DAVA Hawaii Lung Summit · Kona, Hawaii · Jul 8–11, 2026
DAVA Hawaii Lung 2026 Slide Intelligence
A focused thoracic-oncology summit, fully distilled: 126 presented slide talks from 35 faculty across eight therapeutic themes — every data slide OCR-transcribed and 141+ named trials tagged. EGFR, KRAS/RAS, HER2, next-generation ADCs, small cell, fusion drivers, radiation & theranostics, and IO/perioperative strategy. Curated by KOL Pulse from the live #DAVALung feed.
126
Slide Talks
476
Slides OCR'd
35
Faculty
141
Trials Tagged
Faculty & Speakers
The Voices at DAVA Hawaii Lung 2026
Every faculty speaker, grouped by the theme they presented most, with their X and institutional profiles and the trials & topics they covered at the summit.
Create a free account, pick the tumor types you cover, and go beyond the tweet — the intelligence pharma teams use to map influence and prepare for engagement:
NORTHSTAR surgical update: @maraantonoff, @UTMDAnderson reports lung resection after Osi in EGFR-mutant stage IV NSCLC was safe, median LOS 3 days, 9.5% pCR & PFS endpoint met. Study explores:
Which patients benefit?
When should we operate?
What can surgery teach us? #DAVALung
[Slide 1]
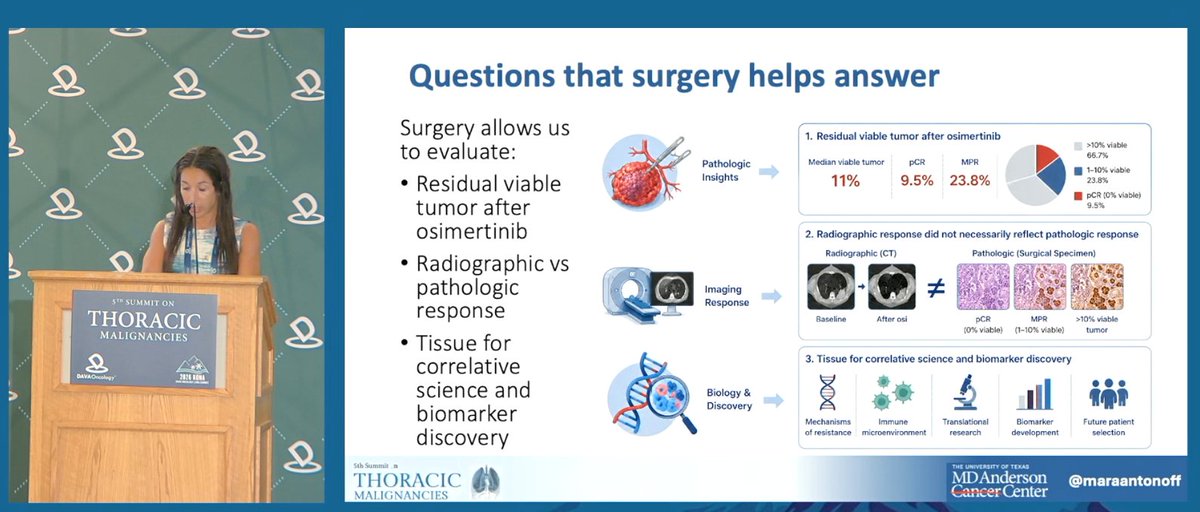
Questions that surgery helps answer
Surgery allows us to evaluate:
- Residual viable tumor after osimertinib
- Radiographic vs pathologic response
- Tissue for correlative science and biomarker discovery
1. Residual viable tumor after osimertinib (Pathologic Insights): Median viable tumor 11% | pCR 9.5% | MPR 23.8%. Pie chart: >10% viable 66.7%; 1-10% viable 23.8%; pCR (0% viable) 9.5%.
2. Radiographic response did not necessarily reflect pathologic response (Imaging Response): Radiographic (CT) Baseline -> After osi ≠ Pathologic (Surgical Specimen) pCR (0% viable) / MPR (1-10% viable) / >10% viable tumor.
3. Tissue for correlative science and biomarker discovery (Biology & Discovery): Mechanisms of resistance, Immune microenvironment, Translational research, Biomarker development, Future patient selection.
Footer: @maraantonoff, MD Anderson Cancer Center
———
[Slide 2]
Lung resection after osimertinib was safe
- LOS 3 days (1-6)
- Complications infrequent
- 1 (4.8%) pneumonitis
- 2 (9.5%) tachyarrhythmia
- No ICU admissions, reoperations, or deaths
Length of Stay: 3 days (1-6)
ICU Utilization: 0 patients
30-Day Complications: 14.3% (3 patients) [1 (4.8%) pneumonitis; 2 (9.5%) tachyarrhythmia]
90-Day Outcomes: 0% Mortality / Reoperations / Readmissions
Surgery after induction osimertinib is feasible with low morbidity and no perioperative mortality.
Source: Antonoff MB STS 2026. Footer: @maraantonoff, MD Anderson Cancer Center
———
[Slide 3]
Response to therapy may matter more than baseline disease burden
Nodal clearance after osimertinib predicts LCT benefit
- Thoracic Nodes Present at Randomization PFS: Osi + LCT median PFS = 19.0 mo (95% CI 12.6-23.2); Osi alone median PFS = 15.9 mo (95% CI 10.9-23.9); HR 0.92, 90% CI 0.60-1.43, p = 0.388
- Thoracic Nodes Absent at Randomization PFS: Osi + LCT median PFS = 41.5 mo (95% CI 31.2-NA); Osi alone median PFS = 19.6 mo (95% CI 9.1-31.5); HR 0.43, 90% CI 0.23-0.78, p = 0.008
Effusion clearance after osimertinib predicts LCT benefit
- Pleural Effusion Present at Randomization PFS: Osi + LCT median PFS = 15.3 mo (95% CI 11.6-23.9); Osi alone median PFS = 12.9 mo (95% CI 8.5-20.9); HR 0.90, 90% CI 0.52-1.55, p = 0.373
- Pleural Effusion Absent at Randomization PFS: Osi + LCT median PFS = 32.7 mo (95% CI 19.7-48.2); Osi alone median PFS = 22.3 mo (95% CI 14.5-28.1); HR 0.63, 90% CI 0.39-1.02, p = 0.057
Source: Gandhi S et al, ELCC 2026. Footer: @maraantonoff, MD Anderson Cancer Center
———
[Slide 4]
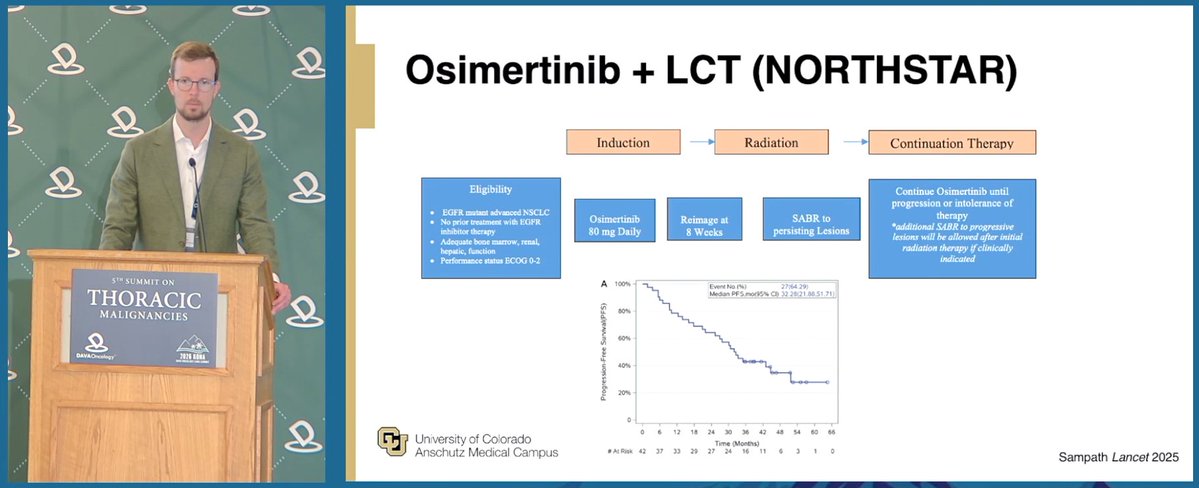
Why NORTHSTAR was needed
THE CHALLENGE: Osimertinib transforms outcomes, but resistance is inevitable. (Tumor Burden vs Time: Response then Progression, Resistant clones emerge.) Virtually all EGFR-mutant patients eventually develop resistance.
THE EVIDENCE (BEFORE NORTHSTAR): Retrospective studies suggested benefit from local consolidative therapy (LCT). Improved Progression-Free Survival; Improved Overall Survival; Delayed Time to New Metastases; Potential for Cure in a Subset. However, prospective randomized evidence was lacking.
-> Could LCT delay progression in EGFR-mutant NSCLC?
Source: Gomez DR et al, J Clin Oncol 2019; Iyengar P et al, JAMA Oncol. 2018.
Dr. @matt_cw_lee@cityofhope discusses how EGFR exon 20 insertion location can influence TKI response, classical EGFR alterations, exon 20 insertions, PACC mutations, T790M-like changes and compound mutations each point toward distinct therapeutic strategies. #DAVALung
ZENITH20
[Slide 1]
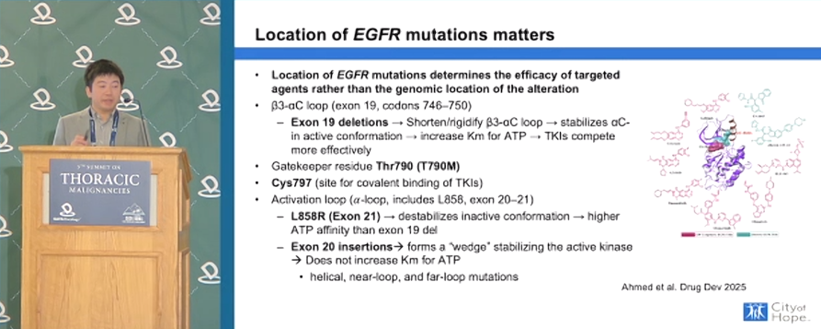
Location of EGFR mutations matters
- Location of EGFR mutations determines the efficacy of targeted agents rather than the genomic location of the alteration
- b3-aC loop (exon 19, codons 746-750)
- Exon 19 deletions -> Shorten/rigidify b3-aC loop -> stabilizes aC- in active conformation -> increase Km for ATP -> TKIs compete more effectively
- Gatekeeper residue Thr790 (T790M)
- Cys797 (site for covalent binding of TKIs)
- Activation loop (a-loop, includes L858, exon 20-21)
- L858R (Exon 21) -> destabilizes inactive conformation -> higher ATP affinity than exon 19 del
- Exon 20 insertions -> forms a "wedge" stabilizing the active kinase -> Does not increase Km for ATP
- helical, near-loop, and far-loop mutations
Ahmed et al. Drug Dev 2025
———
[Slide 2]
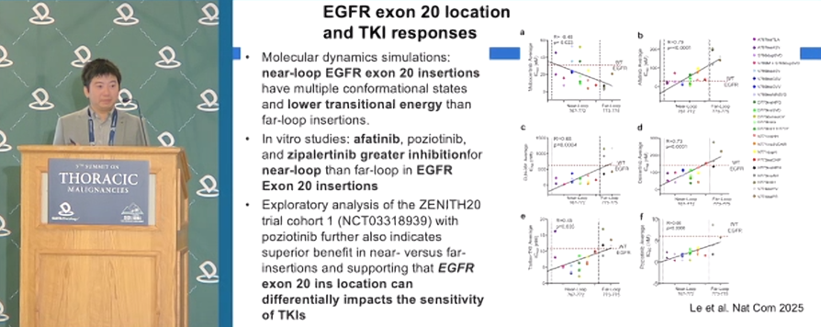
EGFR exon 20 location and TKI responses
- Molecular dynamics simulations: near-loop EGFR exon 20 insertions have multiple conformational states and lower transitional energy than far-loop insertions.
- In vitro studies: afatinib, poziotinib, and zipalertinib greater inhibition for near-loop than far-loop in EGFR Exon 20 insertions
- Exploratory analysis of the ZENITH20 trial cohort 1 (NCT03318939) with poziotinib further also indicates superior benefit in near- versus far-insertions and supporting that EGFR exon 20 ins location can differentially impacts the sensitivity of TKIs
Le et al. Nat Com 2025
———
[Slide 3]
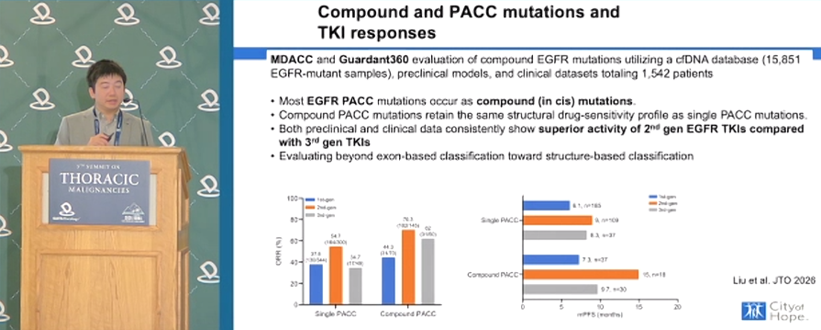
Compound and PACC mutations and TKI responses
MDACC and Guardant360 evaluation of compound EGFR mutations utilizing a cfDNA database (15,851 EGFR-mutant samples), preclinical models, and clinical datasets totaling 1,542 patients.
- Most EGFR PACC mutations occur as compound (in cis) mutations.
- Compound PACC mutations retain the same structural drug-sensitivity profile as single PACC mutations.
- Both preclinical and clinical data consistently show superior activity of 2nd gen EGFR TKIs compared with 3rd gen TKIs
- Evaluating beyond exon-based classification toward structure-based classification
ORR (%): Single PACC 1st-gen 37.5 (n=104/344), 2nd-gen 54.1 (n=71/148); Compound PACC 1st-gen 44.2 (n=147/x), 2nd-gen 76.3 (n=182/145), 3rd-gen 62 (n=x/x)
mPFS (months): Single PACC 1st-gen 6.1 (n=185), 2nd-gen 9, 3rd-gen 8.3 (n=37); Compound PACC 1st-gen 7.3 (n=37), 2nd-gen 15 (n=18), 3rd-gen 9.7 (n=30)
Liu et al. JTO 2026
———
[Slide 4]
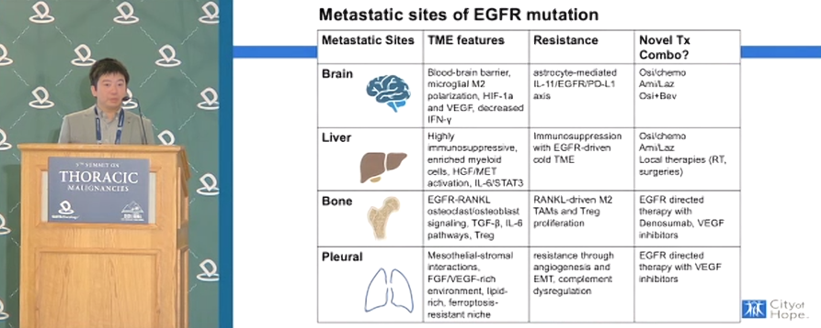
Metastatic sites of EGFR mutation
Metastatic Sites | TME features | Resistance | Novel Tx Combo?
Brain | Blood-brain barrier, microglial M2 polarization, HIF-1a and VEGF, decreased IFN-y | astrocyte-mediated IL-11/EGFR/PD-L1 axis | Osi/chemo, Ami/Laz, Osi+Bev
Liver | Highly immunosuppressive, enriched myeloid cells, HGF/MET activation, IL-6/STAT3 | Immunosuppression with EGFR-driven cold TME | Osi/chemo, Ami/Laz, Local therapies (RT, surgeries)
Bone | EGFR-RANKL osteoclast/osteoblast signaling, TGF-b, IL-6 pathways, Treg | RANKL-driven M2 TAMs and Treg proliferation | EGFR directed therapy with Denosumab, VEGF inhibitors
Pleural | Mesothelial-stromal interactions, FGF/VEGF-rich environment, lipid-rich, ferroptosis-resistant niche | resistance through angiogenesis and EMT, complement dysregulation | EGFR directed therapy with VEGF inhibitors
Amazing life story told by a dear colleague, Dr. Ravi Salgia from City of Hope as opening of the Hawaii Lung Cancer Summit! His discovery of MET- mutation is only a part of a remarkable story of family, science and resilience !
Dr. @UrsWeberMD@CUCancerCenter on consolidation in EGFR-mutant metastatic NSCLC: targeting drug-tolerant persister cells for deeper disease control with strategies such as osimertinib + chemo, osimertinib + amivantamab, and sequential osimertinib + LCT. #DAVALung
[Slide 1]
Drug-Tolerant Persister Cells
- Osimertinib will significantly reduce the burden of disease in most patients but is unable to eradicate all cancer cells.
- The remaining cancer cells generally become quiescent for months to years until they develop treatment resistance and begin to proliferate again.
- The goal of consolidation treatment is to eliminate as many of these DTPs as possible.
[Schematic] Initially sensitive tumour -> DTPs/minimal residual disease -> Phenotype switching and epigenetic resistance -> Tumour relapse; Genetic resistance.
Strategy 1: eradication of pre-DTPs and sensitive cells with combinatorial approaches (Drug 1: Targeting vulnerabilities of pre-DTPs; Drug 2: Targeting sensitive cancer cells).
Strategy 2: targeting DTPs with sequential treatment (Drug 1: Targeting sensitive cancer cells; Emergence of DTPs; Drug 2: Targeting the intrinsic vulnerabilities of DTPs / the microenvironment of DTPs / the products and availability of DTPs).
University of Colorado Anschutz Medical Campus.
Russo Nature Reviews Cancer 2024
———
[Slide 2]
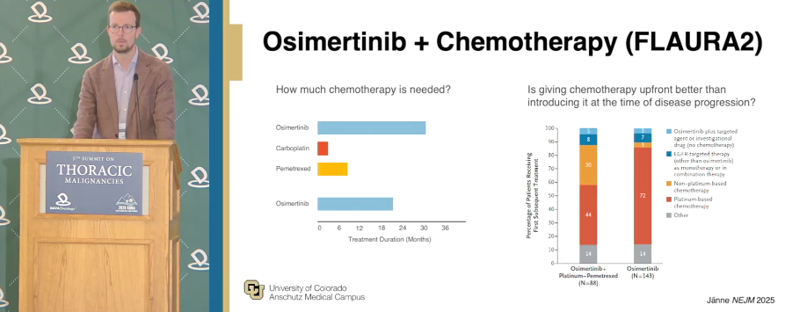
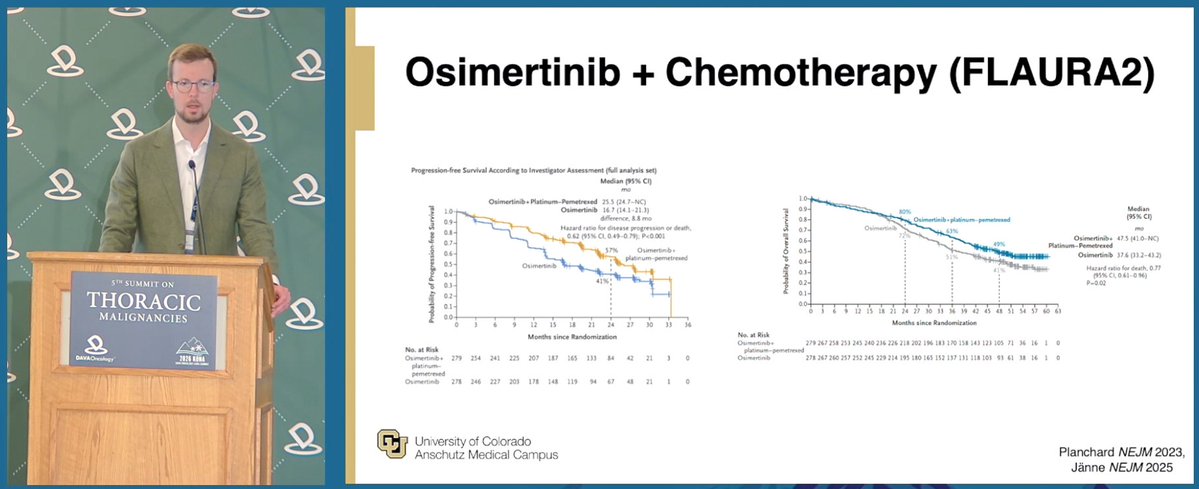
Osimertinib + Chemotherapy (FLAURA2)
How much chemotherapy is needed? [Bar chart of Treatment Duration (Months): Osimertinib ~30+; Carboplatin ~12; Pemetrexed ~15; Osimertinib ~30+]
Is giving chemotherapy upfront better than introducing it at the time of disease progression? [Stacked bar chart - Percentage of Patients Receiving First Subsequent Treatment]
Osimertinib + Platinum-Pemetrexed (N=88): Osimertinib plus targeted agent or investigational drug (no chemotherapy) 8; EGFR-targeted therapy (other than osimertinib) as monotherapy or in combination therapy 35; Non-platinum-based chemotherapy 44; Platinum-based chemotherapy; Other <4.
Osimertinib (N=143): 7; 20; 72; Other <4.
Janne NEJM 2025
———
[Slide 3]
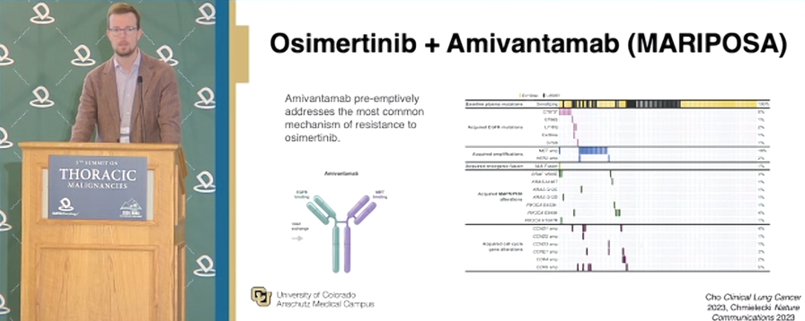
Osimertinib + Amivantamab (MARIPOSA)
Amivantamab pre-emptively addresses the most common mechanism of resistance to osimertinib.
[Antibody diagram: Amivantamab - EGFR binding / MET binding; Fc]
[Oncoprint / co-mutation plot of baseline plasma mutations 100%; acquired EGFR mutations (C797X, ...); acquired amplifications (MET amp, HER2 amp); acquired mesenchymal fusion (NLR7 fusion, ...); acquired MAPK/K alterations (BRAF V600E, KRAS amp, KRAS G12D, NRAS G12D, PIK3CA E545K, PIK3CA E542K); acquired cell cycle gene alterations (CCND1 amp, CCND2 amp, CCND3 amp, CDK6 amp, CCNE1 amp)]
University of Colorado Anschutz Medical Campus.
