Phase II PET-adapted, chemotherapy-free trastuzumab + pertuzumab in HER2+ early breast cancer. 5-year follow-up confirms ~90% iDFS in PET responders, ~30% chemo-free outcomes.
Discover KOL Sentiment on PHERGain →Design - Phase 2 PET-adapted, chemotherapy-free neoadjuvant trastuzumab + pertuzumab (dual HER2 blockade), HER2+ stage I-IIIA early breast cancer (NCT03161353); chemo added only for PET non-responders.
Strategy - De-escalation: ~30% of patients achieved excellent outcomes chemotherapy-free (PET responders with pathologic complete response).
Efficacy (5-yr) - 5-year follow-up confirms ~90% invasive disease-free survival in PET responders per the page.
Safety - Grade >=3 treatment-related AEs 33% (PET-adapted, Group B) vs 62% (full chemo, Group A); SAEs 14% vs 28%; PET-responder pCR subgroup had grade >=3 TRAEs of just 1% with no SAEs.
Regulatory - Investigational STRATEGY - not an FDA-registration trial; trastuzumab and pertuzumab are individually approved, the chemo-free PET-adapted algorithm is not.
Sponsor / drug - MEDSIR (investigator-initiated); trastuzumab (Herceptin) + pertuzumab (Perjeta).
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.







Trial slides shared by KOLs at ESMO Breast 2026 (#ESMOBreast26). Click any image to expand. OCR text extracted via AWS Textract.




[Slide 1] 2026 ESMO BREAST CANCER Annual Congress Chemotherapy-free, pathological complete response (pCR)-guided strategy with trastuzumab-pertuzumab (HP) and T-DM1 in HER2+ early breast cancer (EBC): PHERGain-2 Laia Garrigos, Manuel Ruiz-Borrego, Jose Manuel Perez-Garcia, Angel Guerrero-Zotano, Alfonso Cortes- Salgado, Sherko Kümmel, Marco Colleoni, Cristina Reboredo-Rendo, Begona Bermejo, Isabel Blancas, Joaquin Gavila, Alessandra Fabi, Olalla Ballesteros Griselda Martrat, Simona lacobucci, Olga Boix, Pau Berenguer-Molins, Daniel Alcala-Lopez, Javier Cortés, Antonio Llombart-Cussac May 6, 2026 ESMO ESMO BREAST CANCER --- [Slide 2] Content of this presentation is copyright and responsibility of the author Permission $ required for re-use PHERGain-2 Study Design TREATMENT Cohort A Key eligibility criteria pCRt Patients ≥ 18 years Histologically confirmed ypTO/is HP (+ET) x10 invasive carcinoma of ypNO the breast No prior treatment for At screening: Primary Endpoints Cohort B Central breast cancer HP (±ET) HER2 IHC 3+" x8 Breast MRI Surgery ypN0(i+) HER2 status T-DM1 (±ET) (1) >10% HRQoL ypN0(mol+) EoS & ypN1mi x10 decline rate Node-negative status Tumor size 5-30 mm MRI imaging (2) 3y-RFI rate (MRI) Cohort C ECOG PS 0/1 ChT' T-DM1 LVEF >55% ypN1-N3 (+ET) Adequate organ function HP: 600 mg H plus 1200 mg P loading x10 dose, then 600 mg H plus 600 mg P Physician's choice chemotherapy was allowed maintenance dose q3w before adjuvant T-DM1 T-DM1 3.6 mg/kg of body weight q3w ET up to 5 years and radiotherapy as per Follow-up* HR status and institutional practices PROs assessments: Baseline D1C1-C8 ≤14d pre-op Adj D1C1 FU q3m x2y FU q6m x3y Annual to EOS *According to the 2018 American Society of Clinical Oncology/College of American Pathologists criteria TAII patients who were hormonal receptor positive received ET concomitantly with HP or T-DM1 ET was sex and menopausal status based premenopausal and perimenopausal women receive ovarian function suppression plus tamoxifen (20 mg/day orally) or letrozole (2 5 mg/day orally). postmenopausal women receive letrozole (2 5 mg/day orally), and men receive tamoxofen (20 mg/day orally) *All patients must be followed up for 5 years from when the last patient has completed surgery (EoS). even if the assigned treatment is discontinued permanently Chl, chemotherapy, ECOGPS Eastem Cooperative Oncology Group performance status