Resectable stage II-IIIB NSCLC (perioperative) — Merck Sharp & Dohme LLC
Discover KOL Sentiment on KEYNOTE-671 →Design - Phase 3 perioperative pembrolizumab + neoadjuvant chemo -> adjuvant pembrolizumab vs placebo, resectable stage II-IIIB NSCLC (NCT03425643).
EFS - HR 0.58 (median not reached vs 17.0 mo); 5-yr EFS 49.9% vs 26.5%.
OS - HR 0.72 (95% CI 0.56-0.93, P=0.0103); 5-yr OS 64.6% vs 53.6%.
Safety - Grade >=3 AEs 44.9% vs 37.3%; AE discontinuation 13.0% vs 6.5%.
Regulatory - FDA approved October 2023.
Sponsor / drug - Merck (MSD); pembrolizumab (Keytruda).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.









Top tweets by impressions — click to view on X
Is it applicable for ANY patients?
But we will need to revise all of these thoughts in the wake of recent data presentations on AEGEAN, Neotorch, & upcoming #ASCO23 presentation of KEYNOTE-671.…
☑️#WCLC25 #LCSM Mini Oral Abstract🆙
🔥KEYNOTE-671 4-year update
🔥Perioperative Pembrolizumab in Non-Small Cell Cancer (NSCLC): 4-Year Outcomes by Nodal Status in the KEYNOTE-671 Study
🎙️…
🚦 pCR + MRD in periop NSCLC:
🔴 MRD+ = worst prognosis
▫️Will adj IO be enough?
🟡 MRD– / no pCR (~80%) = gray zone
▫️Who actually benefits (and is IO ‘right’)?