Cho Clinical Lung Cancer 2023, Chmielecki Nature Communications 2023
Practical #DAVALung update from @Jsabari@nyulangone: amivantamab's EGFR/MET targeting is paired with strategies to improve tolerability - SKIPPirr dex prophylaxis, SC dosing to reduce IRRs, COCOON dermatologic care, and VTE prophylaxis with ami+laz.
COCOONCOPERNICUS
[Slide 1]
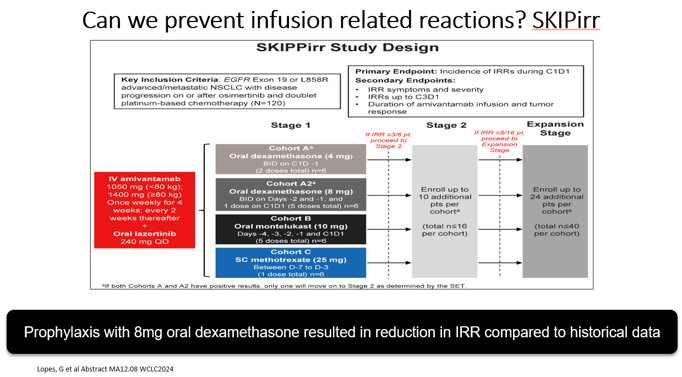
Can we prevent infusion related reactions? SKIPirr
SKIPPirr Study Design
Key Inclusion Criteria: EGFR Exon 19 or L858R advanced/metastatic NSCLC with disease progression on or after osimertinib and doublet platinum-based chemotherapy (N=120)
Primary Endpoint: Incidence of IRRs during C1D1
Secondary Endpoints: IRR symptoms and severity; IRRs up to C3D1; Duration of amivantamab infusion and tumor response
Stage 1 / Stage 2 / Expansion Stage
IV amivantamab 1050 mg (<80 kg), 1400 mg (>=80 kg) Once weekly for 4 weeks; every 2 weeks thereafter + Oral lazertinib 240 mg QD
Cohort A*: Oral dexamethasone (4 mg) BID on C1D1 (2 doses total) n=6
Cohort A2*: Oral dexamethasone (8 mg) BID on Days 2 and -1, and 1 dose on C1D1 (5 doses total) n=6
Cohort B: Oral montelukast (10 mg) Days -4, -3, -2, -1 and C1D1 (5 doses total) n=6
Cohort C: SC methotrexate (25 mg) Between D-7 to D-3 (1 dose total) n=6
If IRR <=3/6 pt, proceed to Stage 2: Enroll up to 10 additional pts per cohort (total n<=16 per cohort)
If IRR <=8/16 pt, proceed to Expansion Stage: Enroll up to 24 additional pts per cohort (total n<=40 per cohort)
*If both Cohorts A and A2 have positive results, only one will move on to Stage 2 as determined by the SET.
Prophylaxis with 8mg oral dexamethasone resulted in reduction in IRR compared to historical data
Lopes, G et al Abstract MA12.08 WCLC2024
———
[Slide 2]
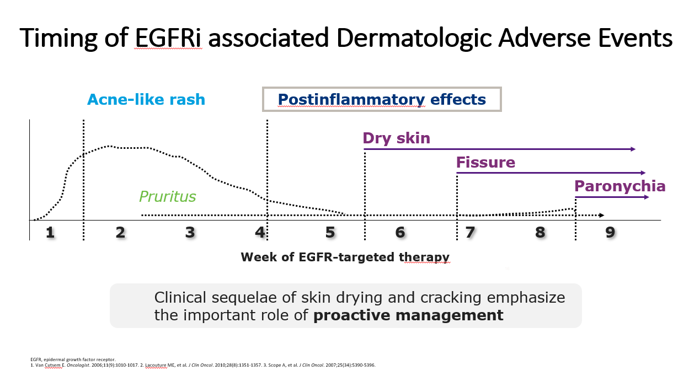
Timing of EGFRi associated Dermatologic Adverse Events
Acne-like rash
Postinflammatory effects
Pruritus
Dry skin
Fissure
Paronychia
Week of EGFR-targeted therapy (1-9)
Clinical sequelae of skin drying and cracking emphasize the important role of proactive management
EGFR, epidermal growth factor receptor. 1. Van Cutsem E. Oncologist. 2006;11(9):1010-1017. 2. Lacouture ME, et al. J Clin Oncol. 2010;28(8):1351-1357. 3. Scope A, et al. J Clin Oncol. 2007;25(34):5390-5396.
———
[Slide 3]
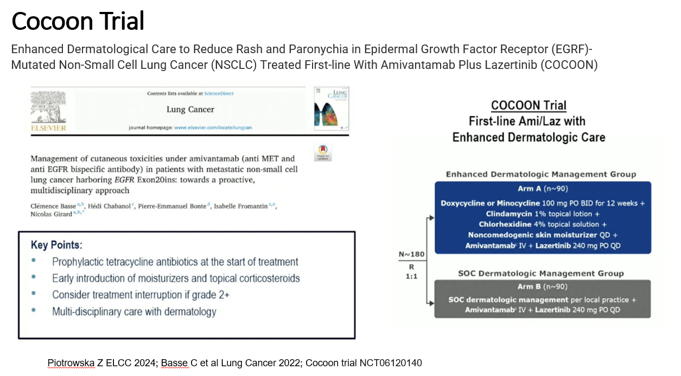
Cocoon Trial
Enhanced Dermatological Care to Reduce Rash and Paronychia in Epidermal Growth Factor Receptor (EGFR)-Mutated Non-Small Cell Lung Cancer (NSCLC) Treated First-line With Amivantamab Plus Lazertinib (COCOON)
Lung Cancer
Management of cutaneous toxicities under amivantamab (anti MET and anti EGFR bispecific antibody) in patients with metastatic non-small cell lung cancer harboring EGFR Exon20ins: towards a proactive, multidisciplinary approach
Clemence Basse, Heidi Chahanoi, Pierre-Emmanuel Bonte, Isabelle Fromantin, Nicolas Girard
Key Points:
- Prophylactic tetracycline antibiotics at the start of treatment
- Early introduction of moisturizers and topical corticosteroids
- Consider treatment interruption if grade 2+
- Multi-disciplinary care with dermatology
COCOON Trial First-line Ami/Laz with Enhanced Dermatologic Care
N~180 R 1:1
Enhanced Dermatological Management Group Arm A (n~90): Doxycycline or Minocycline 100 mg PO BID for 12 weeks + Clindamycin 1% topical lotion + Chlorhexidine 4% topical solution + Noncomedogenic skin moisturizer QD + Amivantamab IV + Lazertinib 240 mg PO QD
SOC Dermatological Management Group Arm B (n~90): SOC dermatologic management per local practice + Amivantamab IV + Lazertinib 240 mg PO QD
Piotrowska Z ELCC 2024; Basse C et al Lung Cancer 2022; Cocoon trial NCT06120140
———
[Slide 4]
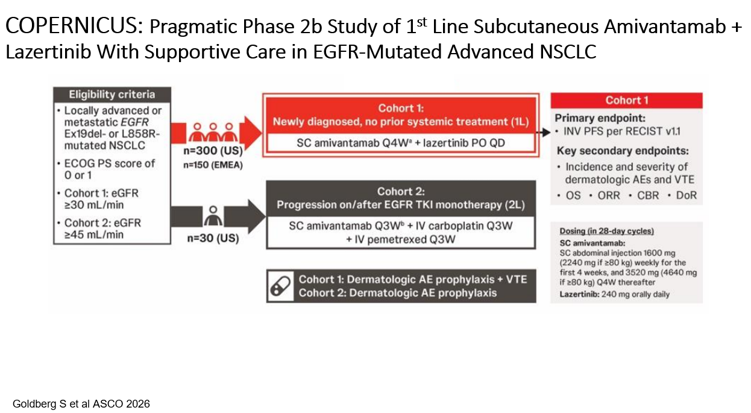
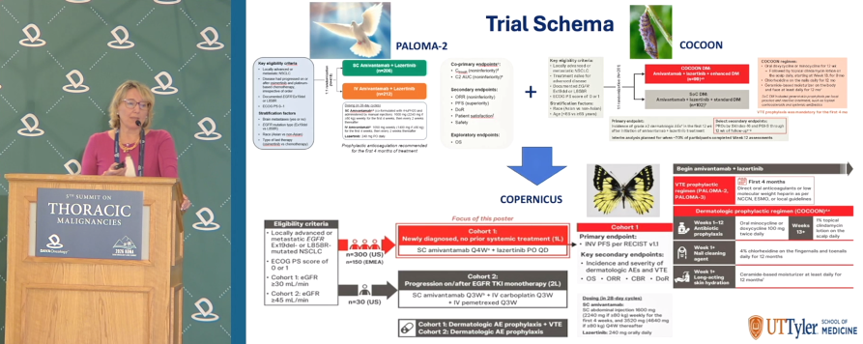
COPERNICUS: Pragmatic Phase 2b Study of 1st Line Subcutaneous Amivantamab + Lazertinib With Supportive Care in EGFR-Mutated Advanced NSCLC
Eligibility criteria:
- Locally advanced or metastatic EGFR Ex19del- or L858R-mutated NSCLC
- ECOG PS score of 0 or 1
- Cohort 1: eGFR >=30 mL/min
- Cohort 2: eGFR >=45 mL/min
n=300 (US), n=150 (EMEA)
n=30 (US)
Cohort 1: Newly diagnosed, no prior systemic treatment (1L): SC amivantamab Q4W + lazertinib PO QD
Cohort 2: Progression on/after EGFR TKI monotherapy (2L): SC amivantamab Q3W + IV carboplatin Q3W + IV pemetrexed Q3W
Cohort 1: Dermatologic AE prophylaxis + VTE
Cohort 2: Dermatologic AE prophylaxis
Cohort 1
Primary endpoint: INV PFS per RECIST v1.1
Key secondary endpoints: Incidence and severity of dermatologic AEs and VTE; OS; ORR; CBR; DoR
Dosing (in 28-day cycles): SC amivantamab SC abdominal injection 1600 mg (2240 mg if >=80 kg) weekly for the first four weeks, and 3520 mg (4640 mg if >=80 kg) Q4W thereafter. Lazertinib 240 mg orally daily.
Goldberg S et al ASCO 2026
At #DAVALung, Dr. Natasha Leighl (@pmcancercentre) presented OptiTROP-Lung05: Sac-TMT+pembro vs pembro in 1L PD-L1+ advanced NSCLC without EGFR/ALK alterations. PFS improved (HR 0.35; p<0.0001); ORR 70.2% vs 42.0%; no new safety signals.
OptiTROP-Lung05
[Slide 1]
OptiTROP-Lung05: Safety
Event, n (%) | Sac-TMT + Pembro (n=208) Any grade | Grade >=3 | Pembro (n=204) Any grade | Grade >=3
Treatment-emergent AEs | 207 (99.5) | 115 (55.3) | 178 (87.3) | 64 (31.4)
Serious | 81 (38.9) | - | 59 (28.9) | -
Led to discontinuation of sac-TMT/pembro | 8 (3.8) / 11 (5.3) | - | 10 (4.9) | -
Led to death | 5 (2.4) | - | 13 (6.4) | -
Common TEAEs:
Anemia | 182 (87.5) | 19 (9.1) | 55 (27.0) | 2 (1.0)
Alopecia | 137 (65.9) | 0 | 6 (2.9) | 0
White blood cell count decreased | 96 (46.2) | 18 (8.7) | 5 (2.5) | 1 (0.5)
Neutrophil count decreased | 93 (44.7) | 36 (17.3) | 3 (1.5) | 1 (0.5)
Stomatitis | 84 (40.4) | 11 (5.3) | 3 (1.5) | 0
Decreased appetite | 73 (35.1) | 2 (1.0) | 27 (13.2) | 0
Weakness | 71 (34.1) | 8 (3.8) | 23 (11.3) | 2 (1.0)
Nausea | 70 (33.7) | 0 | 11 (5.4) | 0
Hypoalbuminemia | 61 (29.3) | 0 | 35 (17.2) | 0
Weight decreased | 56 (26.9) | 1 (0.5) | 19 (9.3) | 1 (0.5)
ALT increased | 55 (26.4) | 1 (0.5) | 33 (16.2) | 0
Rash | 50 (24.0) | 6 (2.9) | 33 (16.2) | 1 (0.5)
- Median duration of exposure: Sac-TMT + Pembro: Sac-TMT 8.9 months/Pembro 8.3 months; Pembro alone: 5.1 months
- Higher incidence of grade >=3 TEAEs with sac-TMT+ pembro vs. pembro, primarily driven by expected hematologic AEs of sac-TMT
- Treatment-emergent AEs leading to discontinuation of pembro were similar in both groups. No treatment-related deaths were attributed to sac-TMT
Zhou C et al. ASCO 2026. (Abstract #: 8506)
———
[Slide 2]
OptiTROP-Lung05: ORR, deep response, and DOR (BICR)
Sac-TMT + pembro improved ORR, deep response rate, and duration of response vs. pembro
ORR: ITT Sac-TMT+Pembro 70.2% vs Pembro 42.0% (Delta 28.3%); TPS >=50% 80.7% vs 60.5%; TPS 1-49% 63.2% vs 30.1%
Deep Response Rate (>=50% SLD reduction): ITT 49.0% vs 25.9% (Delta 23.2%); TPS >=50% 62.7% vs 40.7%; TPS 1-49% 40.0% vs 16.3%
Duration of response: Sac-TMT+Pembro 77.7% vs Pembro 59.4%; HR 0.47 (95% CI: 0.27, 0.82)
Zhou C et al. ASCO 2026. (Abstract #: 8506)
———
[Slide 3]
OptiTROP-Lung05: PFS (BICR) by PD-L1 & histologic subgroups
TPS >=50%: HR 0.47 (95% CI: 0.29, 0.77); Sac-TMT+Pembro (n=83) 65.6% vs Pembro (n=82) 39.0%; PFS events n(%) 26 (31.3) vs 44 (53.7); mPFS mo NR (NE, NE) vs 9.5 (6.9, 13.8)
TPS 1-49%: HR 0.28 (95% CI: 0.19, 0.41); Sac-TMT+Pembro (n=125) 60.1% vs Pembro (n=123) 21.6%; PFS events 40 (32.0) vs 84 (68.3); mPFS NR (11.1, NE) vs 4.3 (2.9, 5.5)
Non-squamous: HR 0.28 (95% CI: 0.18, 0.43); 71.3% vs 33.0%; Sac-TMT+Pembro (n=123) vs Pembro (n=124); PFS events 29 (23.6) vs 70 (56.5); mPFS NR (13.6, NE) vs 6.6 (4.3, 8.7)
Squamous: HR 0.44 (95% CI: 0.29, 0.66); 51.3% vs 24.6%; Sac-TMT+Pembro (n=85) vs Pembro (n=80); PFS events 37 (43.5) vs 58 (72.5); mPFS NR (8.3, NE) vs 5.5 (4.1, 7.0)
One patient with thymoma was excluded from the pembro group in the subgroup analysis of histology; Zhou C et al. ASCO 2026. (Abstract #: 8506)
———
[Slide 4]
OptiTROP-Lung05: PFS, (Exploratory) OS
PFS by BICR: Sac-TMT + Pembro (n=208) PFS events 66 (31.7), Median NR (13.6, NE); Pembro (n=205) 128 (62.4), Median 5.7 (4.3, 7.0). 62.4% vs 29.0%. HR 0.35 (95% CI: 0.26, 0.47) p < 0.0001. Sac-TMT + pembro significantly improved PFS vs. pembro, with a 65% reduction in risk of disease progression or death
Descriptive OS at PFS IA: Sac-TMT + Pembro (n=208) OS events 33 (15.9), Median NR (NE, NE); Pembro (n=205) 54 (26.3), Median 14.5 (14.5, NE). HR 0.55 (95% CI: 0.36, 0.85). Sac-TMT + pembro improved PFS vs. pembro, with a 62% reduction in risk of disease progression or death
Zhou C et al. ASCO 2026. (Abstract #: 8506)
Atypical EGFR-mutant NSCLC requires more than a one-size-fits-all approach. Dr @JuliaRotow (@DanaFarber) discusses management of uncommon EGFR alterations, first-line treatment selection, amivantamab/lazertinib data, and next-gen EGFR TKIs at #DAVALung
[Slide 1]
The spectrum of EGFR mutations
Pie chart: PACC (incl. compound) 12.5%; Exon 20 insertions 9.1%; Other uncommon (incl. L861Q) 9.2%; Classical (incl. T790M) 69.2%
Exon distribution: Exon 18 (688-728): E709_T710delinsD 4%, E709X 10.3%, G719X 40.7%, G724S* 1.6%; Exon 19 (729-761): I740_K745dup 1.7%, L747X 3.1%; Exon 20 (762-823): S768I 20.7%, V769X 4%, V774M 2.8%, R776X 3.4%, G779F 1.7%; Exon 21 (824-875): C797S* 3%
PACC Ex G719X:
- Afatinib alone
- Off-label Osimertinib +/- chemotherapy
- Off-label amivantamab + lazertinib
- Clinical trials
Classical-Like Ex: L816Q:
- Reasonable to use similar strategy to L858R/del19
- Eg osimertinib monotherapy or 1L combinations
Le et al WCLC 2024; Robichaux et al Nature. 2021; Yang et al. 2015; Yang et al. 2020; Bar et al. JTO. 2021; Cho et al #8516 ASCO 2024
Dana-Farber Cancer Institute
———
[Slide 2]
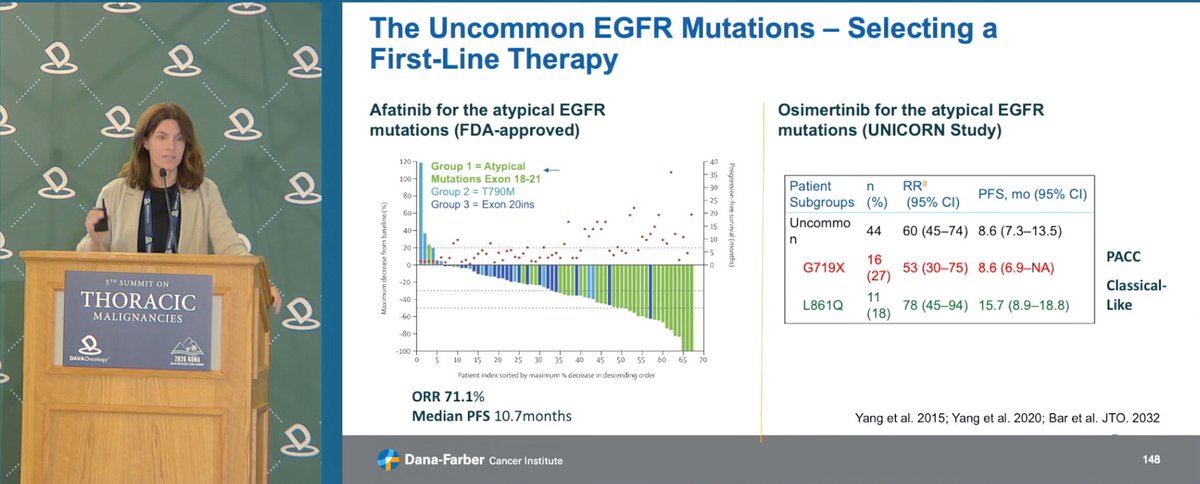
The Uncommon EGFR Mutations - Selecting a First-Line Therapy
Afatinib for the atypical EGFR mutations (FDA-approved):
Waterfall plot - Group 1 = Atypical Mutations Exon 18-21; Group 2 = T790M; Group 3 = Exon 20ins
ORR 71.1%; Median PFS 10.7 months
Osimertinib for the atypical EGFR mutations (UNICORN Study):
Patient Subgroups | n (%) | RR (95% CI) | PFS, mo (95% CI)
Uncommon | 44 | 60 (45-74) | 8.6 (7.3-13.5)
G719X | 16 (27) | 53 (30-75) | 8.6 (6.9-NA) [PACC]
L861Q | 11 (18) | 78 (45-94) | 15.7 (8.9-18.8) [Classical-Like]
Yang et al. 2015; Yang et al. 2020; Bar et al. JTO. 2032
Dana-Farber Cancer Institute
———
[Slide 3]
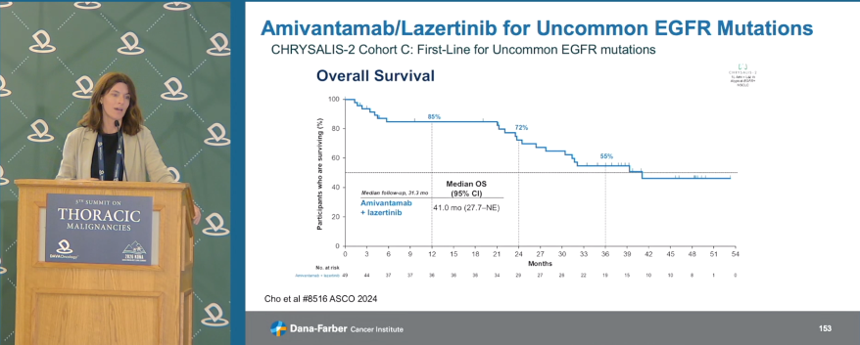
Amivantamab/Lazertinib for Uncommon EGFR Mutations
CHRYSALIS-2 Cohort C: First-Line for Uncommon EGFR mutations
Investigator-assessed response (n=49):
Median follow-up | 17.3 mo (range, 0.1-31.5)
ORR | 57% (95% CI, 42-71)
Median DoR | 20.7 mo (95% CI, 9.9-NE)
DoR >=6 mo, n (%) | 21 (75)
CBR | 84% (95% CI, 70-93)
Median PFS | 19.5 mo (95% CI, 11.2-NE)
Median OS | NE (95% CI, 26.3-NE)
Waterfall: Change in SoD of target lesions (%); PR, SD
Cho et al #8516 ASCO 2024; Le et al WCLC 2024
Dana-Farber Cancer Institute
———
[Slide 4]
Amivantamab/Lazertinib for Uncommon EGFR Mutations
CHRYSALIS-2 Cohort C: First-Line for Uncommon EGFR mutations
Overall Survival KM: Amivantamab + lazertinib (n=49). Landmark survival 85% (12 mo), 72% (24 mo), 55% (36 mo). Median follow-up 31.3 mo. Median OS (95% CI) 41.0 mo (27.7-NE)
Cho et al #8516 ASCO 2024
Dana-Farber Cancer Institute
Dr. @JuliaRotow@DanaFarber discussed the evolving role of resistance-matched therapies in EGFR-mutant NSCLC, emphasizing targeted approaches for MET amplification, EGFR C797S, secondary fusions, and HER2 alterations. #DAVALung
SACHISAVANNAH
[Slide 1]
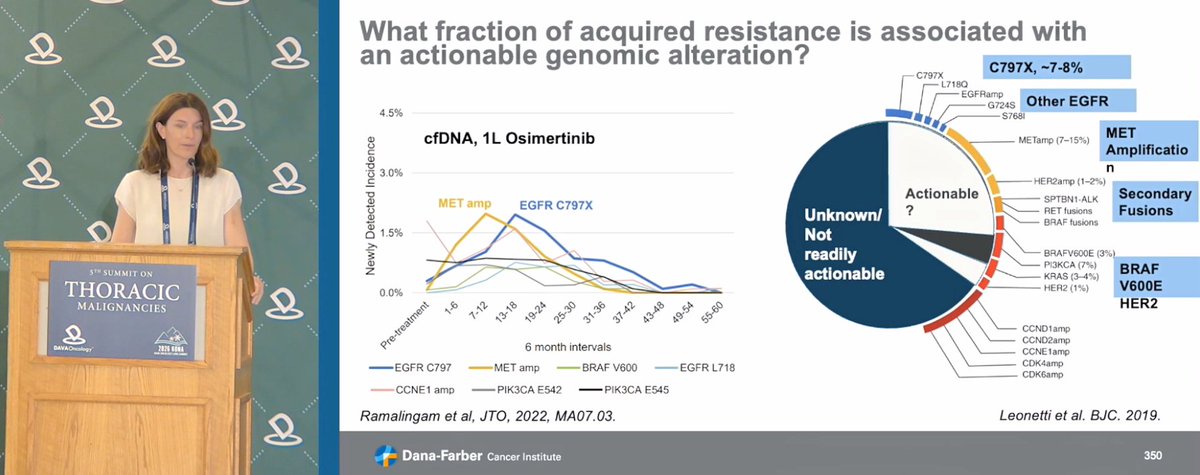
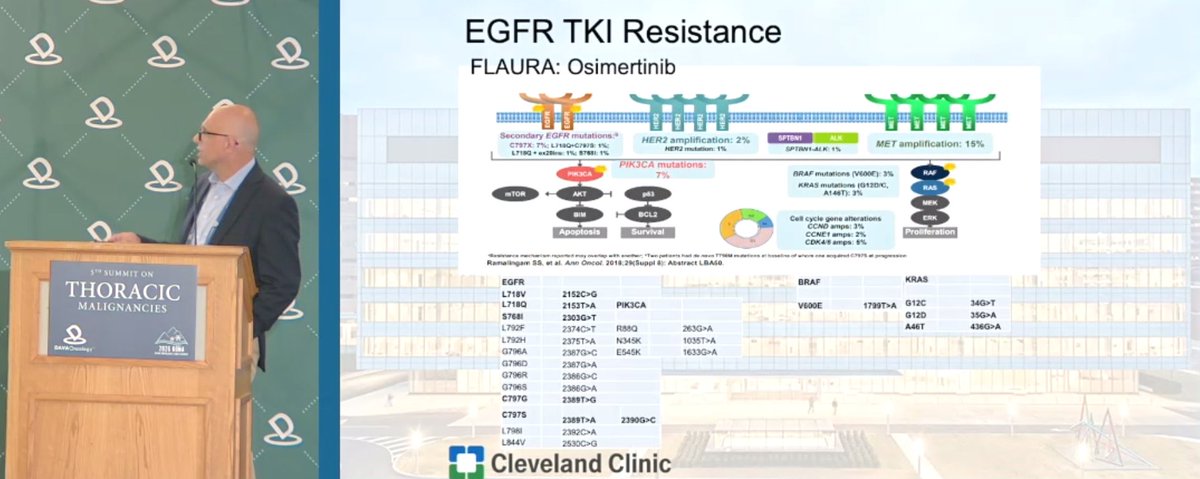
What fraction of acquired resistance is associated with an actionable genomic alteration?