d, day, EoS end of study ET endocne therapy FU, follow-up, HER2 human epidemal growth factor receptor 2. HP trasturumab and pertuzumab, HRQoL health related quality of life IHC, immunohistochemistry, LVEF, left ventricular ejection fraction, m, month MRI, magnetic resonance imaging pCR pathological complete response, PRO patient reported outcomes RFI recurrence free survival; q3w, every three weeks y. year ESMO BREAST CANCER --- [Slide 3] Secondary endpoint: pCR rate by HR status and tumor size Median (range) T1 tumor size: 16mm (7-20) Median (range) T2 tumor size: 23 5mm (21-30) 100 pCR rate 100 100 59.6% 63.0% 59.6% 95% CI 54.6-64.4 95% CI 53.1-72.1 95% CI 53.3-65.7 80 80 80 59.6% 58.3% Pathological complete response (%) 95% CI 51.0-67.7 95% CI 52.4-64.1 60 60 60 40 40 40 236 / 396 68 108 168 288 152/255 84 141 20 20 20 0 0 0 All participants HR- HR+ T1 T2 Fisher's exact test Fisher's exact test P 0.42 P 1.00 Dr. Antonio Llombart-Cussac Content of this presentation IS copynght and responsibility of the author Permission is required for to use ESMO CI. confidence interval HR hormone receptor, pCR pathological complete response ESMO BREAST CANCER --- [Slide 4] ESMO BREAST CANCER BERLIN GERMANY Annual Congress 6-8 MAY 2026 ESMD Conclusion PHERGain-2 suggests maintenance of HRQoL over one year of treatment, although interpretation is limited by treatment heterogeneity and lack of a direct comparator Patients without pCR experienced greater HRQoL deterioration, likely reflecting treatment escalation (T-DM1 ± chemotherapy) The pCR rate of 59.6% observed with this chemotherapy-free strategy is encouraging, particularly in a population including HR-positive disease The safety profile was consistent with known effects of trastuzumab/pertuzumab and T-DM1 Pending mature efficacy outcomes (3-year RFI), this response-adapted, chemotherapy-free, strategy appears clinically feasible and may support treatment individualization in selected low-risk patients Dr. Antonio Liombart Cussac Content of this presentation is copyright and responsability of the author Pomission is required for DO use ESMO ESMO BREAST CANCER
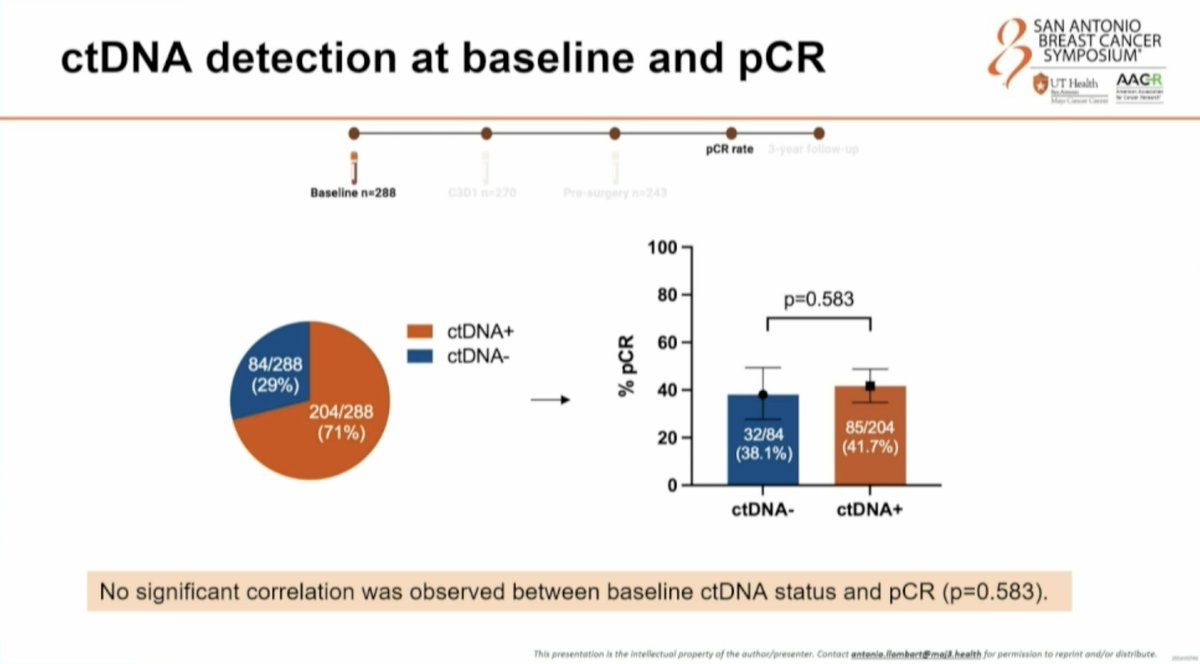



[Slide 1] SAN ANTONIO BREAST CANCER ctDNA detection at baseline and pCR SYMPOSIUM UT Health AAGR - - Mays Classes Carese . - - pCR rate 3-year follow-up j Baseline n=288 0301 n=270 Pre-surgery n=243 100 80 p=0.583 ctDNA+ 60 84/288 ctDNA- (29%) % pCR 40 204/288 (71%) 32/84 85/204 20 (38.1%) (41.7%) 0 ctDNA- ctDNA+ No significant correlation was observed between baseline ctDNA status and pCR (p=0.583). This presentation in the intellectual property of the author/presenter. Contact antenie llembert@maj3 health for permission to reprint and/or distribute --- [Slide 2] SAN ANTONIO BREAST CANCER Early ctDNA dynamics and pCR SYMPOSIUM UT Health AAGR No./ - - - - Mays Casses pCR rate 3-year follow-up Baseline n=288 C3D1 n=270 surgery n=243 p<0.001 100 18% 100 24% ctDNA+ 80 80 p=0.003 71% ctDNA+ % PET response 60 60 76% 114/126 82% % pCR 40 (90.5%) 40 ctDNA- 61/126 23/41 29% 20 20 (48.4%) 97% (56.1%) 9/41 | ctDNA- (22.0%) 0 0 Baseline C3D1 No ctDNA ctDNA No ctDNA ctDNA clearance clearance clearance clearance A 76% relative reduction in ctDNA positivity was achieved after 2 treatment cycles. ctDNA clearance after two cycles strongly correlated with PET response (p<0.001) and pCR (p=0.003). This presentation is the intellectual property of the author/presenter. Contact antonio.lfombart@maj3.heaith . for permission to reprint and/or distribute --- [Slide 3] SAN ANTONIO BREAST CANCER Late ctDNA dynamics and pCR SYMPOSIUM UT Health AAGR I - - Mays Casse . I pCR rate 3-year follow-up Baseline n=288 C301 n=270 Pre-surgery n=243 