Phase II UK trial of ctDNA-guided early switch to fulvestrant + palbociclib in HR+/HER2- early breast cancer. 11.3% MRD detection rate; 42.9% concurrent recurrence.
Discover KOL Sentiment on TRAK-ER →Design - Phase 2 investigator-initiated trial: serial ctDNA (molecular residual disease) surveillance to guide an early switch to fulvestrant (Faslodex) + palbociclib (Ibrance) before overt relapse in high-risk HR+/HER2- early breast cancer (NCT04985266; Royal Marsden / ICR, NIHR).
Surveillance yield - Across 2,110 samples from 480 patients, ctDNA was detected in 2.6% of individual tests; 11.3% of patients had ctDNA detected at least once, with higher detection at the first surveillance timepoint.
Concurrent recurrence - 42.9% of ctDNA-positive patients already had concurrent radiological recurrence at the time of ctDNA detection - a key finding for the lead-time question.
Assay performance - The personalized panel design failed in 14.8-16.1% of patients (insufficient tumor material or no trackable variants); the interim surveillance phase is observational with no treatment exposure.
Regulatory / sponsor - Investigational strategy; fulvestrant and palbociclib are approved in metastatic disease but the early-switch strategy here is investigational. Sponsor Royal Marsden / ICR (NIHR). ESMO Breast 2026.
Compiled and reviewed by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated July 21, 2026.







Trial slides shared by KOLs at ESMO Breast 2026 (#ESMOBreast26). Click any image to expand. OCR text extracted via AWS Textract.

[Slide 1] ctDNA SURVEILLANCE IN HR+ BREAST CANCER XXX TRAK-ER STUDY: SIGNAL VS REALITY GOAL: Detect molecular relapse earlier than imaging to guide intervention 1 HOW OFTEN IS ctDNA 2 TIMING MATTERS 3 WHAT DOES THIS MEAN? DETECTED? Metastatic disease rate at ctDNA detection Detection rate 2.6% 62% L declines over time DETECTION FIRST TEST (MO) PER TEST Most early positives already Early test = have metastatic disease lower utility 11.3% 16% Serial testing improves PATIENTS EVER LATER TESTS (M3+) chance of catching ctDNA POSITIVE MRD before metastasis (≥1 TIMEPOINT) Later detections = more "pure MRD" before metastasis ctDNA surveillance in high-risk HR+ breast cancer is TAKEAWAY feasible but not yet practice-changing. Best role: high-risk patients & MRD-directed trials @DrRishabhOnco
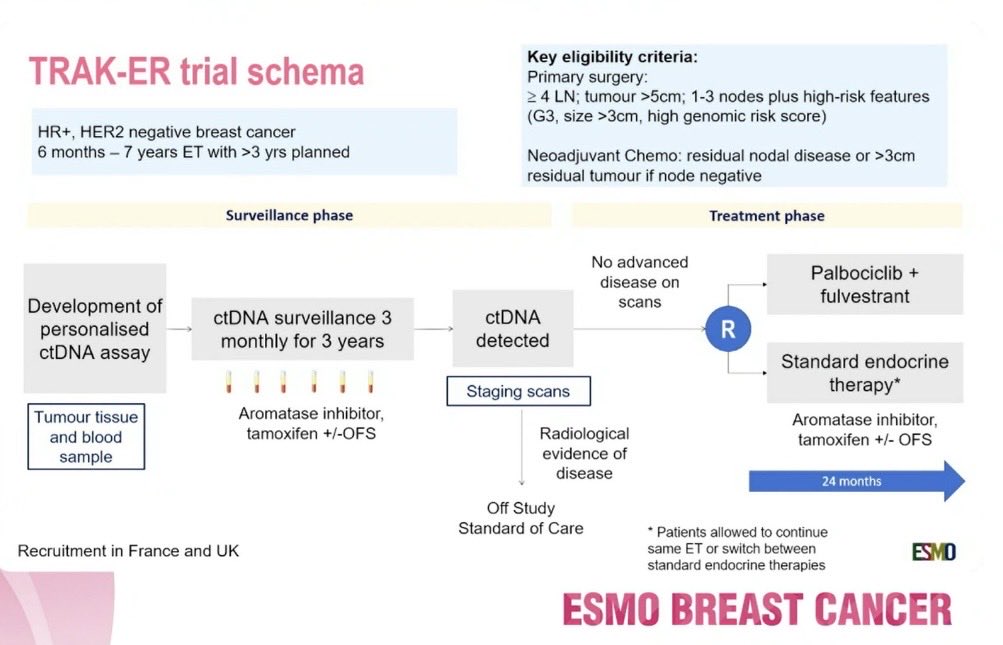


[Slide 1] TRAK-ER trial schema Key eligibility criteria: Primary surgery: ≥4 LN; tumour >5cm; 1-3 nodes plus high-risk features (G3, size >3cm, high genomic risk score) HR+, HER2 negative breast cancer 6 months - 7 years ET with >3 yrs planned Neoadjuvant Chemo: residual nodal disease or >3cm residual tumour if node negative Surveillance phase Treatment phase No advanced Palbociclib + disease on . Development of scans fulvestrant ctDNA surveillance 3 ctDNA personalised R monthly for 3 years detected ctDNA assay Standard endocrine . ...... Staging scans therapy* Tumour tissue Aromatase inhibitor, Aromatase inhibitor, and blood tamoxifen +/-OFS Radiological tamoxifen +/- OFS sample evidence of disease 24 months Off Study Standard of Care . Patients allowed to continue Recruitment in France and UK same ET or switch between ESMO standard endocrine therapies ESMO BREAST CANCER --- [Slide 2] Disease Recurrence Rate Recurrence at the Time of