🟢 pCR + MRD– = best…
More news in early stage #lungcancer: @Merck announces Ph3 KEYNOTE-671 study results: Neoadj pembro/chemo ➡️ adju pembro ⬆️ EFS + ⬆️ MPR vs. neoadj chemo alone in stage II, IIIA, IIIB. #LCSM…
🆙 #ELCC26 @myESMO 🇩🇰
🔥Mini Oral session 2
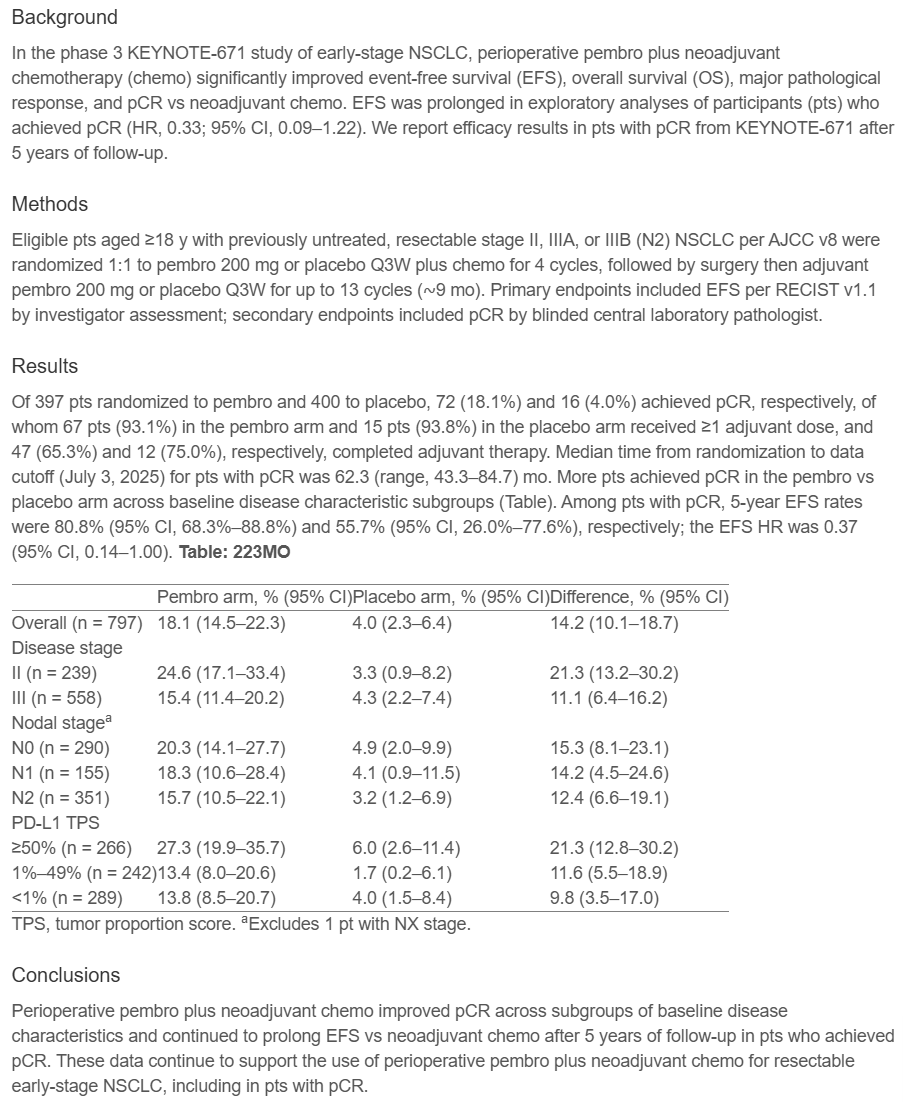
☑️KEYNOTE-671: 5 years F/U in pCR subgroup
🎯EFS HR 0.37, 5-y rate 80.8% vs. 55.7%
🎙️Dr. Margarita Majem
🎙️Chair: Dr. Kersti Oselin…

Today was the first time I observed @SalmaJabbour1 in a debate. It wouldn’t have mattered who was on the other side as she was absolutely spectacular using data and logic to clarify CRT is often the…
🆙 #ELCC26 @myESMO 🇩🇰
🔥Mini Oral session 2
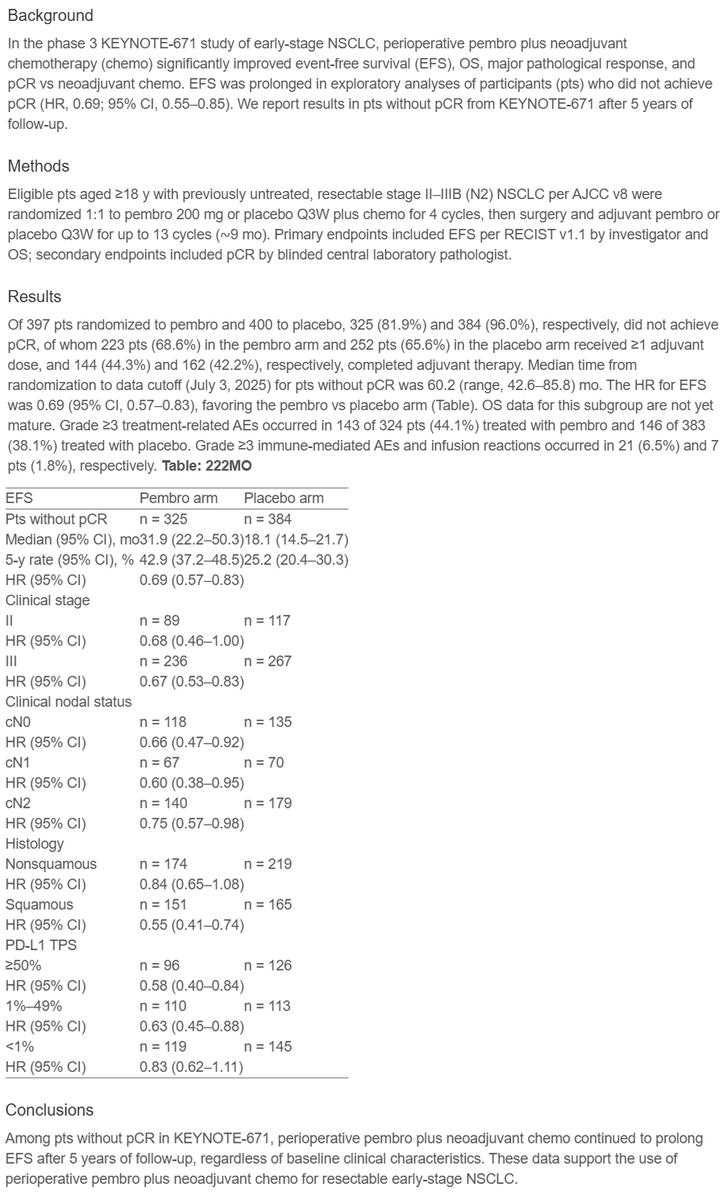
☑️KEYNOTE-671: 5 years F/U in non-pCR subgroup
🎯EFS HR 0.69, 5-y rate 42.9% vs. 25.2%, OS immature
🎙️ @MartinReck2
🎙️Chair: Dr. Kersti Oselin…

🔥 Does pCR translate into long-term benefit? #ELCC26
5-year outcomes from KEYNOTE-671 in early-stage NSCLC answer this 👇
🧬 Study population
• Resectable stage II–IIIB (N2) NSCLC
• Perioperative…
@SalmaJabbour1 and I are going all in for our debate on stage III lung cancer today at #TexasLung26 - it will be a ton of fun and sure to entertain!