cfDNA, 1L Osimertinib. Newly Detected Incidence (%) vs 6 month intervals (Pre-treatment, 1-6, 7-12, 13-18, 19-24, 25-30, 31-36, 37-42, 43-48, 49-54, 55-60). Lines: EGFR C797, MET amp, BRAF V600, EGFR L718, CCNE1 amp, PIK3CA E542, PIK3CA E545. MET amp and EGFR C797X peak ~1.8-2.0% around 13-24 months.
Ramalingam et al, JTO, 2022, MA07.03.
Actionable pie chart: Unknown/Not readily actionable (large) vs Actionable?. C797X, ~7-8%. Other EGFR: L718Q, EGFRamp, G724S, S768I. MET Amplification: METamp (7-15%). HER2amp (1-2%). Secondary Fusions: SPTBN1-ALK, RET fusions, BRAF fusions. BRAF V600E (3%). PI3KCA (7%). KRAS (3-4%). HER2 (1%). CCND1amp, CCND2amp, CCNE1amp, CDK4amp, CDK6amp.
Leonetti et al. BJC. 2019.
Dana-Farber Cancer Institute. 350
———
[Slide 2]
BH-30643 for C797S
Cell Proliferation Inhibition IC50 (nM) for BH-30643, BLU-945, BDTX-1535, Osimertinib. Classical; Classical/C797S; Classical/T790M; Classical/T790M/C797S; EGFR WT amp. Note: Classical L858R and ex19del, Any IC50 value > 1000 nM was plotted as 1000 nM.
Waterfall: Best Change in SoD of Target Lesions (%). Chemo Naive and Chemo Treated. Doses: 20 mg BID, 40 mg BID, 50 mg BID, 60 mg BID. * Indicates only one follow-up scan is available and treatment is ongoing. Responses labeled SD, PD, cPR, uPR.
Driver Mutation: Exon19del, Exon19delins, L858R, G719X, E709K. Rows: C797S, T790M, Osimertinib, Afatinib, Amivantamab, No. Prior Lines THX, Prior Brain Mets.
Le et al ASCO 2026. ORR (unconfirmed) 39-50%.
Dana-Farber Cancer Institute. 355
———
[Slide 3]
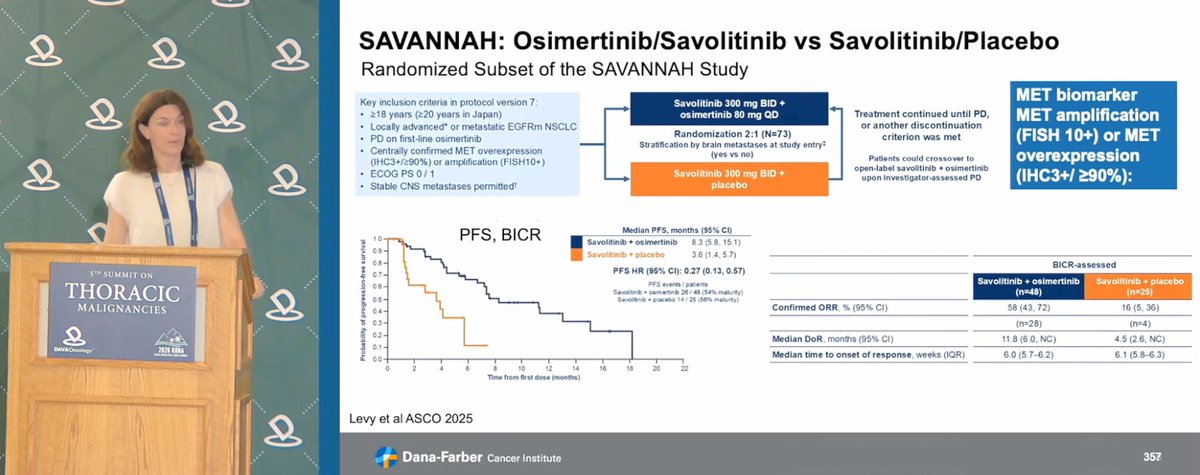
SAVANNAH: Osimertinib/Savolitinib vs Savolitinib/Placebo. Randomized Subset of the SAVANNAH Study.
Key inclusion criteria in protocol version 7: >=18 years (>=20 years in Japan); Locally advanced or metastatic EGFRm NSCLC; PD on first-line osimertinib; Centrally confirmed MET overexpression (IHC3+/>=90%) or amplification (FISH10+); ECOG PS 0/1; Stable CNS metastases permitted.
Arms: Savolitinib 300 mg BID + osimertinib 80 mg QD; Savolitinib 300 mg BID + placebo. Randomization 2:1 (N=73), stratification by brain metastases at study entry. Patients could crossover to open-label savolitinib + osimertinib upon investigator-assessed PD.
MET biomarker: MET amplification (FISH 10+) or MET overexpression (IHC3+/>=90%).
PFS, BICR — Median PFS, months (95% CI): Savolitinib + osimertinib 8.3 (5.8, 15.1); Savolitinib + placebo 3.6 (1.4, 5.7). PFS HR (95% CI): 0.27 (0.13, 0.57). PFS events/patients: Savo+osi 26/48 (54% maturity); Savo+placebo 14/25 (56% maturity).
BICR-assessed: Savolitinib + osimertinib (n=48) vs Savolitinib + placebo (n=25). Confirmed ORR, % (95% CI): 58 (43, 72) [n=28] vs 16 (5, 36) [n=4]. Median DoR, months (95% CI): 11.8 (6.0, NC) vs 4.5 (2.6, NC). Median time to onset of response, weeks (IQR): 6.0 (5.7-6.2) vs 6.1 (5.8-6.3).
Levy et al ASCO 2025.
Dana-Farber Cancer Institute. 357
———
[Slide 4]
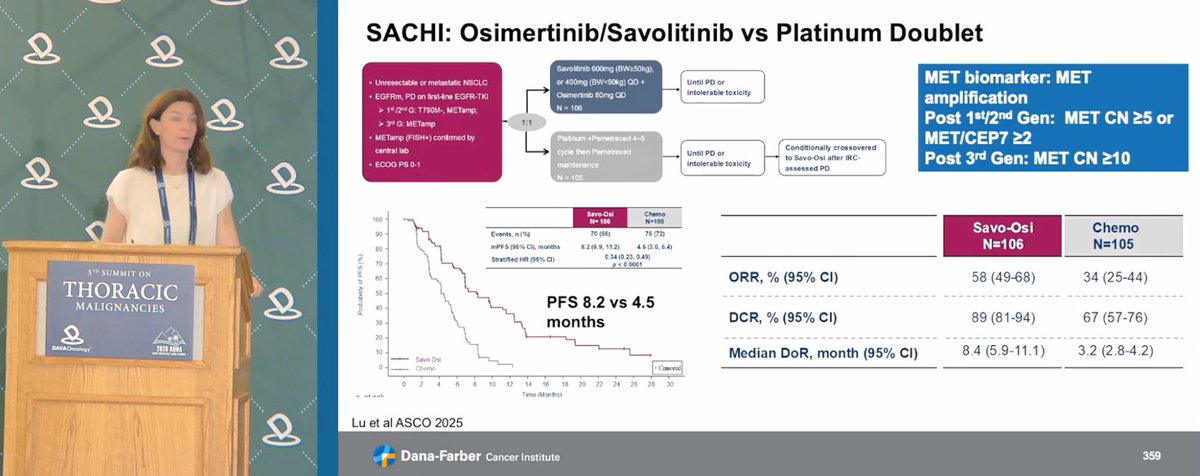
SACHI: Osimertinib/Savolitinib vs Platinum Doublet.
Eligibility: Unresectable or metastatic NSCLC; EGFRm, PD on first-line EGFR-TKI (1st/2nd G: T790M-, METamp; 3rd G: METamp); METamp (FISH+) confirmed by central lab; ECOG PS 0-1.
Arms: Savolitinib 600mg (BW>=50kg), or 400mg (BW<50kg) QD + Osimertinib 80mg QD, N=106; vs Platinum + Pemetrexed 4-6 cycle then Pemetrexed maintenance, N=105. Randomization 1:1. Until PD or intolerable toxicity. Conditionally crossover to Savo-Osi after IRC-assessed PD.
MET biomarker: MET amplification. Post 1st/2nd Gen: MET CN >=5 or MET/CEP7 >=2. Post 3rd Gen: MET CN >=10.
PFS KM — Savo-Osi N=106 vs Chemo N=105. Events, n (%): 70 (66) vs 76 (72). mPFS (95% CI), months: 8.2 (6.9, 11.2) vs 4.5 (3.0, 6.4). Stratified HR (95% CI): 0.34 (0.23, 0.49), p<0.0001. PFS 8.2 vs 4.5 months.
ORR, % (95% CI): 58 (49-68) vs 34 (25-44). DCR, % (95% CI): 89 (81-94) vs 67 (57-76). Median DoR, month (95% CI): 8.4 (5.9-11.1) vs 3.2 (2.8-4.2).
Lu et al ASCO 2025.
Dana-Farber Cancer Institute. 359
Next-generation EGFR TKIs address resistance, CNS activity and tolerability gaps in EGFR-mutant NSCLC. Dr @LeXiuning (@MDAndersonNews) discusses novel EGFR TKIs, including BH-30643 & BDTX1535, focusing on overcoming C797S/T790M, safety & clinical activity #DAVALung
[Slide 1]
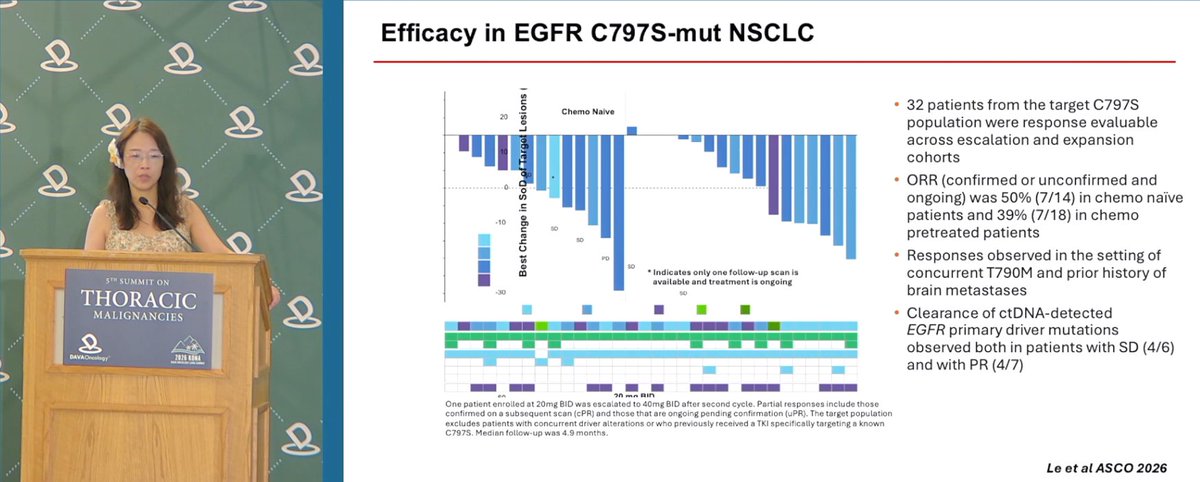
Efficacy in EGFR C797S-mut NSCLC
Waterfall: Best Change in SoD of Target Lesions; Chemo Naive; SD/PD annotations; * Indicates only one follow-up scan is available and treatment is ongoing. Dose 20 mg BID / 40 mg BID.
• 32 patients from the target C797S population were response evaluable across escalation and expansion cohorts
• ORR (confirmed or unconfirmed and ongoing) was 50% (7/14) in chemo naive patients and 39% (7/18) in chemo pretreated patients
• Responses observed in the setting of concurrent T790M and prior history of brain metastases
• Clearance of ctDNA-detected EGFR primary driver mutations observed both in patients with SD (4/6) and with PR (4/7)
One patient enrolled at 20mg BID was escalated to 40mg BID after second cycle. Partial responses include those confirmed on a subsequent scan (cPR) and those that are ongoing pending confirmation (uPR). The target population excludes patients with concurrent driver alterations or who previously received a TKI specifically targeting a known C797S. Median follow-up was 4.9 months.
Le et al ASCO 2026
———
[Slide 2]
Safety & tolerability
Safety Population (N=82) | TRAE Any Gr / Gr 1 / Gr 2 / Gr 3* | TEAE Any Gr / Gr 3+
Any AE, n (%): 71 (87) / 34 (41) / 21 (26) / 16 (20) | 80 (98) / 33 (40)
EGFR wildtype-related AEs:
Diarrhea: 30 (37) / 22 (27) / 8 (10) / 0 | 35 (43) / 0
Rash: 30 (37) / 20 (24) / 7 (9) / 3 (4) | 34 (41) / 3 (4)
Stomatitis: 15 (18) / 6 (7) / 7 (9) / 2 (2) | 16 (20) / 2 (2)
Dry skin: 10 (12) / 9 (11) / 1 (1) / 0 | 14 (17) / 0
Paronychia: 8 (10) / 2 (2) / 5 (6) / 1 (1) | 11 (13) / 1 (1)
Additional TRAEs reported in ≥ 10% of patients:
Bilirubin increased: 29 (35) / 7 (9) / 11 (13) / 11 (13) | 31 (38) / 11 (13)
Fatigue: 14 (17) / 10 (12) / 3 (4) / 1 (1) | 18 (22) / 2 (2)
Nausea: 10 (12) / 4 (5) / 6 (7) / 0 | 14 (17) / 0
Median duration of exposure was 2.8 months.
* The one grade 4 TRAE was ALT elevation, observed following recent immune-checkpoint inhibitor therapy, and recovered with dose interruption and steroids; no grade 5 TRAE were reported.
• 3 DLTs were reported, at 80mg BID (Gr. 3 mucositis, bilirubin increased) and at 60mg BID (Gr. 3 mucositis)
• Grade ≥2 EGFR-wildtype TRAEs reported in 27% of patients, more commonly at ≥60mg BID
• Bilirubin elevation has been predominately unconjugated and asymptomatic, and generally seen early on treatment due to exposure-dependent UGT1A1 inhibition (Gilbert's-like) by BH-30643
• Treatment-emergent ALT/AST elevations were observed in 12 patients (15%, two Gr. 3, one Gr. 4) with no cases of Hy's Law
• No clinically significant QTc prolongation or treatment-related cardiac effects
• TRAE leading to dose reduction in 13 patients (16%, most commonly bilirubin elevation), and discontinuation in 1 patient (1%)
Le et al ASCO 2026
———
[Slide 3]
DZD6008 is fully BBB-penetrant and potently inhibits various tumor cell lines with single, double, and triple EGFR mutations
pEGFR Inhibition Pharmacodynamic Effect; Anti-proliferative activity Cellular Activities; Anti-tumor activity In Vivo Activities; Anti-CNS metastasis activity (10 mg/kg and 30 mg/kg DZD6008 imaging). EGFR alterations in cells: Classical EGFR mutation; Acquired mutation to 1st-Gen EGFR TKI; Acquired mutation to 3rd-Gen EGFR TKI.
*Mutant EGFR includes H3255, PC9, and Ba/F3 engineered with L,D, LT, DT, LC, DC, LTC, DTC. # WT EGFR includes 42 NSCLC cells.
• DZD6008 potently inhibits major EGFR single-, double-, and triple-mutant variants in cellular assays, in cis and in trans
• DZD6008 is highly effective, at well-tolerated doses, in animal models expressing EGFR activating mutations, acquired resistant T790M and C797S mutations
• DZD6008 is not active in wild-type EGFR driven cells or in vivo models
• DZD6008 is potent in anti-CNS metastasis models, Kpuu,CSF >1.2
PRESENTED BY: Mengzhao Wang, MD (2026 ASCO Annual Meeting, #ASCO26)
———
[Slide 4]
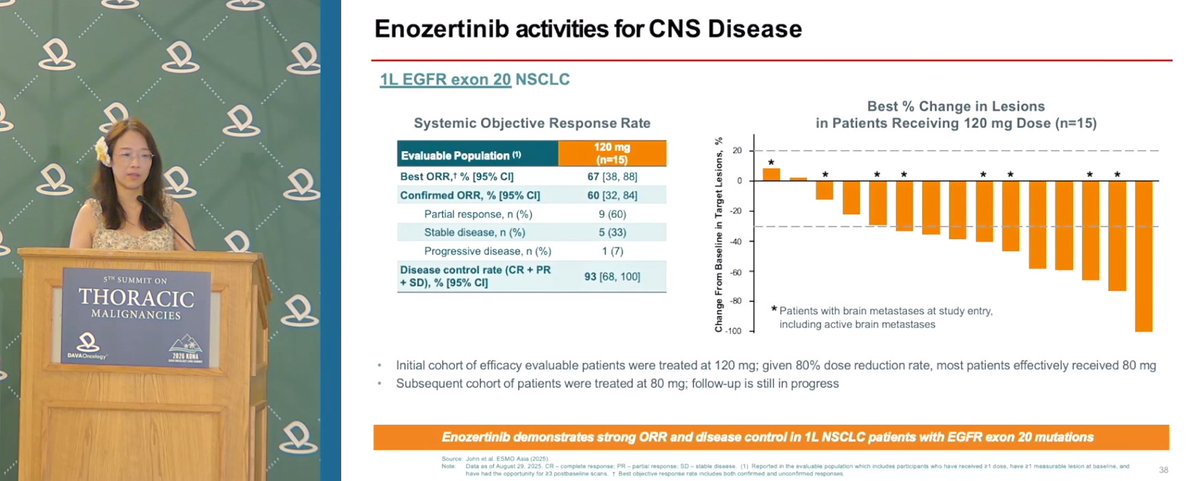
Enozertinib activities for CNS Disease
1L EGFR exon 20 NSCLC
Systemic Objective Response Rate — Evaluable Population, 120 mg (n=15):
Best ORR, % [95% CI]: 67 [38, 88]
Confirmed ORR, % [95% CI]: 60 [32, 84]
Partial response, n (%): 9 (60)
Stable disease, n (%): 5 (33)
Progressive disease, n (%): 1 (7)
Disease control rate (CR + PR + SD), % [95% CI]: 93 [68, 100]
Best % Change in Lesions in Patients Receiving 120 mg Dose (n=15): waterfall; * Patients with brain metastases at study entry, including active brain metastases.
• Initial cohort of efficacy evaluable patients were treated at 120 mg; given 80% dose reduction rate, most patients effectively received 80 mg
• Subsequent cohort of patients were treated at 80 mg; follow-up is still in progress
Enozertinib demonstrates strong ORR and disease control in 1L NSCLC patients with EGFR exon 20 mutations
Source: John et al. ESMO Asia (2025). Data as of August 29, 2025.