ctDNA Detection Overall, 42.9% of patients had recurrent No recurrence Recurrence disease at the time ctDNA detection 100%- (45/105) 15 34% 86.7% distant recurrence (39/45) 75% 45 6.7% loco-regional recurrence suitable for treatment with curative intent (3/45)1 Percentage 74% 50% 4.4% incurable locally advanced recurrence (2/45) 29 2.2% missing (1/45) 66% 25% 16 In patients detected at initial test (M0), 26% 65.9% had recurrent disease 0% Month 0 Month 3+ In patients detected in subsequent tests Timepoint ctDNA detected (M3+) 26.2% had recurrent disease Dr Niamh Cunningham 1. 2 of the patients had locally advanced curative disease and re-entered surveillance. Content of this presentation is copyright and responsibility of the author Permission IS required for TO use Both had ctDNA detected on subsequent testing. 1 had molecular relapse. MD ESMO BREAST CANCER --- [Slide 3] Conclusion In patients with higher risk ER positive HER2 negative breast cancer ctDNA detection was 1.9% per test and 11.6% per patient in serial testing In patients with initial ctDNA detection in M3+, 26.2% had recurrent disease at the time of detection ctDNA detection was more frequent with more advanced anatomical stage, higher nodal involvement and higher grade Modelling of data from TRAK-ER, highlights the importance of detecting ctDNA at low allele fractions, to identify molecular relapse prior to clinical relapse TRAK-ER demonstrates the feasibility of ctDNA surveillance and informs future trial design Dr Niamh Cunningham Content of this presentation is copynght and responsibility of the outhor Permission is required for no use ESMO ESMO BREAST CANCER




[Slide 1] ESMO BREAST CANCER BERLIN GERMANY Annial Congress 6-8 MAY 2026 ESMO How Can We Integrate New Technologies and Therapeutics to Optimize Outcomes for HR+ HER2- eBC? ctDNA detection rates during surveillance in high-risk PREcoopERA: A window of opportunity (WOO) trial of HR+/HER2 negative breast cancer from the TRAK-ER giredestrant +/- LHRH analogue vs anastrozole + LHRH in study premenopausal patients with ER+/HER2- early breast cancer Elsabetta Munzone Ruichae Shi, Vesna Bjelic-Radisic, Antonia Perefio, Roisin M Connolly Joana Mourato Ribero, Fabio Conforti, Marianna Sinco, Alba Gonzilez Haba Martinez, Eudaid Felp, Verónica Niamh Cunningham Sofia Sardo inform Claire Swift Rosalind Cutts Karen Thomas, Luisa Obadio GI, Beatriz Rajas Garoin Serafin Morales, Dagmar Langanke Johanna Frindle, Cornella Robert D. Daber, Janhua Zhao, Francois Legrand Lemmoner an MacPherson Leo Laurent Rosset Heid Roschitzki-Voser, Roswtha Kammler, Patrizia Dell'Orto Lola Russo, Clara O'Brien Carlo Palmieri, Peter Schmid Marie Robert Alca FC Okines Dymphna Barbara Rupp. Eva Grolimund Meredith Regan Marco Colleges Sherena La Peter Dutsky Lee, Isaac Garcia-Murilas, Fabrice Andre Nicholas C Turner Elisabetta Munzone European institute of Oncology, Milan, staly TRAK-ER deepens our understanding of ctDNA monitoring PREcoopERA modulates use of novel therapies in in the HR+ HER2- adjuvant setting younger patients to optimize therapeutic balance EricaL Mayer NO, MPH Content of the presentation 0 copynght and responsibility of the author Permission 6 required for no use ESMO ESMO BREAST CANCER --- [Slide 2] ESMO BREAST CANCER BERLIN GERMANY Amount Congress 6-8 MAY 2026 ESMD What