The only winner will be our patients who have two…

#ELCC26 @MartinReck2 on KN671 exploratory analysis of patients without pCR
5-year EFS 43% vs 25% , HR =0,69, 95%CI 0.57-0.83) https://t.co/mFvqfzt6Wu
KEYNOTE-671 demonstrated both EFS and OS benefits with perioperative pembrolizumab + chemotherapy, leading to FDA approval October 2023. Alongside AEGEAN (durvalumab), CheckMate-77T (nivolumab), and CheckMate-816 (neoadjuvant-only nivolumab), establishes perioperative immunotherapy as a core stage II-IIIB NSCLC strategy. Choice among regimens individualized by clinical and biomarker factors.
Median: not reached (perioperative pembrolizumab) vs. 17.0 months (placebo + chemo). HR 0.58 (95% CI 0.46-0.72), P<0.001 5-year EFS (ELCC 2026 update) rate: 49.9% (pembrolizumab) vs. 26.5% (placebo). Primary analysis: EFS HR 0.58 (95% CI 0.46-0.72, P<0.001). pCR 18.1% vs. 4.0%; mPR 30.2% vs. 11.0%. 5-year update (ELCC 2026): median EFS 57.1 months (95% CI 38.0-NR) with pembrolizumab vs. 18.4 months (95% CI 14.8-22.1) with placebo; 5-year EFS rate 49.9% vs. 26.5%. pCR subgroup 5-yr EFS 80.8% vs. 55.7% (HR 0.37); non-pCR subgroup 5-yr EFS 42.9% vs. 25.2% (HR 0.69), demonstrating durable benefit even without pCR.
HR 0.72 (95% CI 0.56-0.93), P=0.0103 OS HR 0.72 (95% CI 0.56-0.93, P=0.0103) — 28% reduction in risk of death. Primary OS analysis at ESMO 2024 (P=0.00488) and 5-year update at ESMO 2025 / ELCC 2026 consistent. 5-year OS rate 64.6% (95% CI 59.5-69.2) with pembrolizumab vs. 53.6% (95% CI 48.3-58.6) with placebo. Median follow-up 60.4 months (range 42.6-85.8).
Grade ≥3 adverse events: 44.9% (pembro) vs. 37.3% (placebo). Discontinuation due to AEs: 13.0% (pembro) vs. 6.5% (placebo). Key AEs: neutropenia / chemo-related cytopenia, immune-related AEs (thyroid, skin). Treatment-related deaths 0.8% (pembro) vs. 0.3% (placebo). AE profile consistent with chemotherapy + checkpoint inhibitor combinations.
✅ Perioperative pembrolizumab established as SOC for resectable stage II-IIIB NSCLC. KEYNOTE-671 demonstrated both EFS and OS benefits with perioperative pembrolizumab + chemotherapy, leading to FDA approval October 2023. Alongside AEGEAN (durvalumab), CheckMate-77T (nivolumab), and CheckMate-816 (neoadjuvant-only nivolumab), establishes perioperative immunotherapy as a core stage II-IIIB NSCLC strategy. Choice among regimens individualized by clinical and biomarker factors.
KEYNOTE-671 is a Phase 3 randomized trial (NCT03425643) of perioperative pembrolizumab (Keytruda) - neoadjuvant pembrolizumab plus platinum-based chemotherapy followed by adjuvant pembrolizumab - versus neoadjuvant chemotherapy plus placebo in patients with resectable stage II-IIIB non-small cell lung cancer. Event-free survival and overall survival were the dual primary endpoints.
Event-free survival favored perioperative pembrolizumab with a hazard ratio of 0.58 (median not reached vs 17.0 months; 5-year EFS 49.9% vs 26.5%), and overall survival was significantly improved with a hazard ratio of 0.72 (95% CI 0.56-0.93, P=0.0103), a 28% reduction in the risk of death. The 5-year OS rate was 64.6% with pembrolizumab versus 53.6% with placebo.
Yes. In October 2023 the FDA approved pembrolizumab (Keytruda) with neoadjuvant platinum-containing chemotherapy and then continued as a single agent as adjuvant treatment for resectable (tumors >=4 cm or node-positive) NSCLC, based on KEYNOTE-671.
Grade >=3 adverse events occurred in 44.9% of pembrolizumab patients versus 37.3% with placebo, and treatment discontinuation due to adverse events was 13.0% versus 6.5%. Treatment-related deaths were uncommon (0.8% vs 0.3%). The profile is consistent with a chemotherapy-plus-checkpoint-inhibitor combination, with immune-related events (thyroid, skin) among the notable toxicities.
KEYNOTE-671 helped establish perioperative immunotherapy as a core approach for resectable stage II-IIIB NSCLC, alongside AEGEAN (durvalumab), CheckMate-77T (nivolumab), and the neoadjuvant-only CheckMate-816 (nivolumab). It is distinguished by demonstrating both an EFS and a statistically significant OS benefit.