Dr. @riess_md (@UCD_Cancer) presented Dato-DXd in EGFR-mutated NSCLC: pooled TL-01/TL-05 ORR 43%, mPFS 5.8m, mOS 15.6m; ORCHARD evaluated Dato-DXd + osimertinib after prior osimertinib. NMR biomarker unclear; other TROP2 ADCs in development. #DAVALung
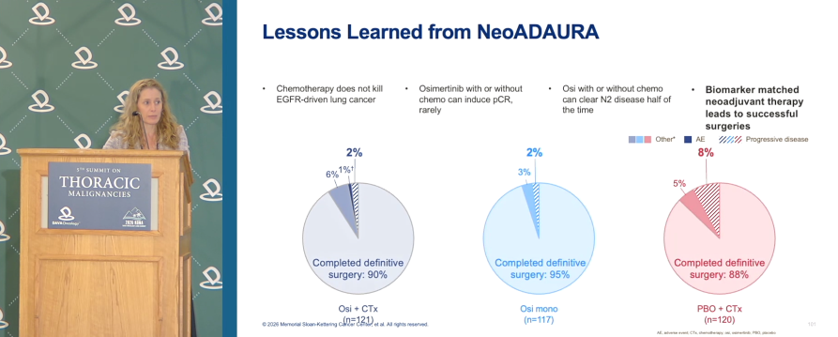
Key lessons from Dr. Jamie Chaft @MSKCancerCenter on NeoADAURA: chemotherapy alone had limited impact in EGFR-driven NSCLC, while osimertinib +/- chemo rarely induced pCR, cleared N2 disease ~half the time, and enabled high rates of definitive surgery. #DAVALung
NeoADAURA
[Slide 1]
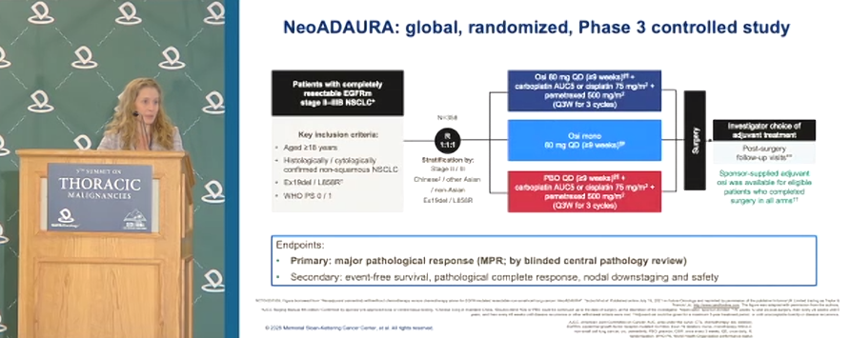
NeoADAURA: global, randomized, Phase 3 controlled study
Patients with completely resectable EGFRm stage II-IIIB NSCLC. N=358. R 1:1:1.
Key inclusion criteria: Aged >=18 years; Histologically / cytologically confirmed non-squamous NSCLC; Ex19del / L858R; WHO PS 0 / 1.
Stratification by: Stage (II vs III); Chinese / other Asian / non-Asian; Ex19del / L858R.
Arm 1: Osi 80 mg QD (>=9 weeks) + carboplatin AUC5 or cisplatin 75 mg/m2 + pemetrexed 500 mg/m2 (Q3W for 3 cycles).
Arm 2: Osi mono 80 mg QD (>=9 weeks).
Arm 3: PBO QD (>=9 weeks) + carboplatin AUC5 or cisplatin 75 mg/m2 + pemetrexed 500 mg/m2 (Q3W for 3 cycles).
Surgery. Investigator choice of adjuvant treatment. Post-surgery follow-up visits. Sponsor-supplied adjuvant osi was available for eligible patients who completed surgery in all arms.
Endpoints:
Primary: major pathological response (MPR; by blinded central pathology review)
Secondary: event-free survival, pathological complete response, nodal downstaging and safety
———
[Slide 2]
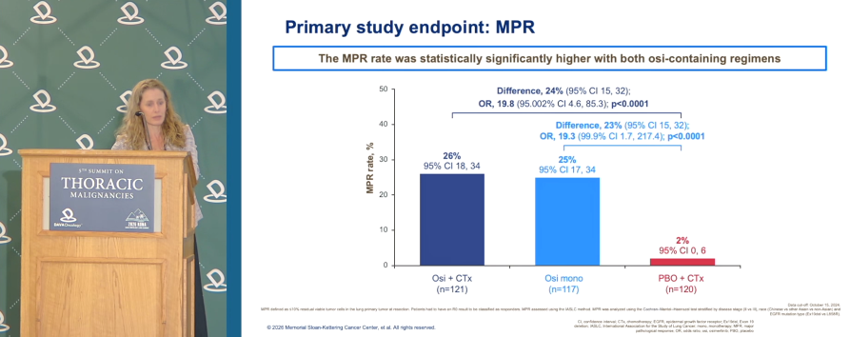
Primary study endpoint: MPR
The MPR rate was statistically significantly higher with both osi-containing regimens
Osi + CTx (n=121): MPR rate 26% (95% CI 18, 34). Difference, 24% (95% CI 15, 32); OR, 19.8 (95.002% CI 4.6, 85.3); p<0.0001
Osi mono (n=117): MPR rate 25% (95% CI 17, 34). Difference, 23% (95% CI 15, 32); OR, 19.3 (99.9% CI 1.7, 217.4); p<0.0001
PBO + CTx (n=120): MPR rate 2% (95% CI 0, 6)
Data cut-off October 15, 2024
———
[Slide 3]
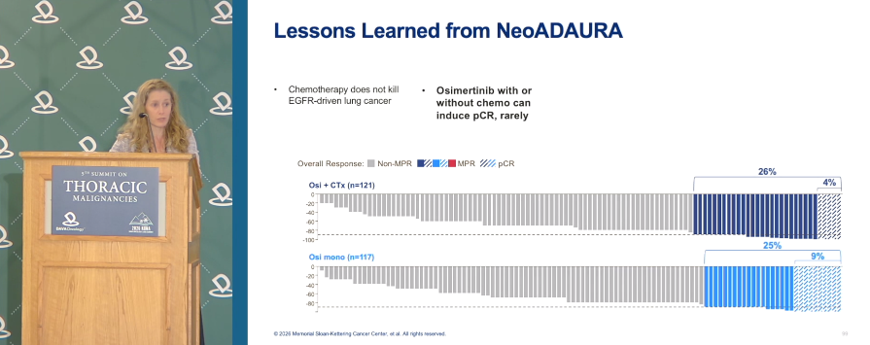
Lessons Learned from NeoADAURA
- Chemotherapy does not kill EGFR-driven lung cancer
- Osimertinib with or without chemo can induce pCR, rarely
Waterfall / overall response (Non-MPR, MPR, pCR):
Osi + CTx (n=121): MPR 26%, pCR 4%
Osi mono (n=117): MPR 25%, pCR 9%
———
[Slide 4]
Lessons Learned from NeoADAURA
- Chemotherapy does not kill EGFR-driven lung cancer
- Osimertinib with or without chemo can induce pCR, rarely
- Osi with or without chemo can clear N2 disease half of the time
- Biomarker matched neoadjuvant therapy leads to successful surgeries
Completed definitive surgery:
Osi + CTx (n=121): 90% (progressive disease 2%, AE 1%, other 6%)
Osi mono (n=117): 95% (progressive disease 2%, other 3%)
PBO + CTx (n=120): 88% (progressive disease 8%, AE 5%)
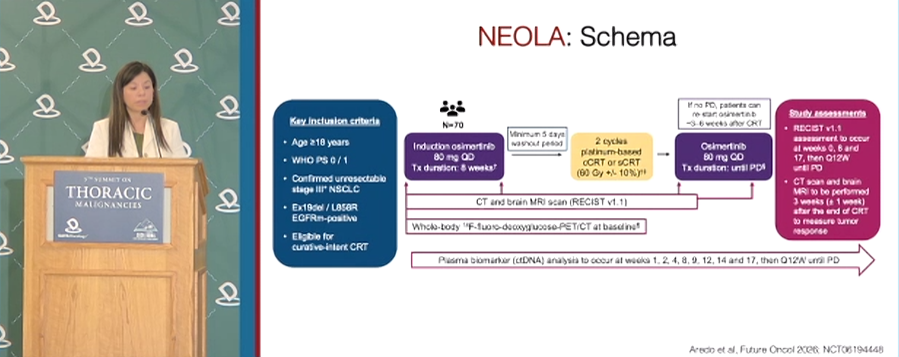
Dr. @JackieAredoMD@StanfordCancer highlights NEOLA: induction osimertinib before CRT + maintenance osi in unresectable stage III EGFR Ex19del/L858R NSCLC showed preliminary ORR 77%, no new safety signals, and did not prevent definitive CRT. #DAVALung
[Slide 1]
Is there a role for induction EGFR TKIs before CRT?
| Induction Erlotinib | Induction Gefitinib | Induction Afatinib | Induction Osimertinib
Study | RTOG-1306 | LOGIK0902/OLCSG0905 | ASCENT | Peled, et al.
Design | Randomized Phase II | Single Arm Phase II | Single Arm Phase II | Single Arm Phase II
Time Period | 2013-2018 | 2011-2017 | 2012-2020 | 2017-2022
Tx Duration | 12 weeks | 8 weeks | 8 weeks | 12 weeks
Definitive Treatment | Concurrent CRT | Concurrent CRT | Concurrent CRT +/- Surgery +/- Afatinib | RT and/or Surgery
Sample Size | --- | 20 | 19 | 21
ORR | --- | 85.0% | 63.2% | 95.2%
Median PFS | --- | 1.4 years | 2.6 years | Not reached
Median OS | --- | 5.5 years | 5.8 years | Not reached
Hotta et al. ESMO Open 2021; Hotta et al. Int J Clin Oncol 2025; Chang et al. Onc 2024; Peled et al. Int J Radiation Oncol Biol Phys 2025
———
[Slide 2]
"Neo-LAURA" NEOLA: Phase II Global Study
- Design: Multicenter, single-arm, open-label, phase II study
- Objective: Evaluate the efficacy and safety of induction osimertinib prior to CRT and maintenance osimertinib
- Sample Size: 75 patients
- Key Inclusion Criteria:
- Age >= 18 years
- Stage III (IASLC v.8)
- EGFR exon 19 deletion or L858R
- Planned to undergo concurrent or sequential CRT
- Primary Endpoint: 12-month PFS
- Secondary Endpoints: 8-week ORR and DCR, OS, EFS, safety
- Sponsor: AstraZeneca, Cambridge, UK
Aredo et al, Future Oncol 2025; NCT06194448
———
[Slide 3]
NEOLA: Schema
Key inclusion criteria: Age >= 18 years; WHO PS 0/1; Confirmed unresectable stage III NSCLC; Ex19del / L858R EGFRm-positive; Eligible for curative-intent CRT
N=70 -> Induction osimertinib 80 mg QD, Tx duration: 8 weeks -> Minimum 5 days washout period -> 2 cycles platinum-based cCRT or sCRT (60 Gy +/- 10%) -> Osimertinib 80 mg QD, Tx duration: until PD -> If no PD, patients can re-start osimertinib 3-6 weeks after CRT
CT and brain MRI scan (RECIST v1.1); Whole-body 18F-fluoro-deoxyglucose-PET/CT at baseline; RECIST v1.1 assessment to occur at weeks 0, 8 and 17, then Q12W; CT scan and brain MRI to be performed 3 weeks after the end of CRT to measure tumor response
Plasma biomarker (cfDNA) analysis to occur at weeks 1, 2, 4, 8, 9, 12, 14 and 17, then Q12W until PD
Aredo et al, Future Oncol 2026; NCT06194448
———
[Slide 4]
ORR was similar to the observed response to first-line osimertinib in the FLAURA trial in advanced EGFRm NSCLC (ORR 80%)
| N=30
Confirmed ORR, % (95% CI) | 77 (58, 90)
Partial response, n (%) | 23 (77)
Stable disease, n (%) | 6 (20)
Progressive disease, n (%) | 1 (3)
Not evaluable, n (%) | 0
Disease control rate, % (95% CI) | 97 (83, 100)
Wing Chen. Chen et al, ESMO Asia 2025
Dr. @CoreyLangerMD (@PennMedicine) reviewed adjuvant selpercatinib in early-stage RET fusion+ NSCLC: LIBRETTO-432 met its primary EFS endpoint vs placebo (stage II–IIIA HR 0.17; p<0.001), with safety consistent with known selpercatinib profile. #DAVALung
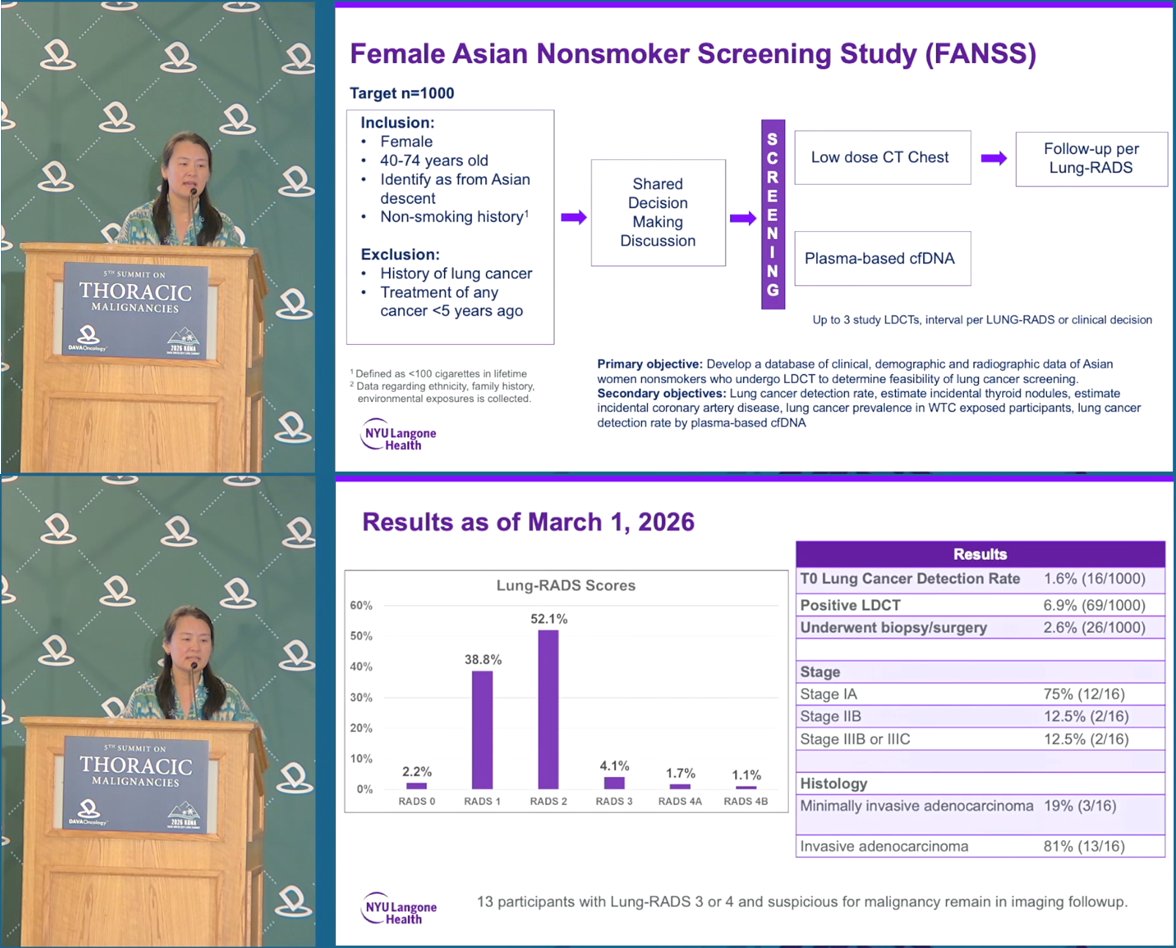
Screening never-smokers: Screening works in never-smokers: FANSS, the US non-smoker program, detected cancer in 1.6% (vs NLST 1.1% & NELSON 0.9%), each tumor carrying an EGFR/HER2 driver, groundglass opacities posing a diagnostic challenge. Dr. @ElaineShumMD (@nyulangone) at
SOLSTICETALENT
[Slide 1]
Female Asian Nonsmoker Screening Study (FANSS)
Target n=1000
Inclusion: Female; 40-74 years old; Identify as from Asian descent; Non-smoking history(1)
Exclusion: History of lung cancer; Treatment of any cancer <5 years ago
Workflow: Shared Decision Making Discussion -> SCREENING -> Low dose CT Chest -> Follow-up per Lung-RADS; Plasma-based cfDNA. Up to 3 study LDCTs, interval per LUNG-RADS or clinical decision.
(1) Defined as <100 cigarettes in lifetime. (2) Data regarding ethnicity, family history, environmental exposures is collected.
Primary objective: Develop a database of clinical, demographic and radiographic data of Asian women nonsmokers who undergo LDCT to determine feasibility of lung cancer screening.
Secondary objectives: Lung cancer detection rate, estimate incidental thyroid nodules, estimate incidental coronary artery disease, lung cancer prevalence in WTC exposed participants, lung cancer detection rate by plasma-based cfDNA.
NYU Langone Health.
Results as of March 1, 2026
Lung-RADS Scores bar chart: RADS 0 = 2.2%; RADS 1 = 38.8%; RADS 2 = 52.1%; RADS 3 = 4.1%; RADS 4A = 1.7%; RADS 4B = 1.1%.
Results table: T0 Lung Cancer Detection Rate 1.6% (16/1000); Positive LDCT 6.9% (69/1000); Underwent biopsy/surgery 2.6% (26/1000).
Stage: Stage IA 75% (12/16); Stage IIB 12.5% (2/16); Stage IIIB or IIIC 12.5% (2/16).
Histology: Minimally invasive adenocarcinoma 19% (3/16); Invasive adenocarcinoma 81% (13/16).
13 participants with Lung-RADS 3 or 4 and suspicious for malignancy remain in imaging followup.
———
[Slide 2]
Lung Cancers Detected from T0:
- Lung-RADS 0 -> 2: 1
- Lung-RADS 2: 1
- Lung-RADS 3: 4
- Lung-RADS 4: 10
Mutation Status(1):
- EGFR exon 19 deletion: 5
- EGFR L858R: 9
- EGFR PACC: 1
- HER2 exon 20 insertion: 3
Family History: Yes 5 (31%); No 11 (69%)
(1) Two participants each with 2 separate primary lung adenocarcinomas.
Images labeled: Lung RADS 0->2; Lung RADS 2; Lung RADS 2; Lung RADS 4.
Additional Pathology: 2 participants with atypical adenomatous hyperplasia; 1 participant with adenocarcinoma in situ.
———
[Slide 3]
Comparison table: FANSS vs NLST vs TALENT
Screened population: FANSS = Asian women who never smoked; NLST = Individuals who have smoked at least 30 pack years and if former, quit in previous 15 years; TALENT = Asian men and women who never smoked and additional risk factor.
n: FANSS = 1,000; NLST = 26,722; TALENT = 12,011.
Positive Screen: FANSS = Lung-RADS 3 or 4: Solid, part solid nodule >=6mm; GGO >=30mm; NLST = Non-calcified nodule >=4mm; TALENT = Solid nodule >6mm; GGO >5mm.
Baseline LDCT Lung Cancer Detection Rate: FANSS = 1.6% (minimally invasive and invasive adenocarcinoma), 1.3% (invasive adenocarcinoma); NLST = 1.1%; TALENT = 2.6% (includes in situ and minimally invasive), 1.5% (invasive adenocarcinoma only).
NYU Langone Health.
———
[Slide 4]
Groundglass Opacities: A Diagnostic Challenge
From TALENT (pie chart): Invasive adenocarcinoma 70 (36.1%); Adenocarcinoma in situ 69 (35.6%); Minimally invasive adenocarcinoma 55 (28.4%).
Groundglass Nodules in FANSS (bar chart, GGO <=5mm / GGO >5-9mm / GGO >=10mm): Lung-RADS 1: 1, 0, 0; Lung-RADS 2: 67, 44, 11; Lung-RADS 3: 2, 8, 3; Lung-RADS 4: 0, 3, 3.
From SOLSTICE (bar chart, Smokers // Non-smokers by Lung-RADS Score): LR0 (5, 1.2%); LR1 (165, 39.3%); LR2 (236, 56.2%); LR3 (7, 1.7%); LR4A (5, 1.2%); LR4b (2, 0.5%); LR4x (0, 0%). Sub-panel percentages: LR 2(A) 69, 35.6% (84); LR 2(B) 71, 36.0% (85); LR 3 (7, 1.7%); LR 2(C) 3, 5.1%; LR 2(D) 56, 26.3% (67).
Chang G-C, et al. Lancet Respir Med 2023. Lai, G et al. WCLC 2025.
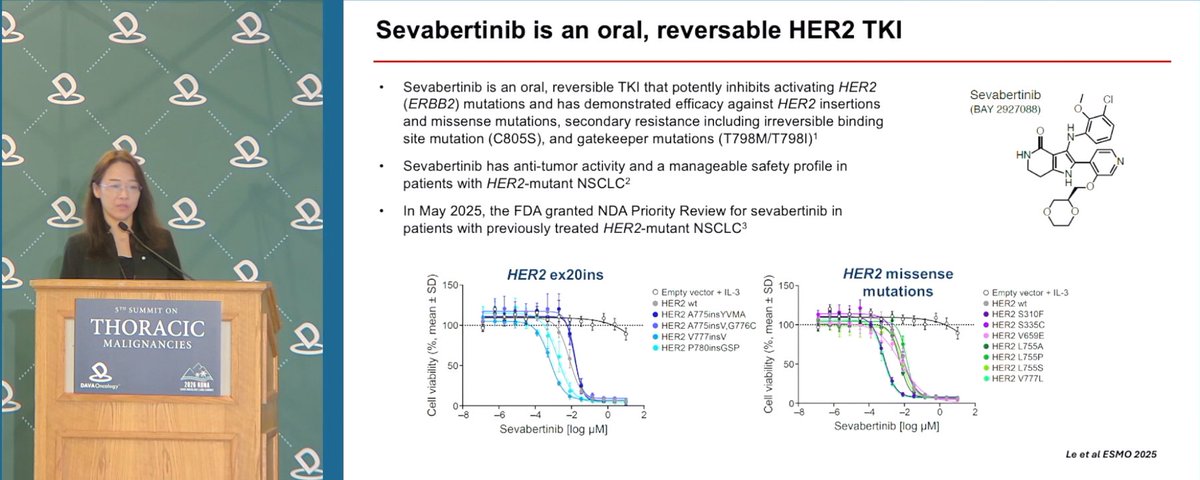
Dr. @LeXiuning from @UTMDAnderson shared insights on sevabertinib, an oral reversible HER2 TKI with activity across HER2 exon 20 insertion, missense, and resistance-associated mutations. The ongoing SOHO-01 study is evaluating its role in HER2-mutant NSCLC. #DAVALung
SOHO-01SOHO-02
[Slide 1]
Sevabertinib is an oral, reversable HER2 TKI
- Sevabertinib is an oral, reversible TKI that potently inhibits activating HER2 (ERBB2) mutations and has demonstrated efficacy against HER2 insertions and missense mutations, secondary resistance including irreversible binding site mutation (C805S), and gatekeeper mutations (T798M/T798I)1
- Sevabertinib has anti-tumor activity and a manageable safety profile in patients with HER2-mutant NSCLC2
- In May 2025, the FDA granted NDA Priority Review for sevabertinib in patients with previously treated HER2-mutant NSCLC3
Sevabertinib (BAY 2927088) [chemical structure]
[Dose-response curves] HER2 ex20ins: Cell viability (%, mean +/- SD) vs Sevabertinib [log uM] - Empty vector + IL-3, HER2 wt, HER2 A775insYVMA, HER2 A775insV,G776C, HER2 V777insV, HER2 P780insGSP.