Do We Know About ctDNA Detection in HR+/HER2- Early Breast Cancer? Confirmed clinical validity: Detection of ctDNA, at baseline or late adjuvant setting, is strongly prognostic for recurrence. Unconfirmed clinical utility: Does identification of molecular relapse before clinical relapse allow modulation of therapy to delay or reverse recurrence? PALLAS CHiRP Testing at baseline Testing >5 years ctDNA Negative ctDNA Negative 151 95%C 88, 260 p-value 0001 IDFS 75% of ctDNA+ with recurrence within years ctDNA Positive ctDNA Positive Time from Number Erical Mayer ND, MPH Content of this presentation copynght and responsibility of the after Purmission required for " ESMO ESMO BREAST CANCER --- [Slide 3] IESMO BREAST CANCER BERLIN GERMANY Annual Congress 6-8 MAY 2026 ESMO TRAK-ER ctDNA Detection: In Whom? When? Disease Status? Annual ctDNA Detection Rate by Year Since Surgery Recurrence by Visit Category No recurrence Recurrence 8% 7.2% 100% 6.1% 15 6% Annual ctDNA detection rate 5.6% 5.3% 5.4% 75% 34% 4.5% 45 4% 3.5% Percentage 74% 50% 29 2% 25% 66% 16 26% 0% 0% 1 2 3 4 5 6 7 Month 0 Month 3+ Year since surgery Visit category Rate of detection consistent over 7 years after surgery, echoes known persistent recurrence rate for HR+ disease Detection associated with higher disease burden Concurrent disease recurrence more likely when ctDNA+ at baseline, with higher allele fraction EricaL Mayer NO, MPH Content of the presentation in copyright and responsibility of the author Permission . required for no use ESMO ESMO BREAST CANCER --- [Slide 4] ESMO BREAST CANCER BERLIN GERMANY 6-8 MAY 2026 ESMO CONCLUSIONS: PREcoopERA What We Know What We're Waiting For Are We There Yet? Preoperative giredestrant +/- OFS leads Larger experiences with prolonged Until further data are available, oral to substantial antiproliferative effect, SERD monotherapy in premenopausal SERDs should only be used with greater with OFS patients may clarify efficacy, safety, and OFS in premenopausal patients. PREcoopERA aligns with other studies in any preferred population this setting, showing activity but unable Novel combinations and novel to confirm equivalence of SERD alone. biomarkers are needed Toxicity concerns about estradiol levels without ovarian suppression WAIT EricaL Mayer MD, MPH Content of the presentation a copyright and responsibility of the author Permission . required for to use ESMO ESMO BREAST CANCER




[Slide 1] ESMO BREAST CANCER BERLIN GERMANY Annual Congress 6-8 MAY 2026 ESMO 2026 ESMO BREAST CANCER PRINTRIENT LINES Annual Congress ctDNA detection rates during surveillance in high-risk HR+/HER2 negative breast cancer from the TRAK-ER study Niamh Cunningham Sofia Sardo Infirm, Claire Swift, Rosalind J Cutts, Karen Thomas, Robert D. Daber, Jianhua Zhao, Francois Legrand, Jerome Lemonnier, lain MacPherson, Ciara Brien, Carlo Palmieri, Peter Schmid. Marie Robert, Alicia FC Okines, Dymphna Lee. Isaac Garcia-Murillas, Fabrice Andre. Nicholas C Turner 06 May 2026 ESMO ESMO BREAST CANCER --- [Slide 2] ESMO BREAST CANCER BERLIN GERMANY Annual Congress 6-8 MAY 2026 ESMO TRAK-ER trial schema Key eligibility criteria: Primary surgery: ≥4 LN; tumour >5cm; 1-3 nodes plus high-risk features (G3, size >3cm, high genomic risk score) HR+, HER2 negative breast cancer 6 months - 7 years ET with >3 yrs planned