100 17% 12% ctDNA+ 80 p<0.001 70% ctDNA+ 60 83% % R pCR 88% 40 ctDNA- 0/28 61/124 20 (0.0%) (49.2%) 30% ctDNA- 98% 0 Baseline Pre-surgery No ctDNA ctDNA clearance clearance A 83% relative reduction in ctDNA positivity was achieved prior to surgery. ctDNA clearance at the presurgical time point (p<0.001) was significantly associated with achieving a pCR. No patient with detectable ctDNA prior to surgery (n=28) achieved a pCR. This presentation is the intellectual property of the author/presenter. Contact antonia.liombert@maj3.heaith . L for permission to reprint and/or distribute --- [Slide 4] SAN ANTONIO BREAST CANCER Basal ctDNA status and 3-year iDFS rate SYMPOSIUM UT Health AAGR - - - Mays Casses - - PCR rate 3-year follow-up Baseline n=288 0301 n=270 Pre-surgery n=243 100% Hazard ratio 95% 4.1 iDFS (%) 90% (95% CI 0.7; 23.5) p=0.046 85% Group Events/Total (%) 3-year IDFS 80% ctDNA. 0/81 (0.0%) 100.0% (100.0; 100.0) ctDNA+ 14/192 (7.3%) 92.5% (68.8;96.4) 0% 0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 Time (years) Number at risk 81 78 77 77 76 76 76 7 192 189 187 183 178 176 169 21 ON : ctDNA positivity at baseline was associated with a worse 3-year iDFS. This presentation is the intellectual property of the author/presenter. Contact antonio llembert@maj3 health for permission to reprint and/or distribute



[Slide 1] SAN ANTONIO BREAST CANCER PHERGuide: methodology and objectives SYMPOSIUM UT Health AACR - - - - - Objective 1: assess the Neoadjuvant treatment PET (total body) pCR rate correlation between ctDNA detection and pCR Diagnosis Objective 2: evaluate the 3-year follow-up association between ] ctDNA detection and/or Baseline n=336 C3D1 n=311 Pre-surgery n=285 clearance with patient outcomes ctDNA isolation and analysis Guardant Reveal™ Tissue-free epigenomic assay: ctDNA detection+estimated tumor fraction This presentation is the intellectual property of the author/presenter. Contact antonio llombart@maj3 health for permission to reprint and/or distribute --- [Slide 2] SAN ANTONIO BREAST CANCER Early ctDNA dynamics and pCR SYMPOSIUM UT Health AACR I pCR rate 3-year follow-up Baseline n=288 C3D1 n=270 surgery n=243 p<0.001 18% 100 100 24% ctDNA+ 80 80 71% p=0.003 ctDNA+ % PET response 60 60 76% 114/126 82% (90.5%) % pCR 40 40 ctDNA- 23/41 61/126 29% 20 97% (56.1%) 20 (48.4%) 9/41 ctDNA- (22.0%) Baseline 0 0 C3D1 No ctDNA ctDNA No ctDNA ctDNA clearance clearance clearance clearance A 76% relative reduction in ctDNA positivity was achieved after 2 treatment cycles. ctDNA clearance after two cycles strongly correlated with PET response (p<0.001) and pCR (p=0.003). This presentation is the intellectual property of the outhor/presenter. Contact --- [Slide 3] SAN ANTONIO BREAST CANCER Late ctDNA dynamics and pCR SYMPOSIUM UT Health AACR - pCR rate 3-year I Baseline n=288 C3D1 270 Pre-surgery n=243 100 17% 12% ctDNA+ 80 p<0.001 70% ctDNA+ 60 83% % pCR 88% 40 ctDNA- 0/28 61/124 20 (0.0%) (49.2%) 30% ctDNA- 98% 0 Baseline Pre-surgery No ctDNA ctDNA clearance clearance A 83% relative reduction in ctDNA positivity was achieved prior to surgery. ctDNA clearance at the presurgical time point (p<0.001) was significantly associated with achieving a pCR. No patient with detectable ctDNA prior to surgery (n=28) achieved a pCR. This presentation is the intellectual property of the outhor/presenter. Contact antonio.llombart@maj3.health for permission to reprint and/or distribute