HER2 missense mutations: Empty vector + IL-3, HER2 wt, HER2 S310F, HER2 S335C, HER2 V659E, HER2 L755A, HER2 L755P, HER2 L755S, HER2 V777L.
Le et al ESMO 2025
———
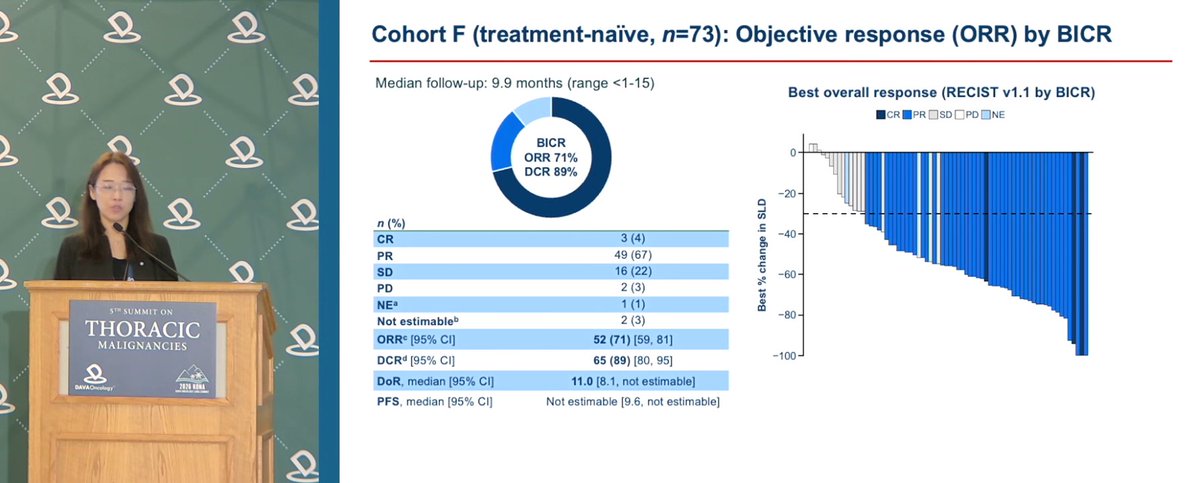
[Slide 2]
Cohort F (treatment-naive, n=73): Objective response (ORR) by BICR
Median follow-up: 9.9 months (range <1-15)
[Donut] BICR ORR 71% DCR 89%
Best overall response (RECIST v1.1 by BICR):
n (%)
CR: 3 (4)
PR: 49 (67)
SD: 16 (22)
PD: 2 (3)
NE(a): 1 (1)
Not estimable(b): 2 (3)
ORR(c) [95% CI]: 52 (71) [59, 81]
DCR(d) [95% CI]: 65 (89) [80, 95]
DoR, median [95% CI]: 11.0 [8.1, not estimable]
PFS, median [95% CI]: Not estimable [9.6, not estimable]
[Waterfall plot - Best % change in SLD; CR/PR/SD/PD/NE]
———
[Slide 3]
Sevabertinib safety and tolerability
ASCO 2026 update:
Table 3. Most common drug-related AEs occurring in >20% of patients in Cohort D or F
n (%)(a) | Cohort D (n=81) All grade | Grade 3 | Cohort F (n=73) All grade | Grade 3
Diarrhea: 70 (86) | 19 (23) | 62 (85) | 4 (5)
Rash: 42 (52) | 1 (1) | 41 (56) | 0
Paronychia: 23 (28) | 1 (1) | 20 (27) | 1 (1)
Stomatitis: 15 (19) | 1 (1) | 20 (27) | 0
Anemia: 15 (19) | 1 (1) | 19 (26) | 1 (1)
Nausea: 17 (21) | 2 (2) | 8 (11) | 2 (3)
(a)Shown are drug-related AEs of any grade and grade 3 that occurred in >20% of patients from Cohort D or F. Relatedness of AEs to treatment was assessed by the investigator. Drug-related AEs were graded by the investigator based on CTCAE v5.0
Loong et al ASCO 2026
———
[Slide 4]
Sevebertinib: anticipated data
- Resistance mechanisms of sevabertinib
- Follow up on cohort F - PFS and DoR
- Response data from cohort G - CNS cohort
- SOHO-02 initial interim analysis
[SOHO-02 study schema] Screening/baseline -> Treatment period -> Active follow-up -> Long-term follow-up.
Patient population: First-line NSCLC with activating mutation in the HER2 TKD; ECOG PS 0 or 1; Eligible for standard of care; >=1 RECIST v1.1 lesion. R (randomized).
Treatment arms: n=139 BAY 2927088 20 mg BID orally; n=139 Standard of care: Cisplatin/carboplatin + pemetrexed + pembrolizumab. Patients will receive treatment until disease progression per RECIST v1.1, unacceptable toxicity, or any other withdrawal criteria are met.
Primary endpoints: PFS per RECIST v1.1 by BICR.
Secondary endpoints: Overall survival; ORR per RECIST v1.1 by BICR; Safety and tolerability; PFS per RECIST v1.1 by investigator; ORR by investigator; Disease control rate per RECIST v1.1 by BICR and investigator; Duration of response by BICR and investigator; Patient-reported outcomes.
Phase 2 OrigAMI-4 findings discussed by Dr. Renata Ferrarotto from @UTMDAnderson showed 42% BICR-assessed ORR, 63% clinical benefit rate, median PFS of 6.8 months, and median OS of 12.5 months with amivantamab in recurrent/metastatic HNSCC. #DAVALung
OrigAMI-4
[Slide 1]
Cohort 1 (Ami mono) BICR-Assessed ORR (n=102) [OrigAMI-4, HNSCC]
BICR-assessed response, N=102:
Confirmed ORR: 42% (95% CI, 32-52)
Best response, n (%): CR 15 (15); PR 28 (27); SD(a) 36 (35); PD 16 (16); NE 7 (7)
Time to first response, weeks: 6.6 (range, 5.6-36.9)
Clinical benefit rate(b): 63% (95% CI, 53-72)
- Investigator-assessed ORR (47%; 95% CI, 37-57) was consistent with the BICR results. Among participants with >=1 post-baseline disease assessment, 84% experienced tumor shrinkage of target lesions.
[Waterfall + spider plots: Best change from baseline in SoD of target lesions; mDOR: NR; CR/PR/SD/PD/NE]
Burtness B, ASCO, 2026; Burtness B, JCO, 2026
———
[Slide 2]
Cohort 1 (Ami mono): PFS and OS [OrigAMI-4]
Median PFS, 6.8 months(a) (95% CI, 5.2-8.3); landmarks 53% (95% CI, 43-62) at ~6 mo, 23% (95% CI, 13-35) at ~12 mo. Amivantamab.
Median OS, 12.5 months (95% CI, 10.2-16.8); landmarks 78% (95% CI, 69-85) at ~6 mo, 54% (95% CI, 42-64) at ~12 mo. Amivantamab.
Median follow-up: 11.8 months (range, 1.1-21.9). No. at risk: PFS Amivantamab 102, 74, 47, 25, 7, 6, 2, 1, 0; OS Amivantamab 102, 94, 79, 47, 25, 13, 3, 1, 0.
Burtness B, ASCO, 2026
———
[Slide 3]
Cohort 2 (Ami + Pembro) in 1L HPV neg (n=39)
- PD-L1 CPS >= 1
- ORR = 56% (CR: 10%): CPS 1-19: 47%; CPS >= 20: 65%
- mPFS = 7.7 months
- No overlapping/new safety signals
[Waterfall + spider plots: Best change from baseline in SoD of target lesions (%); CR/PR/SD/PD/NE]
Mehra R, MHNCS, 2026
Dr. Khaled Hassan from @ClevelandClinic explored emerging mechanisms of EGFR TKI resistance, highlighting the role of APOBEC/AICDA-mediated mutagenesis and its potential as a therapeutic target to overcome acquired resistance in EGFR-mutant NSCLC. #DAVALung
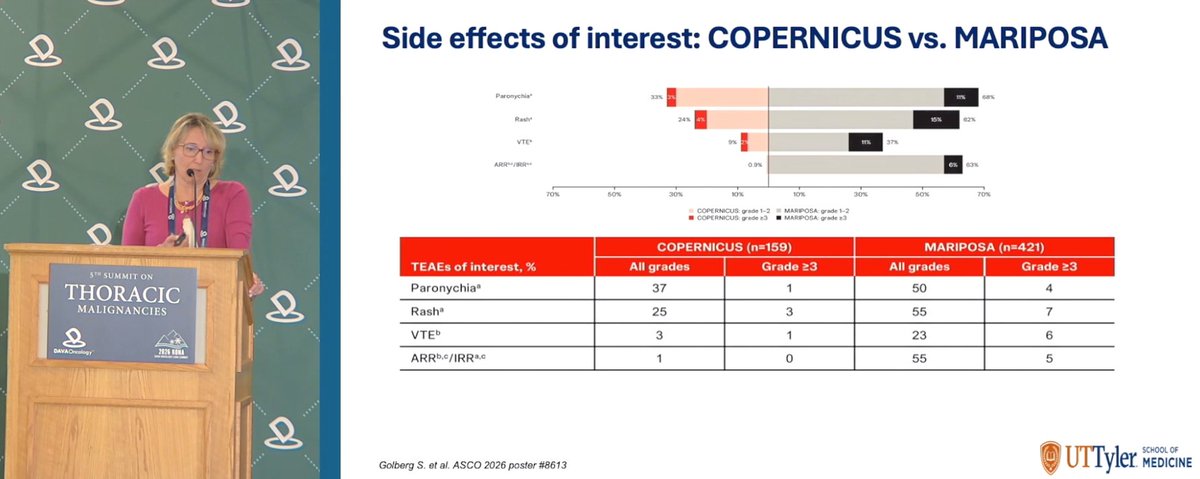
Dr. @ErminiaMassare1 from @uttylersom shared updates on subcutaneous amivantamab plus lazertinib in first-line EGFR-mutated NSCLC, focusing on evidence from MARIPOSA and COPERNICUS. #DAVALung
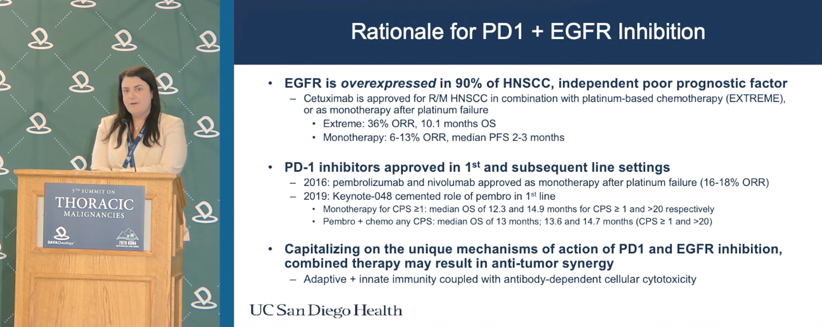
How can EGFR inhibition be paired with PD-1 blockade in head & neck cancer? Dr. Assuntina Sacco of @UCSDHealth shared key data and evolving practice implications at #DAVALung.
EXTREMEFORTIFI-HN01KEYNOTE-048OrigAMI-5
[Slide 1]
Rationale for PD1 + EGFR Inhibition
EGFR is overexpressed in 90% of HNSCC, independent poor prognostic factor. Cetuximab is approved for R/M HNSCC in combination with platinum-based chemotherapy (EXTREME), or as monotherapy after platinum failure. Extreme: 36% ORR, 10.1 months OS. Monotherapy: 6-13% ORR, median PFS 2-3 months.
PD-1 inhibitors approved in 1st and subsequent line settings. 2016: pembrolizumab and nivolumab approved as monotherapy after platinum failure (16-18% ORR). 2019: Keynote-048 cemented role of pembro in 1st line. Monotherapy for CPS >=1: median OS of 12.3 and 14.9 months for CPS >=1 and >20 respectively. Pembro + chemo any CPS: median OS of 13 months; 13.6 and 14.7 months (CPS >=1 and >20).
Capitalizing on the unique mechanisms of action of PD1 and EGFR inhibition, combined therapy may result in anti-tumor synergy. Adaptive + innate immunity coupled with antibody-dependent cellular cytotoxicity.
UC San Diego Health
———
[Slide 2]
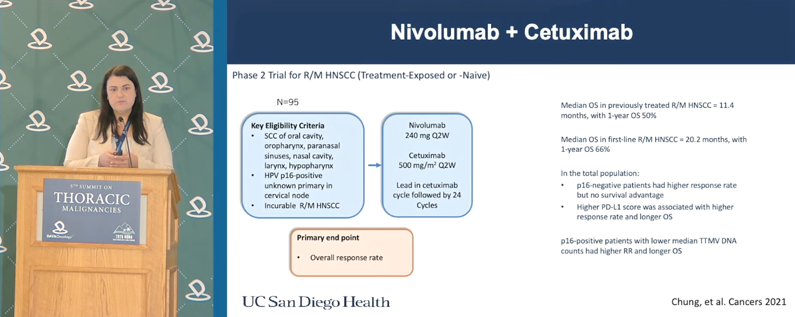
Nivolumab + Cetuximab
Phase 2 Trial for R/M HNSCC (Treatment-Exposed or -Naive). N=95.
Key Eligibility Criteria: SCC of oral cavity, oropharynx, paranasal sinuses, nasal cavity, larynx, hypopharynx; HPV p16-positive unknown primary in cervical node; Incurable R/M HNSCC. Nivolumab 240 mg Q2W; Cetuximab 500 mg/m2 Q2W. Lead in cetuximab cycle followed by 24 Cycles. Primary end point: Overall response rate.
Median OS in previously treated R/M HNSCC = 11.4 months, with 1-year OS 50%. Median OS in first-line R/M HNSCC = 20.2 months, with 1-year OS 66%. In the total population: p16-negative patients had higher response rate but no survival advantage; Higher PD-L1 score was associated with higher response rate and longer OS. p16-positive patients with lower median TTMV DNA counts had higher RR and longer OS.
Chung, et al. Cancers 2021
———
[Slide 3]
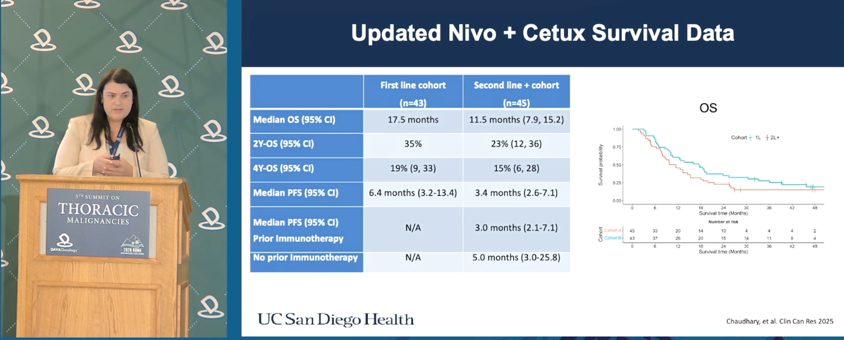
Updated Nivo + Cetux Survival Data
First line cohort (n=43) / Second line + cohort (n=45): Median OS (95% CI) 17.5 months / 11.5 months (7.9, 15.2); 2Y-OS (95% CI) 35% / 23% (12, 36); 4Y-OS (95% CI) 19% (9, 33) / 15% (6, 28); Median PFS (95% CI) 6.4 months (3.2-13.4) / 3.4 months (2.6-7.1); Median PFS (95% CI) Prior Immunotherapy N/A / 3.0 months (2.1-7.1); No prior immunotherapy N/A / 5.0 months (3.0-25.8).
Chaudhary, et al. Clin Can Res 2025
———
[Slide 4]
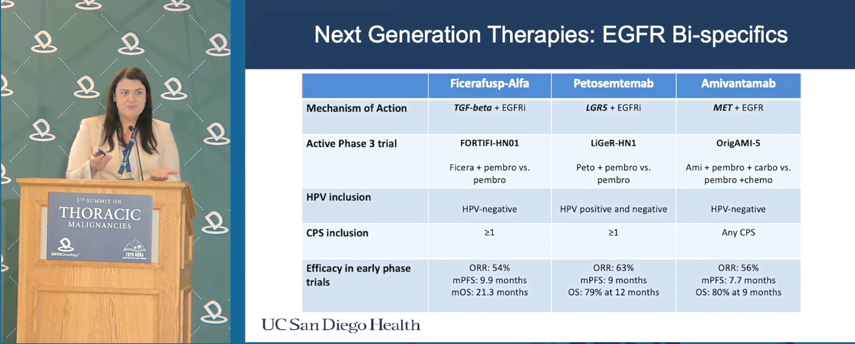
Next Generation Therapies: EGFR Bi-specifics
Ficerafusp-Alfa / Petosemtemab / Amivantamab:
Mechanism of Action: TGF-beta + EGFRi / LGR5 + EGFRi / MET + EGFR.
Active Phase 3 trial: FORTIFI-HN01 (Ficera + pembro vs. pembro) / LiGeR-HN1 (Peto + pembro vs. pembro) / OrigAMI-5 (Ami + pembro + carbo vs. pembro + chemo).
HPV inclusion: HPV-negative / HPV positive and negative / HPV-negative.
CPS inclusion: >=1 / >=1 / Any CPS.
Efficacy in early phase trials: ORR: 54%, mPFS: 9.9 months, mOS: 21.3 months / ORR: 63%, mPFS: 9 months, OS: 79% at 12 months / ORR: 56%, mPFS: 7.7 months, OS: 80% at 9 months.
UC San Diego Health
Clinical data for petosemtamab, an EGFR/LGR5 bispecific, was discussed by @eevokes from @UChicagoMed, including an ORR of 36%, median time to response of 1.9 months, median duration of response of 6.7 months, and median OS of 11.4 months in recurrent/metastatic HNSCC. #DAVALung
[Slide 1]
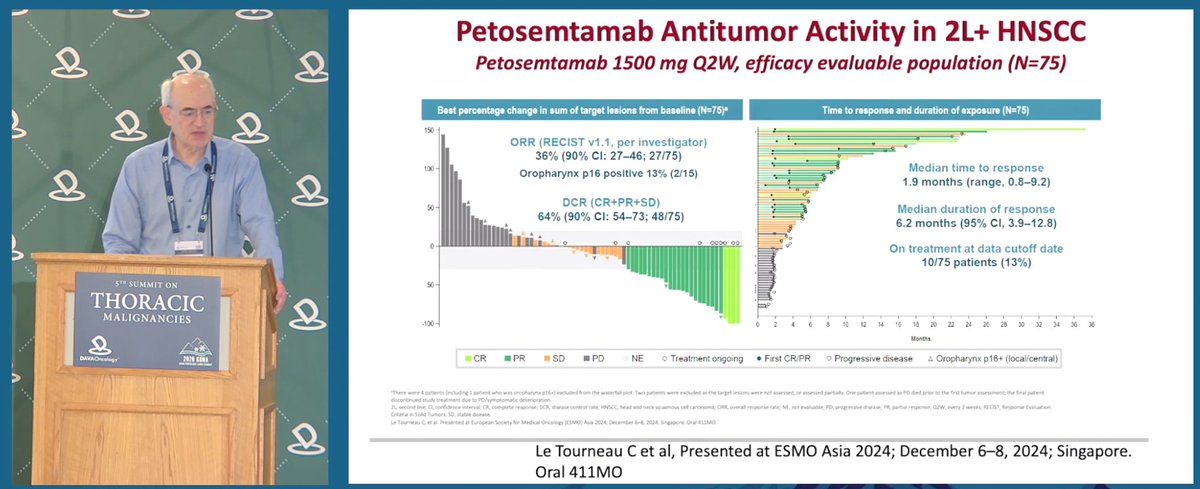
Petosemtamab Antitumor Activity in 2L+ HNSCC
Petosemtamab 1500 mg Q2W, efficacy evaluable population (N=75)
Best percentage change in sum of target lesions from baseline (N=75):
ORR (RECIST v1.1, per investigator) 36% (90% CI: 27-46; 27/75); Oropharynx p16 positive 13% (2/15)
DCR (CR+PR+SD) 64% (90% CI: 54-73; 48/75)
Time to response and duration of exposure (N=75):
Median time to response 1.9 months (range, 0.8-9.2)
Median duration of response 6.2 months (95% CI, 3.9-12.8)
On treatment at data cutoff date 10/75 patients (13%)
Legend: CR, PR, SD, PD, NE, Treatment ongoing, First CR/PR, Progressive disease, Oropharynx p16+ (local/central)
Le Tourneau C et al, Presented at ESMO Asia 2024; December 6-8, 2024; Singapore. Oral 411MO
———
[Slide 2]
Petosemtamab Antitumor Activity in 2L+ HNSCC
Petosemtamab 1500 mg Q2W, efficacy evaluable population (N=75)
Median PFS 4.9 months (95% CI: 3.2-5.4); 11/75 censored
Median OS 11.4 months (95% CI: 7.2-15.9); 46/75 patients died, 29/75 censored
- In the single-arm cohort, initially presented at AACR 2023, among 48 evaluable patients, the median DOR, PFS, and OS were 6.7, 5.2, and 12.5 months, respectively
Le Tourneau C et al, Presented at ESMO Asia 2024; December 6-8, 2024; Singapore. Oral 411MO. Cohen et al. Cancer Res 2023;83 (8 suppl): Abstract CT012.
———
[Slide 3]
Efficacy
Best percent change in sum of target lesions from baseline (n=43):
Confirmed ORR (RECIST v1.1, per investigator) 63% (27/43, 95% CI: 49-75) [6 CR, 21 PR]
p16 positive 4/8 (50%); p16 negative 23/35 (66%); CPS 1-19 8/17 (47%); CPS >=20 19/26 (73%)
Time to response and duration (n=43):
Median time to response 1.9 months (range: 1.6-9.1)
Median duration of response Not reached (95% CI: 7.4-NC)
14 responders were continuing therapy at data cutoff
Best overall response: CR, PR, SD, PD, NE. EGFR H-Score and PD-L1 CPS shown per patient.