Neoadjuvant Chemo: residual nodal disease or >3cm residual tumour if node negative Surveillance phase Treatment phase No advanced Palbociclib + disease on scans fulvestrant Development of ctDNA surveillance 3 ctDNA personalised R monthly for 3 years detected ctDNA assay Standard endocrine Staging scans therapy* Tumour tissue Aromatase inhibitor, Aromatase inhibitor, and blood tamoxifen +/-OFS Radiological tamoxifen +/- OFS sample evidence of disease 24 months Off Study Standard of Care . Patients allowed to continue Recruitment in France and UK same ET or switch between ESMO standard endocrine therapies ESMO BREAST CANCER --- [Slide 3] Disease Recurrence Rate Recurrence at the Time of ctDNA Detection Overall, 42.9% of patients had recurrent No recurrence Recurrence disease at the time ctDNA detection 100% (45/105) 15 34% 86.7% distant recurrence (39/45) 75% 45 6.7% loco-regional recurrence suitable for treatment with curative intent (3/45)1 Percentage 74% 50% 4.4% incurable locally advanced recurrence (2/45) 29 2.2% missing (1/45) 66% 25% 16 In patients detected at initial test (M0), 26% 65.9% had recurrent disease 0% Month 0 Month 3+ In patients detected in subsequent tests Timepoint ctDNA detected (M3+) 26.2% had recurrent disease Dr Niamh Cunningham 1. 2 of the patients had locally advanced curative disease and re-entered surveillance Content of this presentation is copyright and responsibility of the author Permission is required for no USA Both had ctDNA detected on subsequent testing 1 had molecular relapse ESMO ESMO BREAST CANCER --- [Slide 4] ESMO BREAST CANCER BERLIN GERMANY Annual Congress 6-8 MAY 2026 ESMO Conclusion In patients with higher risk ER positive HER2 negative breast cancer ctDNA detection was 1.9% per test and 11.6% per patient in serial testing In patients with initial ctDNA detection in M3+, 26.2% had recurrent disease at the time of detection ctDNA detection was more frequent with more advanced anatomical stage, higher nodal involvement and higher grade Modelling of data from TRAK-ER, highlights the importance of detecting ctDNA at low allele fractions, to identify molecular relapse prior to clinical relapse TRAK-ER demonstrates the feasibility of ctDNA surveillance and informs future trial design Dr Niamh Cunningham Content of this presentation B copyright and responsibility of the author Permission is required for no use ESMO ESMO BREAST CANCER




[Slide 1] TRAK-ER Trial Schema Key Eligibility Criteria: High Risk HR+ Node Positive HR+, HER2 negative breast cancer Primary surgery: > 4 LN; tumour >5cm; 1-3 nodes plus high-risk features (G3, size >3cm, high genomic risk score) 6 months - 7 years ET with >3 yrs planned Neoadjuvant Chemo: residual nodal disease or >3cm residual tumour if node negative Surveillance Phase Treatment Phase Development of No advanced Palbociclib + fulvestrant personalised ctDNA assay ctDNA surveillance 3 ctDNA disease on scans R Plasma Detect ID MRD WES monthly for 3 years detected tumor informed assay Standard endocrine therapy Tumour tissue IIIIII Staging scans Aromatase inhibitor, and blood sample Aromatase inhibitor, tamoxifen +/- OFS tamoxifen +/-OFS Radiological 24 months evidence of disease Primary Endpoints: Surveillance phase: ctDNA detection rates Treatment phase: RFS with palbo & fulvestrant VS standard ET in Off Study