[Slide 1] Secondary endpoint: pCR rate by HR status and tumor size Median (range) T1 tumor size: 16mm (7-20) Median (range) T2 tumor size: 23.5mm (21-30) 100 pCR rate 100 100 59.6% 63.0% 59.6% 95% CI 54.6-64.4 95% CI 53.1-72.1 95% CI 53.3-65.7 80 80 80 59.6% 58.3% Pathological complete response (%) 95% CI 51.0-67.7 95% CI 52.4-64.1 60 60 60 I 40 40 40 236 / 396 68 / 108 168/288 20 152/255 20 84 141 20 0 0 0 All participants HR- HR+ T1 T2 Fisher's exact test Fisher's exact test P 0.42 P = 1.00 Dr. Antonio Llombart-Cussac Content of this presentation is copyright and responsibility of the author. Permission is required for re-use ESMO CI, confidence interval; HR, hormone receptor; pCR pathological complete response --- [Slide 2] Primary safety endpoint: >10% HRQoL decline rate at one year >10% HRQoL decline rate Patient-reported outcomes N = 396 ; n (%) 42.8 % Completion rate at baseline 391 (98.7) 95% CI 36.9-48.8 Baseline HRQoL score, mean (95% CI) 78.6 (76.8-8 0.5) Completion rate at 1 year 360 (90.9) HR positive: 45.2% (95% CI 38.3-52.3) Fisher's exact test 1-year HRQoL score, mean (95% CI) 69.6 (67.5-71.8) HR negative: 36.1% (95% CI 25.4-47.9) p=0.11 n (%), number of patients (percentage based on N); N, Number of patients. Patient reported outcomes were analyzed on patients who received at least one dose of study treatment and completed baseline and at least one follow-up questionnaire 1- year post-neoadjuvant treatment Patients without a >10% decline at one year who discontinued the study due to disease progression, toxicity or death within the first year after starting neoadjuvant treatment were considered events. Dr. Antonio Llombart-Cussac Content of this presentation is copyright and responsibility of the author Permission is required for re-use ESMO CI, confidence interval; HR, hormone receptor, HRQoL, health-related quality of life --- [Slide 3] Baseline Characteristics N = 396 N = 396 Patient baseline characteristics Primary tumor baseline characteristics n (%) n (%) Age; Median (range) (years) 55 (24-85) Median tumor size (mm, Min; Max) 18 (7-30) Sex T stage mm Woman 394 (99.5) T1b/T1c: >5 to <20 244 (61.6) T2: >20 to <30 152 (38.4) Menopausal status Histologic grade Postmenopausal 235 (59.3) Gx* 57 (14.4) Premenopausal 159 (40.2) G1 21 (5.3) Not available 2 (0.5) G2 185 (46.7) ECOG performance status G3 133 (33.6) 0 382 (96.5) HER2 IHC 3+ 396 (100) 1 14 (3.5) Hormonal receptor status Multifocal or multicentric breast cancer 15 (3.8) Negative 108 (27.3) ECOG PS, Eastern Cooperative Oncology Group performance status; HER2, human epidermal growth factor receptor 2; Positive 288 (72.7) IHC, immunohistochemistry Tumor staging was assessed as per American Joint Committee on Cancer staging manual, 8th edition "Differentiation status could not be assessed "All patients who were hormonal receptor-positive received ET concomitantly with HP or T-DM1 ET was sex- and menopausal status-based premenopausal and perimenopausal women receive ovanan function suppression plus tamoxifen (20 mg/day orally) or letrozole (2.5 mg/day orally); postmenopausal women receive letrozole (2.5 mg/day orally); and men receive tamoxifen (20 Dr. Antonio Llombart-Cussac mg/day orally). Content of this presentation is copyright and responsibility of the author Permission is required for re-use n (%), number of patients (percentage based on N); N, Number of patients. ESMO --- [Slide 4] Content of this presentation is copyright and responsibility of the author, Permission is required for no-use. PHERGain-2 Study Design TREATMENT Key eligibility criteria Cohort A pCR' Patients 2 18 years Histologically confirmed ypTO/is HP (±ET) x10 invasive carcinoma of ypNO the breast Primary Endpoints No prior treatment for At screening: Cohort B Central breast cancer HP (±ET) HER2 IHC 3+* x8 Breast MRI Surgery ypN0(i+) HER2 status T-DM1 (±ET) (1) >10% HRQoL ypN0(mol+) EoS & ypN1mi x10 decline rate Node-negative status Tumor size 5-30 mm MRI imaging (2) 