💊 Arms Capivasertib + https:
#SABCS2025 Nick Turner presents our capi291 ctDNA data. Benefit seen in those without ESR1m and large genomic rearrangements more frequently found in ctDNA vs tissue. Nice data supporting this combination, and supports both tissue and ctDNA evals. @OncoAlert https://t.co/UjMNGd2Y
#ESMOBreast26 CAPItello-291 final analysis PFS benefit is clear; PFS2 also supports sustained disease control. No OS benefit was shown. ➡️ Prior CDK4/6i-altered subgroup: interesting, but exploratory. OS remains unproven and confounded by post-progression therapies. https://t
📌 Capivasertib and fulvestrant for patients with HR+/HER2- advanced breast cancer: Final overall survival ✨results from the phase III CAPItello-291 trial ✨Proffered Paper Session 2 @hoperugo #ESMOBreast26 @OncoAlert #OncoAlertAF https://t.co/shAj2lZNV5
#ESMOBreast26 CAPItello-291 final OS: Capivasertib + fulvestrant continued to show durable benefit in PIK3CA/AKT1/PTEN-altered HR+/HER2− ABC, with meaningful PFS2 improvement and ~7-month OS gain after prior CDK4/6i. Manageable safety profile maintained. #BreastCancer https://t
CAPItello-291 is a global Phase III double-blind, placebo-controlled trial that established capivasertib (Truqap) + fulvestrant as a treatment option for HR+/HER2- advanced breast cancer progressing on aromatase inhibitor therapy, particularly in patients with PIK3CA/AKT1/PTEN-altered tumours. The final OS analysis presented at ESMO Breast 2026 added important nuance: the regimen did NOT improve overall survival in either the altered or overall population, but PFS2 and time-to-chemotherapy data continue to support sustained disease control. Capivasertib + fulvestrant received FDA approval Nov 2023 and NICE approval May 2025 for the PIK3CA/AKT1/PTEN-altered cohort.
FDA approved capivasertib (Truqap) + fulvestrant Nov 2023 for adults with HR+, HER2-negative locally advanced or metastatic breast cancer with one or more PIK3CA/AKT1/PTEN alterations following progression on at least one endocrine-based regimen. Approval based on the PIK3CA/AKT1/PTEN-altered cohort of CAPItello-291 (HR 0.50 vs 0.79 in non-altered).