ctDNA detected patients Standard of Care Erica L Mayer MD, MPH Content of the presentation 15 copynght and responsibility of the author Permission is required for re use ESMO --- [Slide 2] ctDNA detection rate Detection Rate per Visit Month Detected Not Detected ctDNA detected in 1.9% of samples 1000 5.0% (107/5724) 1.7% 1.2% 750 1.9% ctDNA detected in 11.6% of patients 0.3% (105/901) ¹ ctDNA was detected in 5.0% of initial tests Number of Tests 2.1% 500 1.1% 1.1% 0% 250 (MO) vs 1.3% of subsequent tests (M3+) 1.5% 0% (p<0.001) 4.9% 0% 0 58.9% of ctDNA detection occurred after an 0 3 6 9 12 15 18 21 24 27 30 33 36 Visit Month initial negative test Median allele fraction: 0.02% (0.001-7.97%)² No trend in detection rates from M3+ onwards (p=0.2154) Number above bar indicates ctDNA detection rate per test 1. Two patents had ctDNA detected in 2 timepoints. Both received treatment for local recurrence Dr Niamh Cunningham and re-entered surveillance and subsequently had ctDNA detected ESMO Content of this presentation is copyright and responsibility of the author Permission IS required for 10 use 2. Weighted average variant allele frequency reported for each positive timepoint --- [Slide 3] Disease Recurrence Rate Recurrence at the Time of ctDNA Detection No recurrence Recurrence Overall, 42.9% of patients had recurrent disease at the time ctDNA detection 100%- (45/105) 15 34% 86.7% distant recurrence (39/45) 75% 45 74% 6.7% loco-regional recurrence suitable for treatment with curative intent (3/45)¹ 4.4% incurable locally advanced recurrence (2/45) Percentage 50% 29 66% 2.2% missing (1/45) 25% 16 In patients detected at initial test (M0), 26% 65.9% had recurrent disease 0% Month 0 Month 3+ In patients detected in subsequent tests Timepoint ctDNA detected (M3+) 26.2% had recurrent disease Dr Niamh Cunningham 1. 2 of the patients had locally advanced curative disease and re-entered surveillance. Content of this presentation IS copynght and responsibility of the author Permission is required for use Both had ctDNA detected on subsequent testing. 1 had molecular relapse. --- [Slide 4] Exploratory Clinical Correlation with ctDNA detection Anatomic Stage pT Stage pN Stage 30% P = 0.018 30% P 0.691 30% p<0.001 18/84 20/96 (21%) 33/206 (21%) ctDNA positive (%) 20% 16/149 ctDNA positive (%) 20% 40/338 16/143 45/376 33/270 28/287 1/11 2/28 ctDNA positive (%) 20% (16%) (12%) (11%) (12%) (12%) 37/429 (11%) (10%) (9%) 4/69 (9%) 10% (7%) 10% 10% (6%) 0% 0% 0% IIA IIB IIIA IIIB IIIC T1 T2 T3 T4 NO N1 N2 N3 Stage Pathological Tumour Status Pathological Nodal Status ctDNA detection increased with higher nodal stage and numerically more frequent in stage IIIC tumours Dr Niamh Cunningham Content of this presentation is copyright and responsibility of the author Permission is required for re use *Statistical testing: Exploratory time-to-event analyses accounting for delayed study entry. ESMO