3y-RFI rate (MRI) Cohort C ECOG PS 0/1 ChT' + T-DM1 LVEF >55% ypN1-N3 (±ET) Adequate organ function HP: 600 mg H plus 1200 mg P loading x10 dose, then 600 mg H plus 600 mg P Physician's choice chemotherapy was allowed maintenance dose q3w before adjuvant T-DM1 T-DM1: 3.6 mg/kg of body weight q3w ET up to 5 years and radiotherapy as per Follow-up® HR status and institutional practices PROs assessments: Baseline D1C1-C8 ≤14d pre-op Adj D1C1 FU q3m x2y FU q6m x3y Annual to EOS "According to the 2018 American Society of Clinical Oncology/College of American Pathologists criteria. TAII patients who were hormonal receptor-positive received ET concomitantly with HP or T-DM1. ET was sex- and menopausal status-based: premenopausal and perimenopausal women receive ovarian function suppression plus tamoxifen (20 mg/day orally) or letrozole (2.5 mg/day orally); postmenopausal women receive letrozole (2.5 mg/day orally); and men receive tamoxifen (20 mg/day orally). *All patients must be followed up for 5 years from when the last patient has completed surgery (EoS), even if the assigned treatment is discontinued permanently. ChT, chemotherapy; ECOG PS, Eastern Cooperative Oncology Group performance status; d, day, EoS, end of study; ET, endocrine therapy, FU, follow-up; HER2, human epidermal growth factor receptor 2; HP, trastuzumab and pertuzumab; HRQoL, health-related quality of life; IHC, immunohistochemistry; LVEF, left ventricular ejection fraction; m, month; MRI, magnetic resonance imaging; pCR pathological complete response; PRO, patient reported outcomes; RFI, recurrence-free survival; q3w, every three weeks; y. year




[Slide 1] Content of this presentation is copyright and responsibility of the author. Permission is required for re-use. PHERGain-2 Study Design TREATMENT Key eligibility criteria Cohort A pCR Patients 2 18 years Histologically confirmed ypTO/is HP (±ET) x10 invasive carcinoma of ypNO the breast Primary Endpoints No prior treatment for At screening: Cohort B Central breast cancer HP (±ET) HER2 IHC 3+* x8 Breast MRI Surgery ypN0(i+) HER2 status T-DM1 (±ET) (1) >10% HRQoL ypN0(mol+) EoS & ypN1mi x10 decline rate Node-negative status Tumor size 5-30 mm MRI imaging (2) 3y-RFI rate (MRI) Cohort C ECOG PS 0/1 ChT' T-DM1 LVEF >55% ypN1-N3 (+ET) Adequate organ function HP: 600 mg H plus 1200 mg P loading x10 dose, then 600 mg H plus 600 mg P Physician's choice chemotherapy was allowed maintenance dose q3w before adjuvant T-DM1 T-DM1: 3.6 mg/kg of body weight q3w ET up to 5 years and radiotherapy as per Follow-up* HR status and institutional practices PROs assessments: Baseline D1C1-C8 <14d pre-op Adj D1C1 FU q3m x2y FU q6m x3y Annual to EOS "According to the 2018 American Society of Clinical Oncology/College of American Pathologists criteria. TAII patients who were hormonal receptor-positive received ET concomitantly with HP or T-DM1. ET was sex- and menopausal status-based premenopausal and perimenopausal women receive ovanan function suppression plus tamoxifen (20 mg/day orally) or letrozole (2.5 mg/day orally); postmenopausal women receive letrozole (2.5 mg/day orally): and men receive tamoxifen (20 mg/day orally). *All patients must be followed up for 5 years from when the last patient has completed surgery (EoS), even if the assigned treatment is discontinued permanently ChT, chemotherapy, ECOG PS, Eastern Cooperative Oncology Group performance status; d, day, EoS, end of study, ET, endocrine therapy, FU, follow-up; HER2, human epidermal growth factor receptor 2; HP, trastuzumab and pertuzumab; HRQoL. health related quality of life; IHC, immunohistochemistry, LVEF, left ventricular ejection fraction; m, month; MRI, magnetic resonance imaging