Van Herpen CML et al, Presented at ASCO 2025; May 30-June 3, 2025; Chicago, IL, USA. Poster 6024
Dr. Timothy Burns @OSUCCC_James shared insight on expanding landscape of MET-targeted ADCs in NSCLC, covering FDA-approved Teliso-V and investigational Temab-A, with a focus on efficacy, toxicity, and future directions for MET-directed therapy. #DAVALung
LUMINOSITY
[Slide 1]
MET ADCs: Telisotuzumab vedotin (Teliso-V) The LUMINOSITY STUDY
ORR: c-Met High (n=78) 34.6% (24.5-46.2); c-Met Intermediate (n=83) 22.9% (14.1-33.4); c-Met OE Total (N=161) 28.6% (21.7-36.2).
Number of responders 27 / 19 / 46. Median DOR, months [95% CI] 9.0 [4.2, 13.0] / 7.2 [5.3, 11.5] / 8.3 [5.6, 11.3]. DOR >=6 months, n (%) 17 (63.0) / 9 (47.4) / 26 (56.5).
Best Reductions in Target Lesions per ICR (n=147).
Progression-Free Survival: Median, mo [95% CI] c-Met High 5.5 [4.1, 8.3]; c-Met Intermediate 6.0 [4.5, 8.1]; c-Met OE Total 5.7 [4.6, 6.9]. Events, n (%) 55 (70.5) / 57 (68.7) / 112 (69.6).
Overall Survival: Median, mo [95% CI] c-Met High 14.6 [9.2, 25.6]; c-Met Intermediate 14.2 [9.6, 16.6]; c-Met OE Total 14.5 [9.9, 15.6]. Events, n (%) 47 (60.3) / 55 (66.3) / 102 (63.4).
66 (41.0%) of patients received a subsequent systemic therapy after Teliso-V discontinuation.
DCR was 60.3% (c-Met high), 57.8% (c-Met intermediate), and 59.0% (c-Met OE total).
c-Met protein overexpression in nonsquamous EGFR wildtype NSCLC was defined as >=25% tumor cells with 3+ staining (high [>=50% 3+]; intermediate [>=25%-<50%]).
Camidge et al. ASCO 2024; JCO 2024
———
[Slide 2]
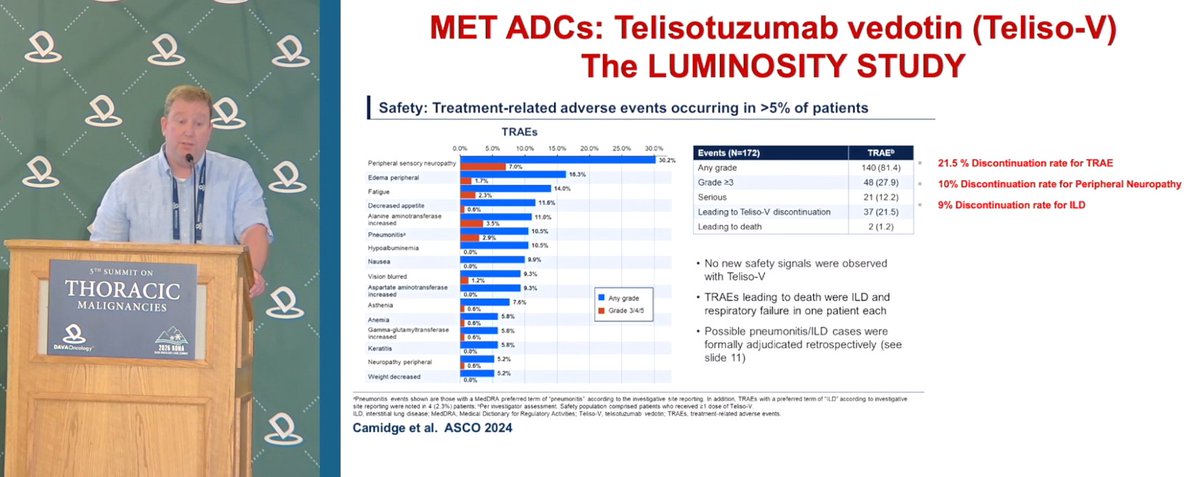
MET ADCs: Telisotuzumab vedotin (Teliso-V) The LUMINOSITY STUDY
Safety: Treatment-related adverse events occurring in >5% of patients (TRAEs). Any grade / Grade 3/4/5: Peripheral sensory neuropathy 30.2% / 7.0%; Edema peripheral 16.3% / 1.7%; Fatigue 14.0% / 2.3%; Decreased appetite 11.6% / 0.6%; Alanine aminotransferase increased 11.0% / 3.5%; Pneumonitis 10.5% / 2.9%; Hypoalbuminemia 10.5% / 0.0%; Nausea 9.9% / 0.0%; Vision blurred 9.3% / 1.2%; Aspartate aminotransferase increased 9.3% / 0.0%; Asthenia 7.6% / 0.6%; Anemia 5.8% / 0.6%; Gamma-glutamyltransferase increased 5.8% / 0.6%; Keratitis 5.8% / 0.0%; Neuropathy peripheral 5.2% / 0.6%; Weight decreased 5.2% / 0.0%.
Events (N=172) TRAE: Any grade 140 (81.4); Grade >=3 48 (27.9); Serious 21 (12.2); Leading to Teliso-V discontinuation 37 (21.5); Leading to death 2 (1.2).
21.5% Discontinuation rate for TRAE; 10% Discontinuation rate for Peripheral Neuropathy; 9% Discontinuation rate for ILD.
No new safety signals were observed with Teliso-V. TRAEs leading to death were ILD and respiratory failure in one patient each. Possible pneumonitis/ILD cases were formally adjudicated retrospectively (see slide 11).
Camidge et al. ASCO 2024
———
[Slide 3]
MET ADCs: Telisotuzumab adizutecan (Temab-A, ABBV-400)
Temab-A Mechanism of Action: Validated c-Met targeted antibody (telisotuzumab); Potent Top1i payload (adizutecan); Stable linker (minimizes free-payload toxicity). Antitumor effect of Temab-A does not rely on c-Met signaling, unlike c-Met protein-targeting TKIs and mAbs.
3L+ EGFR wild type NSCLC ORR by c-Met Protein Cutoff by IHC: All patients 47.9% (23/48); Patients with IHC results 48.9% (23/47); >=50% cells >=2+ 51.4% (19/37); <25% cells 2+ 40.0% (4/10); >=25% cells 3+ 60.0% (9/15); <25% cells 3+ 43.8% (14/32); >=50% cells 3+ 77.8% (7/9); <50% cells 3+ 42.1% (16/38).
3L+ EGFR mutant NSCLC: All patients with post-baseline data (n=38) experienced decrease in tumor burden. Responses occurred irrespective of EGFR L858R alterations, exon 19 deletions or TKI resistance mutations, including T790M and C797S. Responses seen across known EGFR TKI resistance mechanisms: All patients 63%; >=25% cells 2+ 79%; <25% 2+ 33%; >=25% cells 3+ 68%; <25% cells 3+ 60%.
De Miguel et al. ESMO 2024; Camidge et al. ASCO 2025
———
[Slide 4]
MET ADCs: Telisotuzumab adizutecan (Temab-A, ABBV-400)
The most common any-grade TEAEs were gastrointestinal (83%) and hematological (83%). TEAEs of interest: Adjudicated any-grade pneumonitis/ILD n=3, 7% (grade >=3: n=1; 2%); Alopecia n=5, 12% (grade >=3: n=0); Stomatitis n=5, 12% (grade >=3: n=0). 5 (12%) patients experienced fatal TEAEs; 1 death was considered related to Temab-A (pneumonitis). 15/26 (58%) of patients who reported >=1 event of anemia did not require transfusions. 8/17 (47%) of patients who reported >=1 event of neutropenia did not require G-CSF.
TEAEs, n (%) EGFR MT NSCLC (N=41) Any Grade / Grade >=3: Any TEAE 41 (100) / 32 (78); Gastrointestinal 34 (83) / 3 (7); Hematological 34 (83) / 21 (51); Anemia 26 (63) / 13 (32); Neutropenia 17 (41) / 12 (29); Nausea 27 (66) / 1 (2); Vomiting 16 (39) / 3 (7); Decreased appetite 14 (34) / 1 (2); Fatigue 13 (13) / 1 (2); Constipation 13 (32) / -; TEAE leading to dose interruption 31 (76) / 21 (51); TEAE leading to dose reduction 20 (49) / 14 (34); TEAE leading to discontinuation 10 (24) / 6 (15); Related to Temab-A 6 (15) / 3 (7).
Previously treated MET amplified NSCLC Confirmed Objective Response Rate (pooled by dose): NSCLC 69% (20/29); GEA 71% (10/14); CRC 27% (6/22); Cholangio/bile duct 50% (4/8); Other 22%; Total 46% (46/100).
Median DOR, months (95% CI) Total (n=100) 10.9 (8.1-13.9); NSCLC (n=29) 13.0 (7.0-22.1). Median PFS, months (95% CI) Total 8.5 (5.5-11.1); NSCLC 11.0 (7.7-15.1). Median OS, months (95% CI) Total 19.6 (14.5-NE); NSCLC NR.
Camidge et al. ASCO 2025; Murciano-Goroff YR, et al. ESMO 2025; NCT05029882
Young-onset lung cancer (≤50) often shows more actionable drivers (EGFR/ALK/ROS1/RET/HER2) and longer survival. @maraantonoff (@UTMDAnderson) explains why biology—not age alone—should guide surgical decisions. #DAVALung
[Slide 1]
Targeted therapy revolution
Longer survival created new opportunities for local therapy
Historical era: Chemotherapy dominant - Limited efficacy and toxicity
Biomarker discovery: Understanding tumor biology - Identification of actionable drivers
Targeted therapies: Precision medicines emerge - Higher response rates and better tolerability
Combination era: Immunotherapy + targeted agents - Synergistic approaches improve depth and durability
Modern era: Personalized, multi-line treatment strategies - Prolonged survival and improved quality of life
Advances in targeted therapies have fundamentally transformed outcomes for patients with molecularly defined lung cancers--turning a once uniformly poor prognosis into a landscape of meaningful, durable survival.
———
[Slide 2]
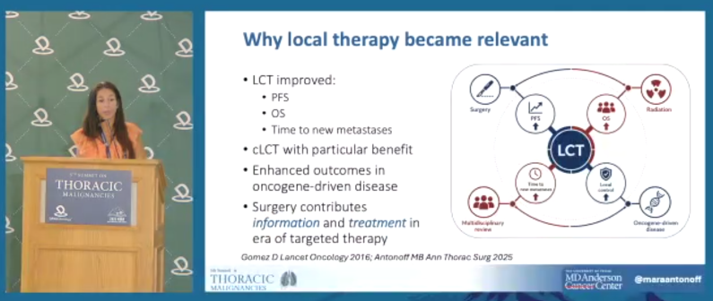
Why local therapy became relevant
- LCT improved: PFS; OS; Time to new metastases
- cLCT with particular benefit
- Enhanced outcomes in oncogene-driven disease
- Surgery contributes information and treatment in era of targeted therapy
[Diagram: LCT central; Surgery, Radiation, Oncogene-driven disease, Multidisciplinary review, Time to new metastases, Local control, OS, PFS]
Gomez D Lancet Oncology 2016; Antonoff MB Ann Thorac Surg 2025
———
[Slide 3]
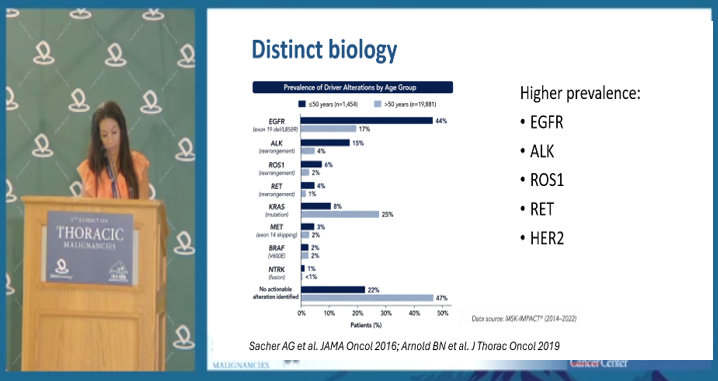
Distinct biology
Prevalence of Driver Alterations by Age Group (<=50 years n=1,454; >50 years n=19,881)
EGFR (exon 19-del/L858R): 44% (<=50) / 17% (>50)
ALK (rearrangement): 15% / 4%
ROS1 (rearrangement): 6% / 2%
RET (rearrangement): 4% / 2%
KRAS (mutation): 8% / 25%
MET (exon 14 skipping): 2% / 3%
BRAF (V600E): 2% / 2%
NTRK (fusion): <1% / <1%
No actionable alteration identified: 22% / 47%
Higher prevalence: EGFR, ALK, ROS1, RET, HER2
Data source: MSK-IMPACT (2014-2022)
Sacher AG et al. JAMA Oncol 2016; Arnold BN et al. J Thorac Oncol 2019
———
[Slide 4]
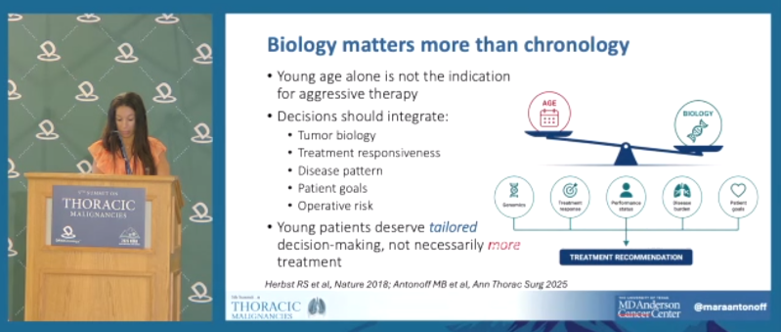
Biology matters more than chronology
- Young age alone is not the indication for aggressive therapy
- Decisions should integrate: Tumor biology; Treatment responsiveness; Disease pattern; Patient goals; Operative risk
- Young patients deserve tailored decision-making, not necessarily more treatment
[Balance diagram: AGE vs BIOLOGY; Genomics, Treatment response, Performance status, Disease burden, Patient goals -> Treatment recommendation]
Herbst RS et al, Nature 2018; Antonoff MB et al, Ann Thorac Surg 2025
The evolving role of patritumab deruxtecan in EGFR-mutated NSCLC was discussed by @JuliaRotow from @DanaFarber, with a review of updated HERTHENA-Lung02 data on efficacy, intracranial activity, overall survival, and safety. #DAVALung
HERTHENA-Lung01HERTHENA-Lung02
[Slide 1]
HER3-DXd significantly reduced the risk of disease progression (by BICR per RECIST 1.1) or death vs PBC
HR: 0.77 (95% CI, 0.63-0.94); P=.011
Median PFS (95% CI), months: HER3-DXd 5.8 (5.5-6.8); PBC 5.4 (5.0-5.6)
Probability of PFS (95% CI) at 9 months: 29% (23%-35%) vs 19% (14%-25%)
HER3-DXd (N=293); PBC (N=293)
Mok et al ASCO 2025
Dana-Farber Cancer Institute
———
[Slide 2]
HER3-DXd demonstrated intracranial activity
Evaluation in patients with brain metastases at baseline according to CNS BICR (Patritumab Deruxtecan, HERTHENA-Lung02)
Intracranial response by CNS BICR per CNS RECIST | HER3-DXd (N=105) | PBC (N=95)
Confirmed intracranial ORR (95% CI), % | 19.0 (12.0-27.9) | 11.6 (5.9-19.8)
Best overall intracranial response: CR 13 (12.4) / 4 (4.2); PR 7 (6.7) / 7 (7.4); SD 52 (49.5) / 47 (49.5); PD 27 (25.7) / 26 (27.4); NE 6 (5.7) / 11 (11.6)
BOR to be confirmed, n (%) 2 (1.9) / 0
Intracranial DCR (95% CI), % 68.6 (58.8-77.3) / 61.1 (50.5-70.9)
Median intracranial TTR (range), mo 2.1 (1.2-6.9) / 2.6 (1.2-4.7)
Median intracranial DOR (95% CI), mo 4.5 (4.1-NE) / 4.2 (2.4-NE)
Prior radiation to the brain, n (%) 39 (37.1) / 36 (37.9)
HR for intracranial progression: 0.75 (95% CI, 0.53-1.06)
Median intracranial PFS (95% CI), months: HER3-DXd 5.4 (4.0-5.9); PBC 4.2 (2.8-5.0)
Mok et al ASCO 2025
Dana-Farber Cancer Institute
———
[Slide 3]
The safety profile of HER3-DXd was generally manageable and was consistent with previously reported trials
TEAEs Occurring in >=10% of Patients. HER3-DXd (n=290) vs PBC (n=280):
Nausea 54% / 42%; Thrombocytopenia (grouped PT) 22% grade 1-2, 30% grade >=3 / 8% grade >=3, 19%; Fatigue 43% / 39%; Neutropenia (grouped PT) 15%+26% / 23%+23%; Alopecia 37% / 7%; Constipation 33% / 34%; Decreased appetite 29% / 23%; Anemia 23%+7% / 16%+30%; Leukopenia 15%+11% / 10%+21%; AST increased 24% / 21%; Diarrhea 23% / 13%; Vomiting 20% / 12%; ALT increased 21% / 21%; Hypokalemia 12%+7% / 5%; Asthenia 13% / 14%; Headache 13% / 11%; Cough 13% / 11%; Lymphopenia 8%+5% / 3%; Malaise 10% / 5%; Weight decreased 9% / 7%; Pyrexia 10% / 10%; Hypoalbuminemia 10% / 4%; Rash 6% / 10%
- Observed hematologic toxicities generally occurred early (cycle 1 or 2), were transient, and in most instances were not associated with clinical sequelae
- Each arm had 1 grade >=3 bleeding event associated with grade >=3 platelet count decreased
ILD Adjudication, n (%): HER3-DXd (n=290) Total ILD 28 (9.7); Adjudicated as ILD 15 (5.2); Adjudicated as treatment-related ILD 14 (4.8). PBC (n=280) Total ILD 2 (0.7); Adjudicated as ILD 0; treatment-related ILD 0
Mok et al ASCO 2025
Dana-Farber Cancer Institute
———
[Slide 4]
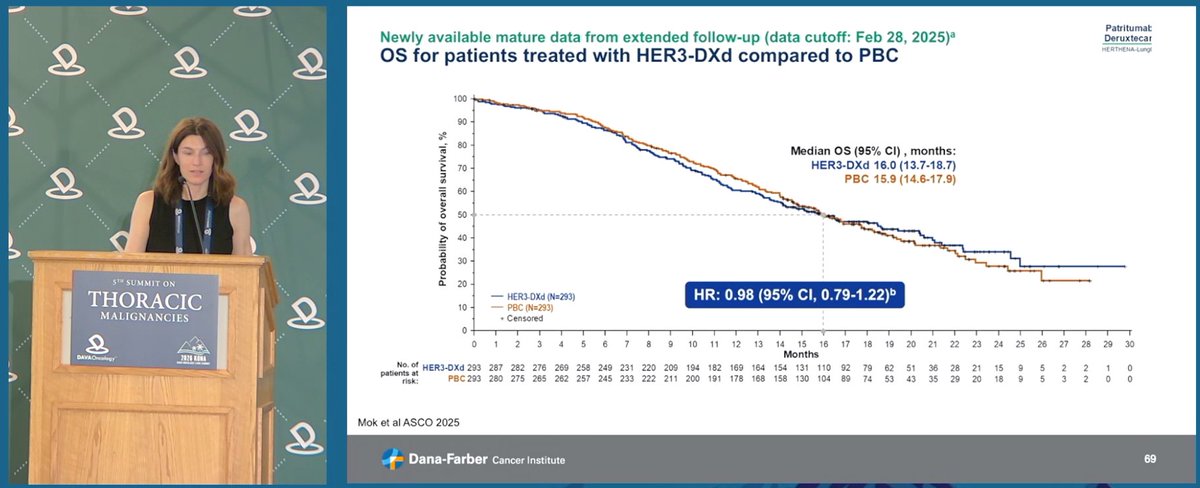
Newly available mature data from extended follow-up (data cutoff: Feb 28, 2025)
OS for patients treated with HER3-DXd compared to PBC
Median OS (95% CI), months: HER3-DXd 16.0 (13.7-18.7); PBC 15.9 (14.6-17.9)
HR: 0.98 (95% CI, 0.79-1.22)
HER3-DXd (N=293); PBC (N=293)
Mok et al ASCO 2025
Dana-Farber Cancer Institute
Biology-guided RT: Dr. @HenryParkMD (@YaleMed) reviewed RefleXion X1/SCINTIX therapy using PET signal for real-time RT tracking, approved in lung/bone, and an endometrial adenocarcinoma lung met case with 42% PTV reduction. #DAVALung
[Slide 1]
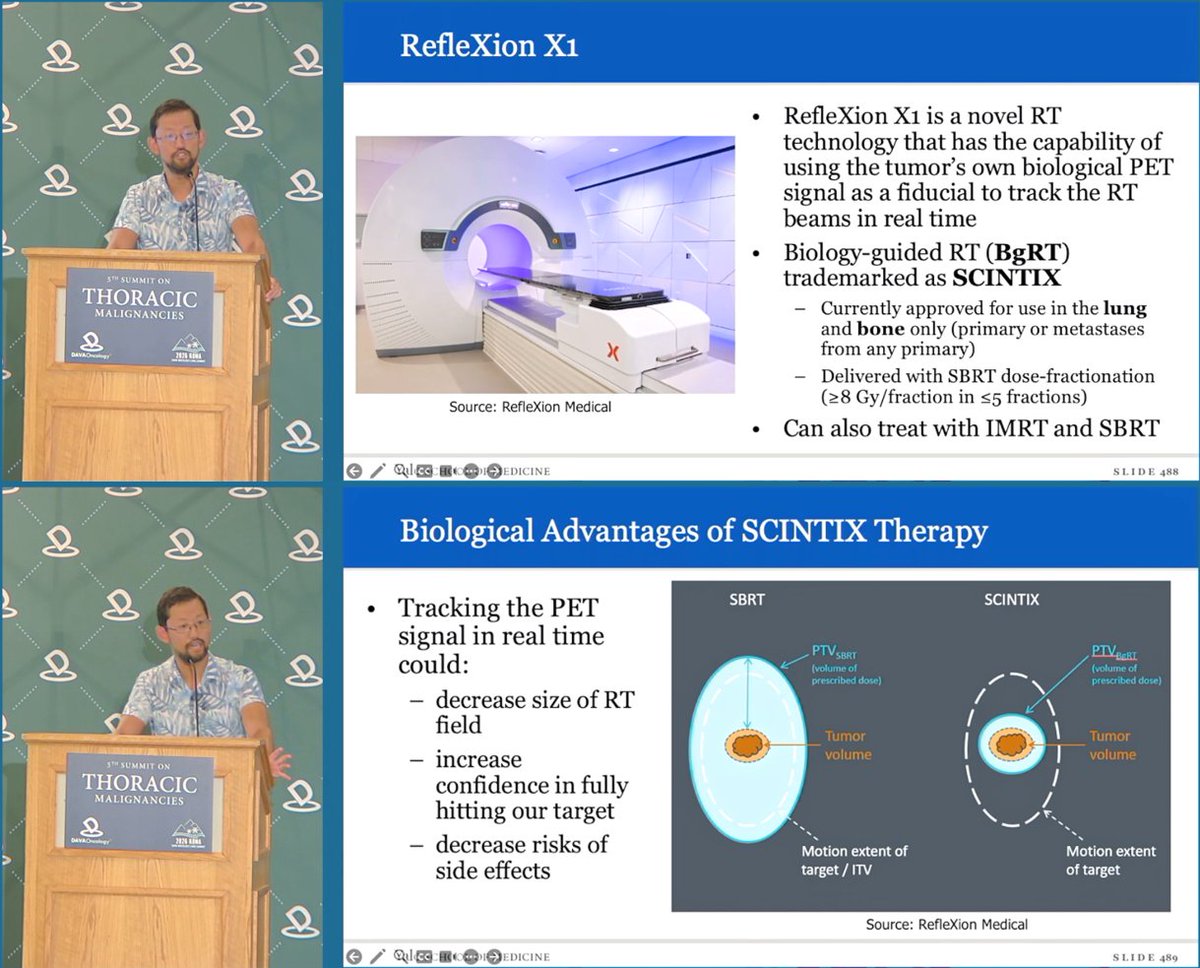
RefleXion X1
• RefleXion X1 is a novel RT technology that has the capability of using the tumor's own biological PET signal as a fiducial to track the RT beams in real time
• Biology-guided RT (BgRT) trademarked as SCINTIX
– Currently approved for use in the lung and bone only (primary or metastases from any primary)
– Delivered with SBRT dose-fractionation (≥8 Gy/fraction in ≤5 fractions)
• Can also treat with IMRT and SBRT
Source: RefleXion Medical
Biological Advantages of SCINTIX Therapy
• Tracking the PET signal in real time could:
– decrease size of RT field
– increase confidence in fully hitting our target
– decrease risks of side effects
SBRT vs SCINTIX: PTV(SBRT) vs PTV(BgRT); Tumor volume; Motion extent of target / ITV. Source: RefleXion Medical
———
[Slide 2]
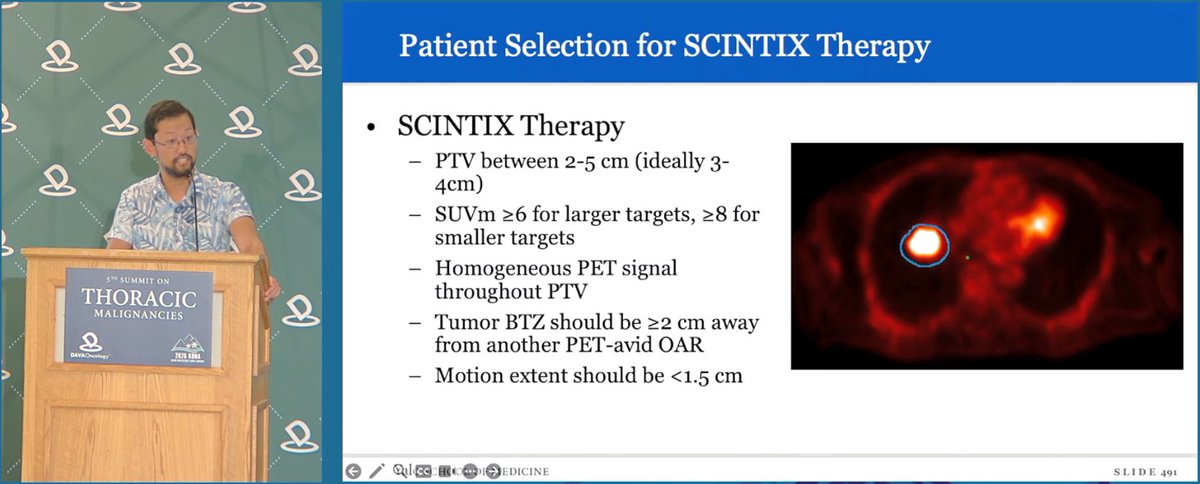
Patient Selection for SCINTIX Therapy
• SCINTIX Therapy
– PTV between 2-5 cm (ideally 3-4cm)
– SUVm ≥6 for larger targets, ≥8 for smaller targets
– Homogeneous PET signal throughout PTV
– Tumor BTZ should be ≥2 cm away from another PET-avid OAR
– Motion extent should be <1.5 cm
———
[Slide 3]
Increased Tracking Confidence and 42% PTV Reduction
Dose distribution comparison (solid: delivered, dotted: planned).