[Slide 1] 2026 ESMO BREAST CANCER Annual Congress ctDNA detection rates during surveillance in high-risk HR+/HER2 negative breast cancer from the TRAK-ER study Niamh Cunningham, Sofia Sardo Infirri, Claire Swift, Rosalind J Cutts, Karen Thomas, Robert D. Daber, Jianhua Zhao, Francois Legrand, Jerome Lemonnier, lain MacPherson, Ciara O'Brien, Carlo Palmien, Peter Schmid, Marie Robert, Alicia FC Okines, Dymphna Lee, Isaac Garcia-Murillas, Fabrice Andre, Nicholas C Tumer 06 May 2026 --- [Slide 2] TRAK-ER trial schema Key eligibility criteria: Primary surgery: ≥4 LN; tumour >5cm; 1-3 nodes plus high-risk features (G3, size >3cm, high genomic risk score) HR+, HER2 negative breast cancer 6 months - 7 years ET with >3 yrs planned Neoadjuvant Chemo: residual nodal disease or >3cm residual tumour if node negative Surveillance phase Treatment phase No advanced Palbociclib + disease on Development of scans fulvestrant ctDNA surveillance 3 ctDNA personalised R monthly for 3 years detected ctDNA assay Standard endocrine Staging scans therapy* Tumour tissue Aromatase inhibitor, Aromatase inhibitor, and blood tamoxifen +/-OFS Radiological tamoxifen +/- OFS sample evidence of disease 24 months Off Study Standard of Care * Patients allowed to continue Recruitment in France and UK same ET or switch between ESMO standard endocrine therapies --- [Slide 3] ctDNA detection rate Detection Rate per Visit Month Detected Not Detected ctDNA detected in 1.9% of samples 1000 5.0% (107/5724) 1.7% 1.2% 750 ctDNA detected in 11.6% of patients 1.9% (105/901) ¹ Number of Tests 0.3% 2.1% 500 1.1% ctDNA was detected in 5.0% of initial tests 1.1% 0% (MO) VS 1.3% of subsequent tests (M3+) 250 1.5% (p<0.001) 0% 4.9% 0% 0 58.9% of ctDNA detection occurred after an 0 3 6 9 12 15 18 21 24 27 30 33 36 initial negative test Visit Month Median allele fraction: 0.02% (0.001-7.97%)² No trend in detection rates from M3+ onwards (p=0.2154) Number above bar indicates ctDNA detection rate per test 1. Two patents had ctDNA detected in 2 timepoints. Both received treatment for local recurrence Dr Niamh Cunningham and re-entered surveillance and subsequently had ctDNA detected Content of this presentation is copyright and responsibility of the author Permission is required for re-use 2. Weighted average variant allele frequency reported for each positive timepoint MD --- [Slide 4] Disease Recurrence Rate Recurrence at the Time of ctDNA Detection Overall, 42.9% of patients had recurrent No recurrence Recurrence disease at the time ctDNA detection 100% (45/105) 15 34% 86.7% distant recurrence (39/45) 75% 45 6.7% loco-regional recurrence suitable for treatment with curative intent (3/45)1 Percentage 74% 50% 4.4% incurable locally advanced recurrence (2/45) 29 2.2% missing (1/45) 66% 25% 16 In patients detected at initial test (MO), 26% 65.9% had recurrent disease 0% Month 0 Month 3+ In patients detected in subsequent tests Timepoint ctDNA detected (M3+) 26.2% had recurrent disease Dr Niamh Cunningham 1. 2 of the patients had locally advanced curative disease and re-entered surveillance. Content of this presentation is copyright and responsibility of the author Permission is required for re-use Both had ctDNA detected on subsequent testing. 1 had molecular relapse. ESMD


Highest-engagement tweets about this trial, ranked by KOL discussant count (replies + quote-tweets). Replies in green, quote-tweets in blue. Wall Street, stock-promo, and non-substantive replies excluded.
ctDNA surveillance in HR+ breast cancer is promising… but here’s the reality 👇 #ESMOBreast26 🧬 TRAK-ER study 👥 High-risk HR+ / HER2- on adjuvant ET ⚡ Strategy: Serial ctDNA → detect relapse BEFORE imaging 📊 Key findings: • Detection per test: just 2.6% • 11.3% pts https://t.