pCR pathological complete response; PRO, patient-reported outcomes; RFI, recurrence-free survival; q3w, every three weeks; y. year --- [Slide 2] Baseline Characteristics N = 396 N = 396 Patient baseline characteristics Primary tumor baseline characteristics n (%) n (%) Age; Median (range) (years) 55 (24-85) Median tumor size (mm, Min; Max) 18 (7-30) Sex T stage1, mm Woman 394 (99.5) T1b/T1c: >5 to <20 244 (61.6) T2: >20 to <30 Menopausal status 152 (38.4) Postmenopausal 235 (59.3) Histologic grade Gx* 57 (14.4) Premenopausal 159 (40.2) G1 21 (5.3) Not available 2 (0.5) G2 185 (46.7) ECOG performance status G3 133 (33.6) 0 382 (96.5) HER2 IHC 3+ 396 (100) 1 14 (3.5) Hormonal receptor status Multifocal or multicentric breast cancer 15 (3.8) Negative 108 (27.3) ECOG PS, Eastern Cooperative Oncology Group performance status; HER2, human epidermal growth factor receptor 2; Positive 288 (72.7) IHC, immunohistochemistry Tumor staging was assessed as per American Joint Committee on Cancer staging manual, 8th edition "Differentiation status could not be assessed *All patients who were hormonal receptor-positive received ET concomitantly with HP or T-DM1. ET was sex- and menopausal status-based premenopausal and perimenopausal women receive ovanan function suppression plus tamoxifen (20 mg/day orally) or letrozole (2.5 mg/day orally); postmenopausal women receive letrozole (25 mg/day orally); and men receive tamoxifen (20 Dr. Antonio Llombart-Cussac mg/day orally). Content of this presentation is copyright and responsibility of the author. Permission is required for re-use n (%), number of patients (percentage based on N); N, Number of patients ESMO --- [Slide 3] Primary safety endpoint: >10% HRQoL decline rate at one year ≥10% HRQoL decline rate Patient-reported outcomes N = 396 ; n (%) Completion rate at baseline 391 (98.7) 42.8% 95% CI 36.9-48.8 Baseline HRQoL score, mean (95% CI) 78.6 (76.8-8 0.5) Completion rate at 1 year 360 (90.9) HR positive: 45.2% (95% CI 38.3-52.3) Fisher's exact test 1-year HRQoL score, mean (95% CI) 69.6 (67.5-71.8) HR negative: 36.1% (95% CI 25.4-47.9) p 0.11 n (%), number of patients (percentage based on N); N, Number of patients. Patient reported outcomes were analyzed on patients who received at least one dose of study treatment and completed baseline and at least one follow-up questionnaire 1. year post-neoadjuvant treatment Patients without a >10% decline at one year who discontinued the study due to disease progression, toxicity or death within the first year after starting neoadjuvant treatment were considered events Dr. Antonio Llombart-Cussac Content of this presentation is copyright and responsibility of the author Permission is required for re-use ESMO CI, confidence interval; HR, hormone receptor, HRQoL, health-related quality of life --- [Slide 4] Secondary endpoint: pCR rate by HR status and tumor size Median (range) T1 tumor size: 16mm (7-20) Median (range) T2 tumor size: 23.5mm (21-30) 100 pCR rate 100 100 59.6% 63.0% 59.6% 95% CI 54.6-64.4 95% CI 53.1-72.1 95% CI 53.3-65.7 80 80 80 59.6% 58.3% Pathological complete response (%) 95% CI 51.0-67.7 95% CI 52.4-64.1 60 60 60 40 40 40 236 / 396 68 / 108 168 / 288 152/255 20 84 141 20 20 0 0 0 All participants HR- HR+ T1 T2 Fisher's exact test Fisher's exact test p=0.42 P 1.00 Dr. Antonio Liombart-Cussac Content of this presentation is copyright and responsibility of the author Permission is required for re-use. ESMO CI, confidence interval; HR, hormone receptor, pCR pathological complete response