Target coverage in post-treatment bDVH review: PTV_BGRT 94.98% at 1177 cGy; Volume (%) vs Dose (cGy).
———
[Slide 4]
Vision for SCINTIX Therapy
• Treat smaller and less avid lesions with higher resolution on next-generation X2
• Expand indications beyond lung and bone targets
• Treat multiple metastatic sites for complete metastatic ablation for stage IV cancers of all types in conjunction with immunotherapy and targeted therapy
• Novel radioisotopes beyond FDG
R01: Deep Learning-Based PET Denoising Algorithms
Development and Clinical Translation of Advanced PET Imaging for Real-Time Biology-Guided Radiotherapy
Radiation Oncology team receives NIH Academic Industry Partnership (AIP) R01 Grant. Notice of Award, National Cancer Institute; Recipient: Yale Univ, 150 Munson St, New Haven CT 06511; Award Number 1R01CA304967-01A1; Federal Award Date 06/30/2026. Principal Investigators: David J. Carlson PhD, Henry S. Park MD MPH, Chi Liu PhD; Co-Investigators: Huaxiao Chen, Emily Draeger PhD, Timothy Robinson MD PhD.
Fig. 8: Recovery of image quality of RefleXion PET of a lung cancer patient to iterative-reconstructed diagnostic PET using various deep learning methods (Diagnostic PET, RefleXion PET, U-Net, Diffusion; NTS=3.9, 5.4, 6.7).
Fig. 9: MDPET results (high-count ground truth, averaged image w/o registration, proposed MDPET reconstruction before and after denoising).
Theme · 8 talks
KRAS & RAS-Targeting Agents
G12C, G12D, and RAS(ON/OFF) inhibitors — adagrasib, olomorasib, divarasib, zoldonrasib — including perioperative trials.
KRYSTAL-7 tests adagrasib + pembrolizumab in 1L KRAS G12C NSCLC, showing ORR 44%, mDOR 26.3m, mPFS 11m and mOS 18.3m, while key questions remain on safety, PD-L1, chemo need, CNS activity and co-mutations. Update from Dr. @Jsabari@nyulangone at #DAVALung
KRYSTAL-7
[Slide 1]
KRYSTAL-7 design: phase 2 (NCT04613596)
• Cohort 1a: Patients with PD-L1 Tumor Proportion Score (TPS) <1% given adagrasib (400 mg twice daily) + pembrolizumab.
• Cohort 1b: Patients with PD-L1 TPS <1% given adagrasib monotherapy (600 mg twice daily).
• Cohort 2: Patients with PD-L1 TPS ≥1% given adagrasib (400 mg twice daily) + pembrolizumab.
1L advanced KRAS G12C-mutated NSCLC
Subgroup analysis by PD-L1 expression
Key eligibility criteria
• Advanced, unresectable or metastatic NSCLC with KRAS G12C mutation
• No prior systemic therapy for locally advanced/metastatic disease
• Known PD-L1 TPS score (local or central testing)
• Treated, neurologically stable brain metastases allowed
ADA 400 mg PO BID + PEMBRO 200 mg IV Q3W
Primary endpoint
• ORR per investigator assessment (RECIST v1.1)
Secondary endpoints
• DOR and PFS per investigator assessment
• OS
• Safety
Exploratory analysis
• Efficacy by ADA dose reductions due to AEs
———
[Slide 2]
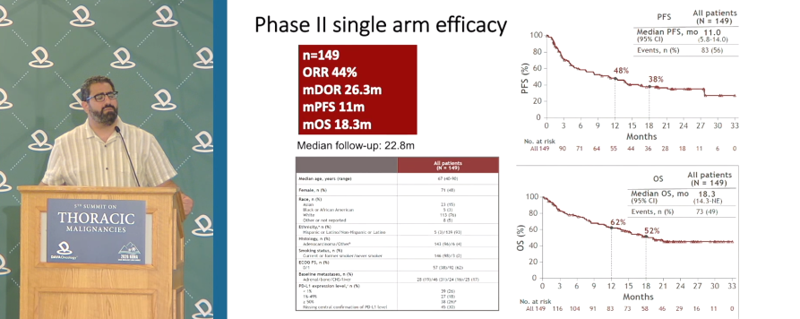
Phase II single arm efficacy
n=149
ORR 44%
mDOR 26.3m
mPFS 11m
mOS 18.3m
Median follow-up: 22.8m
PFS — All patients (N=149): Median PFS, mo 11.0 (95% CI 5.8–14.0); events n (%) 83 (56); 48% at ~12 mo, 38% later
OS — All patients (N=149): Median OS, mo 18.3 (95% CI 14.3–NE); events n (%) 73 (49); 62%, 52%
Baseline table (All patients N=149): Median age; Female 71 (48); Race; PD-L1 expression subgroups
———
[Slide 3]
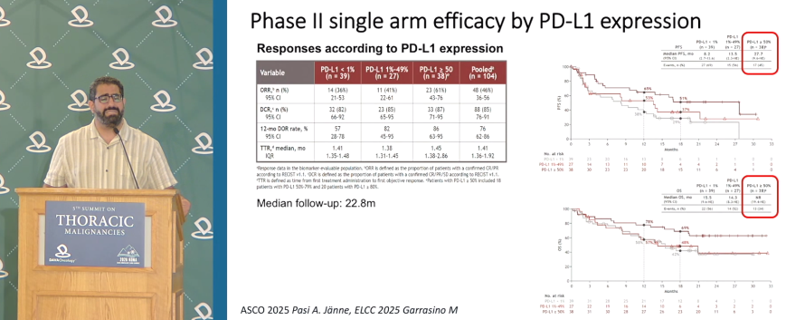
Phase II single arm efficacy by PD-L1 expression
Responses according to PD-L1 expression
Variable | PD-L1 <1% (n=39) | PD-L1 1–49% (n=27) | PD-L1 ≥50% (n=38) | Pooled (n=104)
ORR, n (%): 14 (36%) | 11 (41%) | 23 (61%) | 48 (46%)
95% CI: 21–53 | 22–61 | 44–76 | 36–56
DCR, n (%): 32 (82%) | 23 (85%) | 33 (87%) | 88 (85%)
95% CI: 66–92 | 65–95 | 71–95 | 76–91
12-mo DOR rate, %: 73 | 79 | 76 | 76
95% CI: 28–78 | 43–96 | 26–91 | 51–89
TTR, median, mo: 1.45 | 1.38 | 1.45 | 1.41
IQR: 1.31–1.45 | 1.31–1.45 | 1.31–2.66 | 1.36–1.92
Median follow-up: 22.8m
ASCO 2025 Pasi A. Jänne, ELCC 2025 Garrasino M
———
[Slide 4]
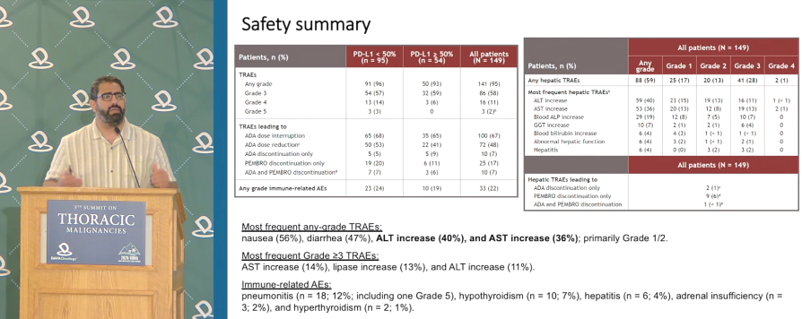
Safety summary
Patients, n (%) | PD-L1 <50% (n=95) | PD-L1 ≥50% (n=54) | All patients (N=149)
TRAEs
Any grade: 91 (96) | 50 (93) | 141 (95)
Grade 3: 54 (57) | 32 (59) | 86 (58)
Grade 4: 13 (14) | 3 (6) | 16 (11)
Grade 5: 3 (3) | 0 | 3 (2)
TRAEs leading to:
ADA dose interruption: 65 (68) | 35 (65) | 100 (67)
ADA dose reduction: 50 (53) | 22 (41) | 72 (48)
ADA discontinuation only: 9 (9) | 4 (7) | 13 (9)
PEMBRO discontinuation only: 19 (20) | 6 (11) | 25 (17)
ADA and PEMBRO discontinuation: 7 (7) | 3 (6) | 10 (7)
Any grade immune-related AEs: 23 (24) | 10 (19) | 33 (22)
Hepatic TRAEs (All patients N=149) by grade:
Any hepatic TRAEs: 88 (59) any grade; 25 (17) G1; 20 (13) G2; 41 (28) G3; 2 (1) G4
Most frequent hepatic TRAEs: ALT increase 59 (40); AST increase 53 (36); Blood ALP increase 20 (13); GGT increase 10 (7); Blood bilirubin increase 6 (4); Abnormal hepatic function 6 (4); Hepatitis 6 (4)
Hepatic TRAEs leading to: ADA discontinuation only 2 (1); PEMBRO discontinuation only 9 (6); ADA and PEMBRO discontinuation 1 (1)
Most frequent any-grade TRAEs: nausea (56%), diarrhea (47%), ALT increase (40%), and AST increase (36%); primarily Grade 1/2.
Most frequent Grade ≥3 TRAEs: AST increase (14%), lipase increase (13%), and ALT increase (11%).
Immune-related AEs: pneumonitis (n=18; 12%; including one Grade 5), hypothyroidism (n=10; 7%), hepatitis (n=6; 4%), adrenal insufficiency (n=3; 2%), and hyperthyroidism (n=2; 1%).
Real-world data from Dr. Michael Kelley @DukeHealth: in the VA experience, sotorasib outcomes were mPFS 6.0 months and mOS 12.0 months. Dose reduction of sotorasib due to toxicity was common, but was not associated with worse PFS or OS outcomes.
[Slide 1]
Methods
- Patients identified from VA Corporate Data Warehouse (CDW) and National Precision Oncology Program (NPOP) database
- Data cutoff: April 4, 2023
- Manual chart review used for unstructured data, including tumor response
- AEs leading to drug interruption, dose reduction or discontinuation were captured
- PFS and OS measured from initiation of sotorasib
- Chi-square proportional-hazards model used for survival analyses
- Chi-square and logistic regression used for variables impacting toxicity
- Analyses performed using R
Zhou KI et al. JTO Clin Res Rep. 2024; PMID: 38746048
———
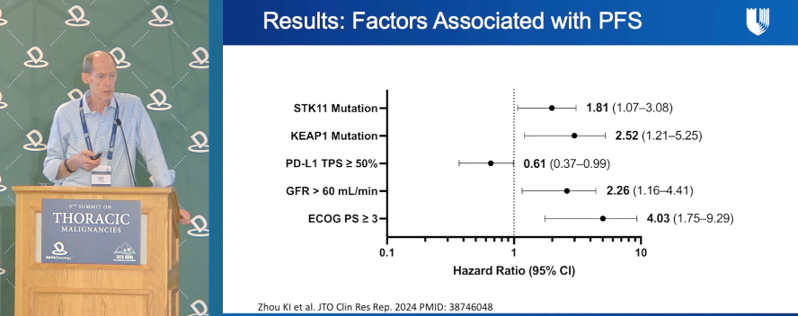
[Slide 2]
Results: Factors Associated with PFS
Forest plot of Hazard Ratio (95% CI):
- STK11 Mutation: 1.81 (1.07-3.08)
- KEAP1 Mutation: 2.52 (1.21-5.25)
- PD-L1 TPS >= 50%: 0.61 (0.37-0.99)
- GFR > 60 mL/min: 2.26 (1.16-4.41)
- ECOG PS >= 3: 4.03 (1.75-9.29)
X-axis: Hazard Ratio (95% CI), 0.1 to 10
Zhou KI et al. JTO Clin Res Rep. 2024 PMID: 38746048
———
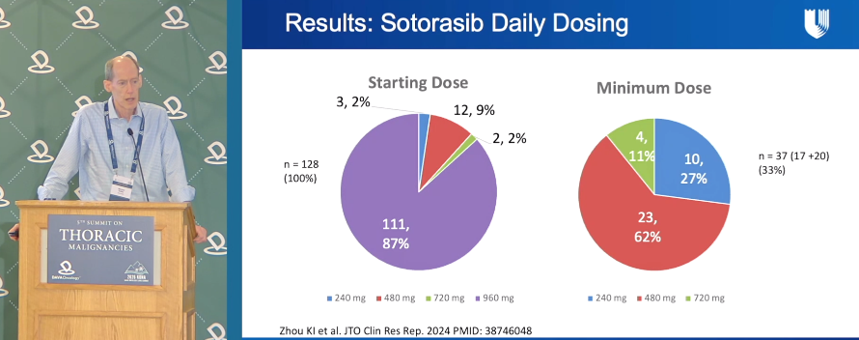
[Slide 3]
Results: Sotorasib Daily Dosing
Starting Dose (n = 128, 100%):
- 240 mg: 3, 2%
- 480 mg: 12, 9%
- 720 mg: 2, 2%
- 960 mg: 111, 87%
Minimum Dose (n = 37 (17 +20), 33%):
- 240 mg: 10, 27%
- 480 mg: 23, 62%
- 720 mg: 4, 11%
Zhou KI et al. JTO Clin Res Rep. 2024 PMID: 38746048
———
[Slide 4]
Results: Dose Reduction and Outcomes
Progression-Free Survival: HR 0.60 (95% CI 0.38-0.97). Curves: Not dose reduced vs Dose reduced. Y-axis Survival probability; X-axis Months since start of drug.
Number at risk (PFS): Not dose reduced (n=91): 30, 14, 3, 1; Dose reduced (n=37): 22, 10, 2, 0
Overall Survival: HR 0.42 (95% CI 0.22-0.80). Curves: Not dose reduced vs Dose reduced.
Number at risk (OS): Not dose reduced (n=91): 41, 22, 9, 1; Dose reduced (n=37): 29, 18, 6, 1
Zhou KI et al. JTO Clin Res Rep. 2024 PMID: 38746048
Dr. Timothy Burns @OSUCCC_James highlights olomorasib in KRAS G12C-mutant NSCLC with untreated brain metastases: CNS disease is common (23.4-41.7%), durability remains a key need, and olomorasib showed promising intracranial activity with no unexpected TRAEs. #DAVALung
LOXO-RAS-20001
[Slide 1]
Brain Metastases are common and targetable in Oncogene Driven NSCLC
- Brain metastases occur frequently in KRAS G12C mutant NSCLC (23.4-41.7%).
- 1st generation KRAS G12C OFF inhibitors have demonstrated CNS activity, however, durability of response is lacking.
- Agents with high icORR and durability will be required to significantly improve outcomes in KRAS G12C Mutant NSCLC
Table 2. Intracranial response rates of precision agents in NSCLC brain metastases.
Oncogenic Driver | Brain Metastasis Rates | Precision Agent | Intracranial Response Rates
EGFR | 20-30% [45-49] | Osimertinib | 66% [xx]
RET | ~50% [16] | Selpercatinib (LOXO-292) | 85% [xx]
ALK | 23-34% [49-52] | Brigatinib, Alectinib, Lorlatinib | 78% [xx], 81% [xx], 63% [xx]
ROS1 | 19% [53] | Lorlatinib, Entrectinib, Repotrectinib | 44% [xx], 79% [xx], 100% [xx]
KRAS | 29% [53] | Sotorasib, Adagrasib | 50% [xx], 42% [11]
MET | 11-23% [59] | Capmatinib, Tepotinib | 50% [xx], 73% [xx]
HER2 | 47% [59] | Poziotinib | 89% [xx]
Weller et al. Cancer Treatment Reviews, Volume 130, 2024, 102807; Boldig et al. Int. J. Mol. Sci. 2024, 25, 6961.
———
[Slide 2]
CNS activity of 1st generation KRAS G12C OFF inhibitors
Sotorasib: Docetaxel (N=13) 15.4%; Sotorasib (N=16) 33.3% (confirmed BOR waterfall)
CNS PFS and Time to CNS Progression (Sotorasib vs Docetaxel)
Adagrasib: Adagrasib (n=25) 40%; Docetaxel (n=9) 11% (intracranial objective response, measurable lesions). Adagrasib 10/25; Docetaxel 1/9 (1/3)
The HR for intracranial progression-free survival was 0.93 (95% CI 0.50-1.73).
Time to CNS Progression: Adagrasib vs Docetaxel; median intracranial time to progression Adagrasib NR, Docetaxel NR (2.48)
Dingemans et al. Lung Cancer, Volume 207, 2025, 108683; Barlesi F et al Lancet 2025; 406: 615-26.