 +2
+2
Dr. Erica Mayer (@elmayermd) delivered an excellent discussion of the TRAK-ER and PREcoopERA trials at #ESMOBreast26. https://t.co/E8IQiBXcdB
Can ctDNA detect relapse before scans? 👀 #ESMOBreast26 TRAK-ER evaluated serial ctDNA surveillance in high-risk HR+/HER2- EBC. 🧬 ctDNA+ at first test (M0): • 65.9% already had recurrence 🧬 ctDNA+ later (M3+): • Only 26.2% had recurrence → Potential molecular lead-time https://
TRAK-ER Trial: Serial ctDNA Monitoring Uncovers Subclinical Relapse with Significant Lead-Time Advantage in High Risk HR+/HER2− Breast Cancer Moving from Radiologic Detection to Molecular Intervention @OncoAlert #ESMOBreast26 #bcsm #BreastCancer https://t.co/xRiz8DUXSb
#ESMOBreast26 In TRAK-ER, ctDNA positivity appeared to be associated more with nodal burden than with pT stage. At the time of ctDNA detection, 42.9% of patients already had recurrent disease; among those detected during M3+ surveillance, this rate decreased to 26.2%. ctDNA ht
TRAK-ER is a UK-led randomized multicentre study evaluating serial circulating tumor DNA (ctDNA) surveillance every 3 months for 3 years in patients with high-risk HR+/HER2- early breast cancer receiving adjuvant endocrine therapy. The primary aim is to detect molecular relapse before clinical or radiographic progression and randomize ctDNA-positive patients to palbociclib + fulvestrant vs. continued standard endocrine therapy. The interim surveillance analysis presented at ESMO Breast 2026 reports detection rates and clinical correlates from the first 480 patients with successful panel design.
Population: Patients with high-risk early-stage ER+/HER2- breast cancer (Allred 6/8+ ER, IHC 0/1+ HER2 or ISH-negative). High-risk defined by nodal status, tumour size >3 cm, grade 3, or high genomic risk (Oncotype DX RS≥26, Prosigna ≥60, EPclin ≥4.0, MammaPrint high). Currently 901 patients with successful panel design have started surveillance.
Interventions: Surveillance phase: tumour-informed ctDNA assay every 3 months. Treatment phase (post-randomization for ctDNA+ patients): palbociclib 125 mg/day 3 wks on/1 wk off + fulvestrant 500 mg IM monthly vs continued standard endocrine therapy.
Endpoints: Surveillance phase: ctDNA detection rate, lead time to clinical relapse, association with clinicopathologic features. Treatment phase primary: relapse-free survival.
Across 2,110 samples from 480 patients, ctDNA was detected in 2.6% of tests; 11.3% of patients had ctDNA detected at least once. Detection was higher at the first surveillance timepoint (Month 0: 6.2%) than later samples (Month 3+: 1.5%; p<0.0001). 42.9% of patients had concurrent metastatic disease at the time of initial ctDNA detection (65.9% at M0, 26.2% at M3+). Median allele fraction was 0.034%. Detection was numerically more frequent in higher-stage and node-positive disease. Annual detection rates declined over time: 7.6% Y1, 2.9% Y2-3, 1.8% Y4, 2.0% beyond Y7.
The interim surveillance analysis is observational — no treatment exposure. Panel design failed in 14.8-16.1% of patients (insufficient tumour material or detectable variants), highlighting need for more sensitive tumour-agnostic assays. Treatment phase safety (palbo + fulvestrant) is consistent with established profiles for those agents.