[Slide 1] 216 RO: 5-year iDFS of the strategy-based, randomized phase II PHERGain trial evaluating chemotherapy de-escalation in HER2+ early breast cancer (EBC) patients. Cortes J et al PHERGain randomization 1:4 Phase 2 study (June 2017-April 2019) HP Basal: PET scan (total body) pCR ET* x10 F-FDG-PET-based, pCR-adapted Group A N=71 HP N=285 ET*x2 PET scan (Total body) 70% Stage II; 62% ER+/HER2+ PET HP responders ET* x6 Surgery Follow-up PET-responders: 38% pCR Group B TCHP x6 No adjuvant T-DM1 following residual non-pCR HP #ET* x4 PET disease non- TCHP HP responders x6 ET* x10 3y-IDFS:94% Baseline C3D1 Pre-surgery 100% 100% 75% Invasive Disease-Free Survival (IDFS) Invasive Disease Free Survival (IDFS) 75% 5-year iDFS rate in group B: PET responders with pCR 5-year iDFS rate in group B: 89.5% (95% CI: 85.7-93.4) and no chemo: 92.4% (95% CI: 86.7-98.5) 50% 50% 25% 25% 5-year DFS rate in group B 89 5% (95% CI: 85 7-93-4) 0% 5-year IDFS rate in group 8 PET responders with pCR: 92-4% (95% Ct: 06 7-98 5) 0 1 2 3 4 5 0% Time since surgery (years) 0 1 2 3 4 5 Patients risk Patients risk Time since surgery (years) Group 267 261 253 242 202 192 56 84 54 80 69 65 1/3 never received chemo 1 patient with distant recurrence Sonia Pernas, MD, PhD Content of this presentation is copyright and responsibility of the author Permission is required for re use MO


Highest-engagement tweets about this trial, ranked by KOL discussant count (replies + quote-tweets). Replies in green, quote-tweets in blue. Wall Street, stock-promo, and non-substantive replies excluded.
Phergain ctDNA using Guardant Reveal At baseline, 71% detectable No assoc of baseline ctDNA and pCR but assoc w/ worse 3 yr iDFS (HR 4.1, p=0.046) Clearance at C3D1 assoc with pCR ctDNA positivity prior to surgery (17%) has worse iDFS (HR 5.1) @OncoAlert #SABCS25
#ESMOBreast26 Can we safely reduce chemotherapy in HER2+ early breast cancer? 👀 PHERGain-2 tested a pCR-guided strategy with HP ± T-DM1. 📊 Key findings: ✅ pCR: 59.6% ✅ Similar across HR+ / HR- ✅ Similar in T1 vs T2 ✅ HRQoL maintained ⚠️ 3-year RFI still immature. 💡 https://t
GS1-06 – #SABCS25 ctDNA predict pCR and outcomes in HER2+ eBC in PHERGain: - ctDNA clearance after 2 cycles and pre-surgery strongly correlated w pCR - Baseline ctDNA+ linked to worse 3y iDFS ➡️No patient with ctDNA+ before surgery achieved pCR ! @OncoAlert @SABCSSanAntonio ht
PHERGain-2: Chemotherapy Free Dual HER2 Blockade Achieves ~60% pCR with Preserved HRQoL—Operationalizing a De-escalation, "Minimum Effective Treatment" Strategy in Low Risk HER2+ Early #BreastCancer @OncoAlert #ESMOBreast26 https://t.co/LSBoAXoB2A
PHERGain is an international, multicentre, randomized open-label Phase II trial that pioneered a PET-guided, pCR-adapted chemotherapy de-escalation strategy in HER2-positive Stage I–IIIA early breast cancer. Originally published in The Lancet (2024) showing 3-year iDFS of 94.8%, the 5-year follow-up presented at ESMO Breast 2026 confirms durability of this approach with close to 90% of patients remaining recurrence-free five years after surgery — establishing the strategy as a safe and durable alternative for the ~30% of HER2+ EBC patients who can avoid chemotherapy entirely.
Population: 356 patients with centrally confirmed HER2-positive, Stage I–IIIA invasive operable breast cancer with at least one PET-evaluable lesion. Group A: n=71. Group B: n=285. 89% (Group A) and 94% (Group B) proceeded to surgery.
Interventions: Group A: docetaxel + carboplatin + trastuzumab + pertuzumab (TCHP). Group B: trastuzumab + pertuzumab × 2 cycles → FDG-PET response assessment → PET-responders continued chemo-free trastuzumab-pertuzumab; PET non-responders switched to TCHP. Adjuvant therapy guided by pCR.
Endpoints: Primary: 3-year iDFS in Group B (met). Secondary: pCR in PET-responders, safety, 5-year iDFS (this update), ctDNA biomarker analyses.