Approval date: November 2023
Population: Adults with HR+/HER2- locally advanced or metastatic breast cancer who relapsed/progressed during or after AI treatment, with or without prior CDK4/6i. Any menopausal status; men eligible. ~40% PIK3CA/AKT1/PTEN-altered.
Interventions: Capivasertib 400 mg PO BID 4 days on / 3 days off + fulvestrant 500 mg IM Q4W (with C1D1 and C1D15 loading doses). Control: matching placebo + fulvestrant.
Endpoints: Dual primary: investigator-PFS overall and altered. Secondary: OS, PFS2, time to first subsequent chemotherapy, ORR, safety, PROs (HRQoL).
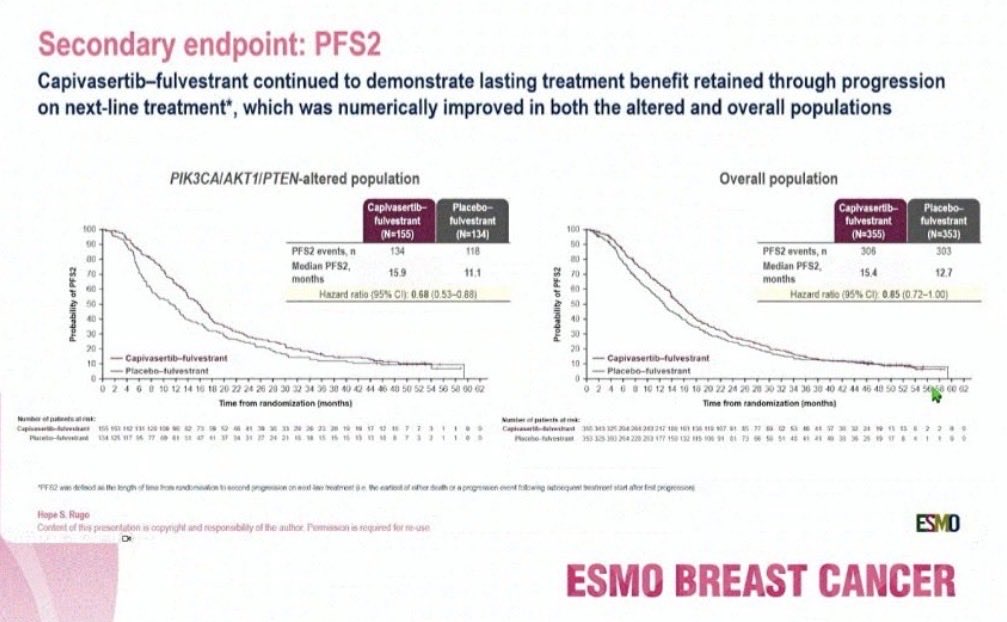
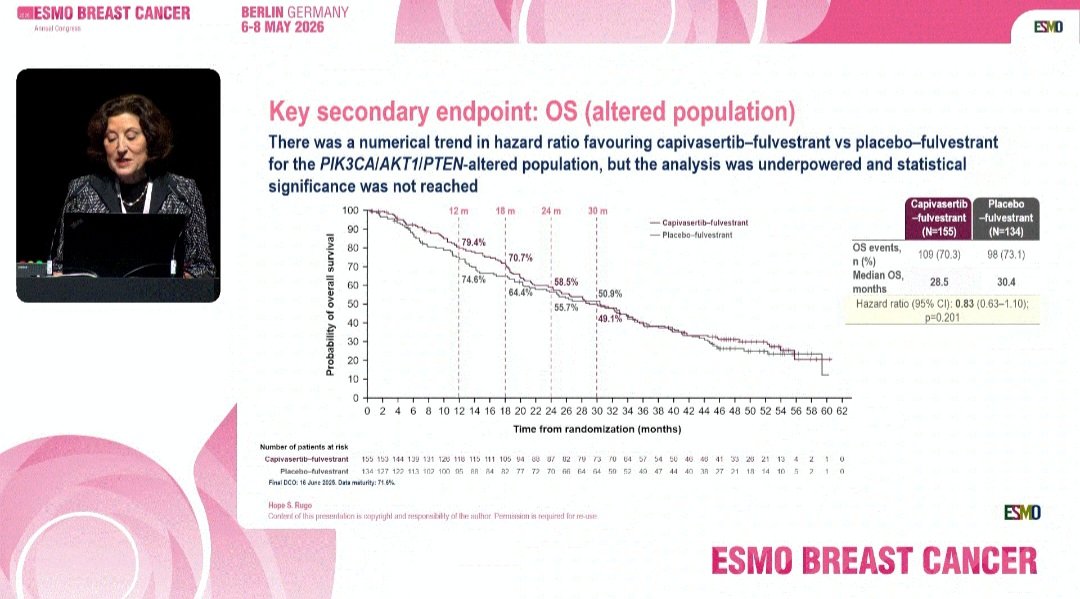
Primary PFS analysis: 7.2 months capivasertib+fulvestrant vs 3.6 months placebo+fulvestrant (HR 0.60, 95% CI 0.51–0.71; p<0.001) overall [NEJM 2023 / SABCS 2022, DCO1]; in the PIK3CA/AKT1/PTEN-altered cohort (n=289), median PFS was 7.3 months (95% CI 5.5–9.0) vs 3.1 months (95% CI 2.0–3.7); HR 0.50 (95% CI 0.38–0.65); p<0.0001 [FDA Drug Trials Snapshot / NEJM 2023]. Final OS analysis at ESMO Breast 2026 was NOT statistically significant: altered population median OS 28.5 vs 30.4 months (HR 0.83, 95% CI 0.63-1.10; p=0.201); overall population 29.4 vs 28.6 months (HR 1.00). However, PFS2 favoured capivasertib in both populations: altered 15.9 vs 11.1 months (HR 0.68); overall 15.4 vs 12.7 months (HR 0.85). Time to first subsequent chemo or death: altered 11.0 vs 6.0 months (HR 0.62); overall 11.0 vs 7.0 months (HR 0.74).
Patient-reported outcomes from CAPItello-291 demonstrated capivasertib-fulvestrant delayed time to deterioration of GHS/QOL and maintained other HRQoL dimensions similarly to fulvestrant — except for diarrhoea symptoms. Common AEs: diarrhoea, rash, hyperglycaemia, nausea. Generally manageable with dose modifications and supportive care. Importantly, the 4-days-on/3-days-off schedule attenuates target AKT inhibition toxicity.