Rishabh Jain framed TRAK-ER as “ctDNA surveillance in HR+ breast cancer is promising… but here’s the reality,” noting “Detection per test: just 2.6%” and that detection “declines over time.” In a follow-up post he pressed the lead-time question: “ctDNA+ at first test (M0): 65.9% already had recurrence; ctDNA+ later (M3+): Only 26.2% had recurrence.” Yakup Ergün flagged that “ctDNA positivity appeared to be associated more with nodal burden than with pT stage,” and that “at the time of ctDNA detection, 42.9% of patients already had recurrent disease.” Aya Mohamed described the result as “Serial ctDNA Monitoring Uncovers Subclinical Relapse with Significant Lead-Time Advantage in High Risk HR+/HER2− Breast Cancer Moving from Radiologic Detection to Molecular Intervention.” Dana-Farber’s Breast Oncology Center noted that Erica Mayer “delivered an excellent discussion of the TRAK-ER and PREcoopERA trials,” setting up the open question of whether ctDNA-guided intervention can translate signal into outcome.
TRAK-ER (NCT04985266) is a Phase 2, investigator-initiated trial run by The Royal Marsden and the Institute of Cancer Research (with NIHR support). It uses serial circulating-tumor-DNA (ctDNA) surveillance to detect molecular residual disease in high-risk HR-positive/HER2-negative early breast cancer and tests whether an early switch to fulvestrant plus palbociclib - triggered before overt clinical relapse - can improve outcomes.
In the surveillance interim analysis, across 2,110 samples from 480 patients, ctDNA was detected in 2.6% of individual tests and 11.3% of patients had ctDNA detected at least once, with the highest detection at the first surveillance timepoint. Importantly, 42.9% of ctDNA-positive patients already had concurrent radiological recurrence at detection, which informs how much lead time ctDNA surveillance actually provides.
No. TRAK-ER tests an investigational ctDNA-guided early-switch strategy in early breast cancer. Fulvestrant (Faslodex) and palbociclib (Ibrance) are separately FDA-approved in metastatic HR-positive/HER2-negative breast cancer, but using ctDNA surveillance to trigger an early switch to this combination in the early/adjuvant setting is investigational and not FDA approved.
The interim data are nuanced: while ctDNA identified molecular residual disease in a meaningful subset of patients, 42.9% of ctDNA-positive patients already had concurrent radiological recurrence at the time of detection, meaning the anticipated lead time was smaller than hoped for many patients. This tempers expectations about how far in advance current ctDNA surveillance can trigger a pre-emptive treatment switch.
The interim surveillance analysis is observational (no treatment exposure yet), and the personalized ctDNA panel design failed in roughly 15-16% of patients because of insufficient tumor material or a lack of trackable variants. These assay-performance and lead-time findings are important for designing future ctDNA-guided intervention trials in early breast cancer.
| Handle | Name | Sentiment | Tweet (excerpt) | Imp. |
|---|---|---|---|---|
| @DrRishabhOnco | Dr Rishabh Jain | Neutral | ctDNA surveillance in HR+ breast cancer is promising… but here’s the reality 👇 #ESMOBreast26 🧬 TRAK-ER study 👥 High-r… | 4,210 |
| @DrRishabhOnco | Dr Rishabh Jain | Neutral | Can ctDNA detect relapse before scans? 👀 #ESMOBreast26 TRAK-ER evaluated serial ctDNA surveillance in high-risk HR+/HER… | 2,251 |
| @DFCI_BreastOnc | Dana-Farber’s Breast Oncology Center | Neutral | Dr. Erica Mayer (@elmayermd) delivered an excellent discussion of the TRAK-ER and PREcoopERA trials at #ESMOBreast26. ht… | 785 |
| @dr_yakupergun | Yakup Ergün | Neutral | #ESMOBreast26 In TRAK-ER, ctDNA positivity appeared to be associated more with nodal burden than with pT stage. At the… | 764 |
