5-year follow-up confirms close to 90% of Group B patients remain free from relapse, validating the durability of the PET-guided, pCR-adapted de-escalation strategy. Approximately one-third of patients successfully omitted chemotherapy. Earlier 3-year iDFS was 94.8% (95% CI 91.4-97.1). ctDNA analysis is emerging as a complementary biomarker for identifying patients with the best prognosis vs those who may need more intensive treatment.
TRAEs and SAEs were numerically higher in Group A (full chemo) than Group B (PET-adapted): grade ≥3 62% vs 33%; SAEs 28% vs 14%. Group B PET-responders with pCR had the lowest incidence of grade ≥3 TRAEs (1%) without any SAEs — the cleanest tolerability profile.
Sara Tolaney highlighted the PHERGain ctDNA biomarker readout using Guardant Reveal, noting that “At baseline, 71% detectable. No assoc of baseline ctDNA and pCR but assoc w/ worse 3 yr iDFS (HR 4.1, p=0.046). Clearance at C3D1 assoc with pCR. ctDNA positivity prior to surgery (17%) has worse iDFS (HR 5.1).” Luca Arecco amplified the finding from SABCS25, writing that “ctDNA clearance after 2 cycles and pre-surgery strongly correlated w pCR” and that “Baseline ctDNA+ linked to worse 3y iDFS,” punctuating the takeaway: “No patient with ctDNA+ before surgery achieved pCR!” The KOL conversation around the 5-year PHERGain follow-up centered on this ctDNA-guided de-escalation question: can pre-surgical liquid biopsy identify which patients can safely stay chemo-free, and which need rescue intensification?
PHERGain is an investigator-initiated Phase 2 randomized trial (NCT03161353) testing a 18F-FDG-PET-adapted, chemotherapy-free neoadjuvant strategy for HER2-positive stage I-IIIA early breast cancer. Patients receive dual HER2 blockade (trastuzumab plus pertuzumab, with endocrine therapy for HR-positive disease), and chemotherapy is added only for tumors that do not respond on PET imaging.
PHERGain demonstrated that a substantial proportion of patients (approximately 30%) can achieve excellent outcomes without chemotherapy. The 5-year follow-up confirmed roughly 90% invasive disease-free survival in PET responders, supporting PET-guided de-escalation for carefully selected HER2-positive early breast cancer.
No. PHERGain evaluates a treatment de-escalation strategy, not a new drug, and it is not an FDA-registration trial. Trastuzumab (Herceptin) and pertuzumab (Perjeta) are individually FDA approved for HER2-positive breast cancer, but the PET-adapted, chemotherapy-free algorithm studied in PHERGain is investigational and not an approved standard.
Grade 3 or higher treatment-related adverse events were markedly lower with the PET-adapted approach than with full chemotherapy (33% versus 62%), as were serious adverse events (14% versus 28%). PET responders who achieved a pathologic complete response had the cleanest tolerability, with grade 3 or higher treatment-related adverse events of only 1% and no serious adverse events.
PHERGain applies to HER2-positive stage I-IIIA operable early breast cancer, using early 18F-FDG-PET imaging after two cycles of dual HER2 blockade to identify metabolic responders who may avoid chemotherapy. It is a research strategy; decisions to de-escalate outside a trial should be individualized and discussed with a multidisciplinary team.
| Handle | Name | Sentiment | Tweet (excerpt) | Imp. |
|---|---|---|---|---|
| @GaiaGriguolo | Gaia Griguolo | Positive | ctDNA analysis in the PHERGAIN trial at #sabcs25 ✅early ctDNA clearance is associated with pCR ✅ctDNA at baseline and … | 575 |
| @DrRishabhOnco | Dr Rishabh Jain | Neutral | #ESMOBreast26 Can we safely reduce chemotherapy in HER2+ early breast cancer? 👀 PHERGain-2 tested a pCR-guided strateg… | 2,494 |
| @stolaney1 | Sara Tolaney | Neutral | Phergain ctDNA using Guardant Reveal At baseline, 71% detectable No assoc of baseline ctDNA and pCR but assoc w/ worse … | 1,374 |
| @Lucarecco | Luca Arecco, MD | Neutral | GS1-06 – #SABCS25 ctDNA predict pCR and outcomes in HER2+ eBC in PHERGain: - ctDNA clearance after 2 cycles and pre-surg… | 643 |
| @Dr_Oncologista | Aya Mohamed | MSc, MD 🎗 | Neutral | PHERGain-2: Chemotherapy Free Dual HER2 Blockade Achieves ~60% pCR with Preserved HRQoL—Operationalizing a De-escalation… | 574 |


