Yakup Ergün cut to the central interpretive tension: “PFS benefit is clear; PFS2 also supports sustained disease control. No OS benefit was shown,” adding that “OS remains unproven and confounded by post-progression therapies.” Rishabh Jain asked the same question more bluntly — “Does capivasertib actually improve survival? CAPItello-291 final OS just answered this” — in the trial’s highest-impression post. Kazuki Nozawa offered a more favorable read, noting capivasertib + fulvestrant “continued to show durable benefit in PIK3CA/AKT1/PTEN-altered HR+/HER2− ABC, with meaningful PFS2 improvement and ~7-month OS gain after prior CDK4/6i.” Paolo Tarantino dug into the biomarker layer at SABCS25, flagging that “Most PIK3CA/AKT/PTEN alterations are found both on tissue and ctDNA, but about 10% are found only on one of the two methods” with “PTEN alterations the most discordant.” Hope Rugo — presenter of the final-OS analysis at ESMO Breast 2026 — flagged the trial-design caveat directly on her own slide: “Overall statistical significance was not observed in the altered population” for OS, with HR 1.00 (95% CI 0.83–1.19) in the altered cohort and HR 1.00 (0.82–1.23) in the overall population. The pre-specified exploratory PIK3CA/AKT1/PTEN-altered + prior CDK4/6i subgroup showed HR 0.78 (0.57–1.07), a ~7-month numerical OS gain that did not cross the statistical hierarchy. Rugo also pointed to the ctDNA biomarker work as supporting “both tissue and ctDNA evals” for patient selection. The most-discussed exchange of the meeting came when Rishabh Jain framed the result as “Does capivasertib actually improve survival? CAPItello-291 final OS just answered this,” and Rugo publicly corrected the framing in a quote-tweet: “Actually the trial was not powered at all for OS. Wait for the data. This was a secondary endpoint and the assumptions were not attainable. Pragmatic decisions.” The exchange — trial design vs. clinical interpretation — is the cleanest articulation of how to read CAPItello-291’s OS column.
CAPItello-291 is a Phase 3 randomized, double-blind trial (NCT04305496) of capivasertib (Truqap, an AKT inhibitor) plus fulvestrant versus placebo plus fulvestrant in patients with HR-positive, HER2-negative locally advanced or metastatic breast cancer whose disease progressed on endocrine therapy. Progression-free survival in the overall population and in the AKT-pathway (PIK3CA/AKT1/PTEN)-altered subgroup were co-primary endpoints.
In the AKT-pathway-altered subgroup (approximately 289 patients), capivasertib plus fulvestrant improved median progression-free survival to 7.3 versus 3.1 months with placebo plus fulvestrant (hazard ratio 0.50). A progression-free survival benefit was also seen in the overall population. At the ESMO Breast 2026 final analysis, overall survival was not statistically significant, so the clinical value rests on the progression-free survival benefit in biomarker-altered tumors.
Yes. On November 17, 2023 the FDA approved capivasertib (Truqap) with fulvestrant for adults with HR-positive, HER2-negative locally advanced or metastatic breast cancer harboring one or more PIK3CA, AKT1 or PTEN alterations, after progression on at least one endocrine-based regimen. The approval was based on the CAPItello-291 progression-free survival benefit in the biomarker-altered subgroup.
The approval is restricted to tumors with one or more PIK3CA, AKT1 or PTEN alterations, identified by an FDA-approved companion diagnostic (FoundationOne CDx). Patients without these AKT-pathway alterations are outside the approved indication.
The most common adverse event is diarrhea; hyperglycemia and rash are also characteristic and require monitoring and management, along with nausea. Patient-reported outcomes showed capivasertib-fulvestrant delayed time to deterioration of global health status/quality of life and maintained other HRQoL dimensions similarly to fulvestrant, except for diarrhea symptoms.
| Handle | Name | Sentiment | Tweet (excerpt) | Imp. |
|---|---|---|---|---|
| @hoperugo | Hope Rugo | Positive | #SABCS2025 Nick Turner presents our capi291 ctDNA data. Benefit seen in those without ESR1m and large genomic rearrangem… | 1,552 |
| @DrRishabhOnco | Dr Rishabh Jain | Neutral | 🔥 Does capivasertib actually improve survival? CAPItello-291 final OS just answered this 👇 Trial: Capivasertib + fulve… | 16,263 |
| @hoperugo | Hope Rugo | Neutral | Actually the trial was not powered at all for OS. Wait for the data. This was a secondary endpoint and the assumptions w… | 9,111 |
| @PTarantinoMD | Paolo Tarantino | Neutral | Interesting ctDNA sub-analysis from CAPItello291. Most PIK3CA/AKT/PTEN alterations are found both on tissue and ctDNA, b… | 4,372 |
| @kazuki_nozawa | Kazuki Nozawa, MD | Neutral | #ESMOBreast26 CAPItello-291 final OS: Capivasertib + fulvestrant continued to show durable benefit in PIK3CA/AKT1/PTEN-… | 1,704 |




