———
[Slide 3]
Clinical data for the CNS Activity of Olomorasib
Phase 1/2 LOXO-RAS-20001
Cohort B8: NSCLC, Olomorasib (150 mg BID) (N=21)
Eligibility: Age >=18; ECOG performance status of 0 or 1; Measurable intracranial disease per mRECIST v1.1; Locally advanced/metastatic NSCLC; Presence of a KRAS G12C mutation; At least 1 untreated, active, brain lesion (>=5 mm); No prior KRAS G12C inhibitor; Leptomeningeal disease was excluded
Key objectives: Safety and Tolerability; Pharmacokinetics; Intracranial ORR and DoR; ORR, DoR, DCR and PFS per modified RECIST v1.1
Patient and Disease Characteristics (Olomorasib n=21):
Age, median, years (range) 65 (42, 80)
Sex, n (%) Male / Female 8 (38) / 13 (62)
Race: White / Asian / Black or African American / other / unknown 11 (52) / 3 (14) / 1 (5) / 1 (5) / 5 (24)
ECOG PS 0/1 7 (33) / 13 (62) / 1 (5)
Smoking history Current / Former / Never 15 (71) / 3 (14) / 3 (14)
Number of baseline intracranial lesions: Target 1/2-5 12 (57) / 9 (43); Non-target 0/1/2-5 5 (24) / 14 (67) / 2 (10)
Prior brain radiotherapy Yes/No 11 (52) / 10 (48)
Prior lines of systemic therapy 0/1/2/3+ 4 (19) / 5 (24) / 6 (29) / 6 (29)
Prior systemic therapy: Platinum-based chemotherapy + anti-PD-(L)1 14 (67); Platinum-based chemo alone / Anti-PD-(L)1 alone 1 (5) / 2 (10)
Cassier et al. ESMO 2025
———
[Slide 4]
Clinical data for the CNS Activity of Olomorasib
Intracranial ORR: 43% (95% CI 21.8, 66.0) (waterfall plot, subjects N=21)
Intracranial Rate of DoR >=6 months: 100% (spider plot)
5 patients (24%) with an intracranial complete response
Cassier et al. ESMO 2025
Early clinical findings with neoadjuvant divarasib in KRAS G12C-mutated NSCLC were presented by @ChaftJamie from @MSKCancerCenter, including a 66.7% radiographic ORR, 35.7% major pathologic response, and 21.4% pathologic complete response. #DAVALung
[Slide 1]
Safety
Safety of neoadjuvant divarasib: All patients experienced an adverse event (AE) during neoadjuvant divarasib but most AEs were Grade 1 and manageable (Table 2). No patients discontinued neoadjuvant treatment due to AEs. During neoadjuvant divarasib treatment, the most common AEs (occurring in >=20% of patients) were nausea (80.0%, 12/15), diarrhoea (73.3%, 11/15), constipation (33.3%, 5/15), vomiting (26.7%, 4/15) and fatigue (20.0%, 3/15). No AEs of increased aspartate aminotransferase or alanine aminotransferase occurred.
Table 2. Safety summary of neoadjuvant divarasib, n (%) Neoadjuvant (N=15): Any Grade AE / TRAE 15 (100.0) / 15 (100.0); Grade 3-4 AE / TRAE 3 (20.0) / 1 (6.7); Serious AE / TRAE 2 (13.3) / 1 (6.7); AE leading to dose reduction or interruption 2 (13.3); AE leading to treatment discontinuation 0.
Chaft, et al. ELCC 2026, Copenhagen.
———
[Slide 2]
Efficacy: Pathologic and Radiographic Response
Pathological response, n (%) N=14: MPR 5 (35.7); pCR 3 (21.4).
Radiographic response, n (%) N=15: ORR 10 (66.7); Partial response 10 (66.7); Stable disease 5 (33.3); Progressive disease 0.
Assessed locally in the pathological response analysis population: patients treated with neoadjuvant divarasib and who either underwent surgery (n=14) or discontinued due to AE, or disease progression (n=0). Assessed in efficacy-evaluable patients and unconfirmed.
———
[Slide 3]
Surgical Outcomes
Surgical outcomes, n (%) unless stated (N=14): Median time from first neoadjuvant treatment to surgery, days (range) 61 (55-64); Median time from last neoadjuvant treatment to surgery, days (range) 1 (1-6); Reported surgical delays 0; Median duration of surgery, minutes (range) 225 (147-350); Median time in hospital, days (range) 3 (1-13); R0 resection 14 (100); Resection approach: Robotically assisted VATS / thoracotomy 9 (64.3) / 5 (35.7).
Intraoperative events, n (%) unless stated (N=14): Intraoperative complications/injury 0; Median estimated blood loss, mL (range) (n=9) 100 (5-650); Peri-hilar/lobar adhesions: Yes / No 1 (7.1) / 13 (92.9); Intraoperative fibrosis: Yes / No 1 (7.1) / 13 (92.9).
Chaft, et al. ELCC 2026, Copenhagen.
The evolving role of olomorasib in KRAS G12C-mutated NSCLC was shown by Dr. Timothy Burns from @OSUCCC_James, including first-line combination data with pembrolizumab. #DAVALung
LOXO-RAS-20001SUNRAY-01
[Slide 1]
The LOXO-RAS-20001 study + SUNRAY-01: Olomorasib + Pembrolizumab:
A. Olomorasib (50 mg /100 mg BID) + Pembrolizumab; Randomized 1:1: LOXO-RAS-20001 Part G 1L NSCLC (n=43); SUNRAY-01 Dose Optimization 1L NSCLC (n=42)
Eligibility: Confirmed stage IIIB-IIIC or stage IV NSCLC; No prior therapy for metastatic disease; PD-L1 expression >=1% permitted; ECOG performance status of 0 or 1; Small (n1.5 cm)*, asymptomatic untreated or treated stable brain metastases were allowed
Key Objectives: Safety, Tolerability and Pharmacokinetics; ORR, DoR, DCR and PFS per RECIST v1.1
B. Waterfall: ORR*, % (95% CI); PD-L1 All: 73% (61.8, 81.8); PD-L1 >=50%: 78% (64.4, 88.0); PD-L1 Score 0, 1-49%, >=50%; Treatment ongoing; Received 1 Cycle of SOC; Olomorasib dose: 50 mg BID, 100 mg BID
C. Swimmer: median DoR: NR; Treatment Duration; Median follow-up time: 12.4 months; Complete Response, Partial Response, Progressive Disease, Treatment Ongoing
Johnson ML et al., 2025 WCLC; Burns et al., J Thorac Oncol 2026;21:103528
———
[Slide 2]
The LOXO-RAS-20001 study + SUNRAY-01: Olomorasib + Pembrolizumab: Safety Profile: 1L Olomorasib + Pembrolizumab
Olomorasib + Pembrolizumab (n=85); Parameter n (%) — TRAEs (>=10%) | Any Grade | Grade 1 | Grade 2 | Grade 3 | Grade 4:
Any TRAE 76 (89.4) | 14 (16.5) | 28 (32.9) | 28 (32.9) | 6 (7.1)
Diarrhea 26 (30.6) | 9 (10.6) | 11 (12.9) | 6 (7.1) | -
ALT increased 22 (25.9) | 3 (3.5) | 3 (3.5) | 13 (15.3) | 1 (1.2)
AST increased 20 (23.5) | 4 (4.7) | 4 (4.7) | 11 (12.9) | 1 (1.2)
Nausea 14 (16.5) | 8 (9.4) | 6 (7.1) | - | -
Fatigue 11 (12.9) | 4 (4.7) | 7 (8.2) | - | -
Pruritus 11 (12.9) | 9 (10.6) | 2 (2.4) | - | -
Vomiting 11 (12.9) | 6 (7.1) | 5 (5.9) | - | -
Decreased appetite 9 (10.6) | 5 (5.9) | 4 (4.7) | - | -
Other TRAEs of interest: Pneumonitis/ILD 2 (2.4) | - | - | 1 (1.2) | 1 (1.2)
Dose modifications due to TRAEs: TRAEs led to dose reductions of olomorasib in 29 patients (34.1%); TRAEs led to permanent discontinuation of the treatment regimen in 10 patients (11.8%)
Johnson ML et al, 2025 WCLC; Burns et al., J Thorac Oncol 2026;21:103528
Emerging perioperative approaches for KRAS G12C-mutated NSCLC were discussed by @_hanielaraujo from @UTMDAnderson, covered ongoing trials such as SUNRAY-02, KRAScendo-3, KANDLELIT-013, and NAUTIKA1 evaluating KRAS inhibitor–based strategies. #DAVALung
KRAScendo 3LCMC4NAUTIKA1SUNRAY-02
[Slide 1]
SUNRAY-02: Phase III trial with adjuvant olomorasib for Resected or Unresectable KRAS G12C-Mutant, Non-Small Cell Lung Cancer
Part A: Stage II-IIIB Resected NSCLC -> Randomize -> Olomorasib + Pembrolizumab vs Placebo + Pembrolizumab
Primary endpoint: Disease-Free Survival by Investigator Assessment
Eligibility for Part A:
- Clinical Stage II-IIIB (N2) NSCLC treated via presurgical chemoimmunotherapy, with residual tumor present after surgery. Patients with a pathologic complete response are not eligible
- Pathologic Stage II-IIIB (N2) NSCLC treated via initial upfront resection
———
[Slide 2]
KRAScendo 3: Divarasib Compared With Investigator's Choice of Immunotherapy or Observation in Participants With Resected Stage II-III...
- Stage II-IIIB resected NSCLC with KRAS G12C mutation
- Prior treatment with neoadjuvant immune checkpoint inhibitor
- Participants who have not achieved pCR following neoadjuvant treatment
R 1:1 -> Divarasib vs Pembrolizumab
Schema based on information available on clinical trials.org from NCT07541170 study
———
[Slide 3]
Pembrolizumab±Calderasib (MK-1084) in Completely Resected Stage IIA-IIIB (N2) KRAS G12Cm NSCLC (MK-1084-013) (KANDLELIT-013)
Has a histological/cytological diagnosis of NSCLC and meets one of the following criteria:
- Newly diagnosed, treatment-naive, resectable, clinical Stage IIA-IIIB (N2) NSCLC
- completely resected, pathological Stage IIA-IIIB (N2) NSCLC, including those previously treated outside the study with neoadjuvant platinum-doublet chemotherapy.
R 1:1 -> Calderasib + MK-3475A (subcutaneous pembrolizumab) vs MK-3475A (subcutaneous pembrolizumab)
Schema based on information available on clinical trials.org from NCT07431827 study
———
[Slide 4]
Neoadjuvant treatment with divarasib - NAUTIKA 1 trial
NAUTIKA1 Trial Design
Clinical Eligibility Criteria: Resectable stage IB-IIIA or IIIB (T3N2 per AJCC 8th edition) NSCLC; ECOG PS 0-1.
Molecular Testing: Molecular testing in CLIA-certified laboratory OR LCMC4 neoadjuvant screening trial.
Neoadjuvant cohorts: ALK+ (Alectinib 8 weeks); ROS1+ (Entrectinib 8 weeks); NTRK+ (Entrectinib 8 weeks); BRAF V600 (Vemurafenib + Cobimetinib 8 weeks); KRAS G12C Cohort (Divarasib 8 weeks); PD-L1+ (Atezolizumab 4 cycles + low dose SBRT 8Gyx3).
Surgery + Assessment of Pathologic Response.
Adjuvant: Standard of Care Chemotherapy (4 cycles) + <=2 years of TKI therapy; Care Depends on PD-L1 Status.
Lee et al., WCLC25
Dr. John Heymach @UTMDAnderson discussed the structural basis of HER2 TKI activity, emphasizing that drug binding pocket differences across HER2 mutations help explain variable responses and resistance to targeted therapies. #DAVALung
[Slide 1]
Location of HER2 mutations and amino acid changes have distinct effects on drug efficacy
In Silico Modeling
- Y772dupYVMA had a smaller binding pocket size than V777L
- L775P causes the p-loop to collapse inward yielding smaller pocket volume
- Mutations with smaller drug binding pocket are less sensitive to some TKI cores (e.g. indole-based inhibitors)
[Structural diagram: P-loop, Alpha C helix, Kinase hinge, aC helix (in)]
[Density plot: Pocket volume (A^3); <WT / >=WT; HER2 WT, HER2 L755S, HER2 L755P, HER2 Y772dupYVMA, HER2 V777L; WT TKD]
Robichaux et al, Cancer Cell 2019
———
[Slide 2]
HER2 has a slightly larger binding pocket because of the location of the alphaC helix. Zongertinib fits into a deeper pocket in HER2, but not into the tighter space in EGFR
White: HER2 & Zongertinib
Green: EGFR & Poziotinib
[Structural overlays labeled: EGFR aC-helix; HER2 aC-helix; Zongertinib steric clash with EGFR]
———
[Slide 3]
Zongertinib fits the more flexible and adaptive HER2 pocket, but is not accommodated in EGFR
Poziotinib - EGFR ATP pocket / HER2 ATP pocket
Zongertinib - HER2 ATP pocket
Drugs that inhibit both EGFR and HER2 exon 20 insertions fit into the tighter EGFR exon 20 pocket
[Molecular structure diagrams of Poziotinib and Zongertinib]
———
[Slide 4]
Zongertinib is an HER2-specific, EGFR-sparing TKI with >2 orders of magnitude greater selectivity than poziotinib or afatinib
- Zongertinib is highly selective for mutant HER2 over EGFR wild-type
- Zongertinib resulted in tumor regressions in a patient-derived NSCLC xenograft model carrying a HER2 exon 20 insertion (HER2 YVMA)
[Selectivity index plot HER2 YVMA: Poziotinib, Afatinib near 0; Zongertinib near -2. Drugs listed: Afatinib, Olmutinib, Osimertinib, Poziotinib, Erlotinib, Gefitinib, Lapatinib, Neratinib, Tucatinib, Pyrotinib, Zongertinib]
[Xenograft tumor volume plot CTG-2543: Vehicle; Erlotinib 75 mg/kg QD; Poziotinib 1 mg/kg QD; Zongertinib 5 mg/kg BID; Zongertinib 30 mg/kg BID; Zongertinib 100 mg/kg BID; Average tumor volume (mm3) vs Days]
Zongertinib is a potent, covalent TKI that selectively inhibits HER2 while sparing EGFR wild-type, thereby potentially limiting associated toxicities
1. Wilding B et al. Cancer Discov. 2025;15:119-38. Plots by Wilding B et al. Cancer Discov. 2025; used under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, with minor color amends
Dr. @LeXiuning from @UTMDAnderson presented preclinical data showing NVL-330 demonstrated broad activity across HER2 alterations and introduced the HEROex-1 first-in-human Phase 1a/1b trial evaluating NVL-330 in advanced HER2-altered NSCLC. #DAVALung
HEROEX-1
[Slide 1]
In vitro efficacy NVL-330 vs. zongertinib
In Vitro Activity, HER2 AND HER2ex20
Broad activity on HER2 oncogenic alterations, including HER2 exon20ins, activating point mutations, and amplified wild-type HER2.
IC50 (nM) scatter comparing Poziotinib, Zongertinib, NVL-330 across cell lines (NCI-H2170 HER2amp, BT-474 HER2amp, NCI-N87 HER2amp, NCI-H1781 HER2VC, Ba/F3 HER2 YVMA, VC, GSP, S310F, R678Q, L755S, V777L).
Avoiding EGFR Inhibition
Greater selectivity for HER2ex20 mutations over EGFR than pan-ERBB inhibitors (e.g. poziotinib).
Selectivity index = IC50 (phospho-EGFR WT in A431) / IC50 (phospho-HER2 or viability). More active for HER2 (top) vs more active for wild-type EGFR (bottom).
———
[Slide 2]
In vivo data: NVL-330
NSCLC patient derived xenograft models with HER2 YVMA
ST3107 (HER2 YVMA): Tumor volume (mm3) vs Days on Treatment. Vehicle BID PO; NVL-330 10/30/75 mg/kg BID PO; T-DXd 10 mg/kg Q3W IV. NVL-330 10 mg/kg −38%; higher doses −76%.
PDX model established from a female patient with NSCLC. Patient treated with investigational therapy, nivolumab, carboplatin/gemcitabine.
CTG-2543 (HER2 YVMA): Tumor volume (mm3) vs Days on Treatment. NVL-330 −38% (10 mg/kg) and −83% (higher doses).
PDX model established from brain metastasis of a 75-year-old female Asian non-smoker with NSCLC. Patient treated with carboplatin/paclitaxel, durvalumab; responded then progressed.
———
[Slide 3]
Activity Post T-DXd
NVL-330 demonstrated activity in cells with acquired resistance to T-DXd
Model generation: NCI-N87 cells → T-DXd → Resistant cell lines: NCI-N87 T-DXd-R (aka N87-R)
Resistance mechanism: Payload resistance — Dxd and DM-1 inhibition rate curves (N87 vs N87-R).
NVL-330 activity is maintained in T-DXd resistant cells — Viability (%) vs T-DXd (ng/mL): NCI-N87 vs NCI-N87-T-DXd-R diverge; vs NVL-330 (nM): curves overlap (activity maintained).
1 Wang et al., SITC, 2023; 2 Sun et al., AACR, 2024.
———
[Slide 4]
A First-in-Human Phase 1a/1b Clinical Trial of NVL-330 in Advanced HER2-Altered NSCLC — HERoex-1
PATIENT POPULATION
• Advanced NSCLC harboring HER2 alteration (by local testing)
o Phase 1a: HER2 mutation or HER2 amplification allowed
o Phase 1b: HER2 mutation only
• ≥1 prior systemic therapy, including platinum-based chemotherapy +/- immunotherapy
o Excluded: Prior selective HER2 TKI
o Prior HER2-directed antibodies and HER2-directed ADCs are allowed.
• Excluded: concurrent oncogenic drivers (e.g., EGFR, BRAF, MET, ROS1, ALK, or RET)
• Evaluable but non-measurable disease allowed in Phase 1a
Enrollment ongoing
Phase 1a: BOIN Dose-Escalation, HER2 mutation or HER2 amplification allowed (DL 1 through DL 7)
Phase 1b: Dose Expansion, HER2 mutation only; Dose Expansion at Candidate RP2Ds
PURPOSE: Phase 1a Safety/Tolerability, Select Candidate RP2D(s); Phase 1b Safety/Tolerability, Confirm RP2D
Emerging combination strategies for HER2-mutant NSCLC were the focus of this talk, reviewed ongoing and planned studies of zongertinib with chemotherapy, local consolidation therapy, and HER2-directed approaches. Presented by @UrsWeberMD from @CUCancerCenter #DAVALung
In the DESTINY-Lung02 RP2 analysis, trastuzumab deruxtecan (5.4 mg/kg) demonstrated a median PFS of 10.0 months (95% CI, 7.7–15.2) and a confirmed ORR of 50% in previously treated HER2-mutant metastatic NSCLC. Presented by @Jheymach (@UTMDAnderson). #DAVALung
DESTINY-Lung02
[Slide 1]
Final analysis from DESTINY-Lung02-A RP2 Study of Trastuzumab Deruxtecan in 2L+ HER2 mutant NSCLC.
mPFS, 5.4 mg/kg: 10.0 (7.7-15.2). Confirmed ORR: 50%.
PFS KM: T-DXd 5.4 mg/kg n=102 vs T-DXd 6.4 mg/kg n=50. Median (95% CI), months: 10.0 (7.7-15.2) vs 12.9 (7.2-16.7). T-DXd 5.4 mg/kg: 73% (95% CI, 62%-81%) at ~6mo, 45% (95% CI, 34%-56%) at ~12mo. T-DXd 6.4 mg/kg: 70% (95% CI, 54%-82%), 53% (95% CI, 36%-67%).
ORR by subgroups (6.4 mg/kg): All patients 50/102 aORR 50.0 (39.9-60.1). Race: Asian 35/65 53.8 (41.0-66.3); White 13/23 56.5 (34.5-76.8); Other 3/14 21.4 (4.7-50.8). ECOG PS: 0 14/29 48.3 (29.4-67.5); 1 37/73 50.7 (38.7-62.6). HER2 mutation: Kinase domain 49/99 49.5 (39.3-59.7). CNS metastasis at baseline: Yes 21/35 60.0 (42.1-76.1); No 30/67 44.8 (32.6-57.4). Tobacco users: Never 26/55 47.3 (33.7-61.2); Former 25/47 53.2 (38.1-67.9). Number of prior lines of therapy: 1 16/37 43.2 (27.1-60.5); 2 15/32 46.9 (29.1-65.3); >=3 20/33 60.6 (42.1-77.1). Prior anti-PD-(L)1 treatment: Yes 37/75 49.3 (37.6-61.1); No 14/27 51.9 (31.9-71.3). Prior anti-PD-(L)1 in combination with chemotherapy: Yes 23/51 45.1 (31.1-59.7); No 14/24 58.3 (36.6-77.9). Anti-PD-(L)1 as prior immediate treatment: Yes 10/29 34.5 (17.9-54.3); No 27/46 58.7 (43.2-73.0). Time from IO therapies: <3 months 11/28 39.3 (21.5-59.4); >=3 to <=6 months 5/11 45.5 (16.7-76.6); >6 months 20/31 64.5 (45.4-80.8).
Janne et al JTO 2025.
———
[Slide 2]
Safety Profile of Trastuzumab Deruxtecan: Common Adverse Events (Incidence >=20%) in HER2-Mutant NSCLC.
Body system | AE | All grade, % | Grade 3 or 4, %: Gastrointestinal - Nausea 67/4, Vomiting 32/3, Constipation 37/1, Diarrhea 23/1. Metabolism - Decreased appetite 40/2. Hematologic - Neutropenia 43/19, Anemia 37/11, Leukopenia 29/5, Thrombocytopenia 28/6. Skin - Alopecia 22/0. Hepatobiliary - Transaminases increased 22/3.
Only data for 5.4 mg/kg Q3W arm is shown. Reference(s): Goto K et al. J Clin Oncol. 2023;41:4852-4863.
———
[Slide 3]
Final analysis from DESTINY-Lung02-A RP2 Study of Trastuzumab Deruxtecan in 2L+ HER2 mutant NSCLC.
ILD: 14.9% (all grade) at 5.4 mg/kg dose.
Table 3. Adjudicated Drug-Related ILD. T-DXd 5.4 mg/kg n=101 vs T-DXd 6.4 mg/kg n=50: Any grade, n (%) 15 (14.9) vs 16 (32.0); Grade 1 4 (4.0) vs 3 (6.0); Grade 2 9 (8.9) vs 11 (22.0); Grade 3 1 (1.0) vs 1 (2.0); Grade 4 0 vs 0; Grade 5 1 (1.0) vs 1 (2.0); Grade >=3 2 (2.0) vs 2 (4.0). Outcome of ILD events, n/N (%): Fatal 1/15 (6.7) vs 1/16 (6.3); Not recovered/not resolved 3/15 (20.0) vs 6/16 (37.5); Recovering/resolving 1/15 (6.7) vs 0; Recovered/resolved with sequelae 0 vs 1/16 (6.3); Recovered/resolved 10/15 (66.7) vs 8/16 (50.0).
Janne et al JTO 2025.
Theme · 11 talks
ADCs & Novel Payloads
TROP2, B7-H3, B7-H4, SEZ6 and MET antibody-drug conjugates — sac-TMT, Dato-DXd, ifinatamab, sigvotatug, YL201, BNT324.
Dr. @PatelOncology (@UCSDHealth) on sacituzumab govitecan in NSCLC:
• IMMUN-132-01: ORR 19%, mPFS5.2m, mOS9.5m
• 49% dose reduction, mostly neutropenia
• Negative as monotherapy in 2L mNSCLC & 1L PD-L1>50%; response did not vary by H-score
#DAVALung
At #DAVALung, Dr. Renata Ferrarotto @UTMDAnderson presented Emi-Le, a B7-H4 ADC in R/M Adenoid Cystic Carcinoma (ACC): manageable safety; ORR 35.6%-46.9% by molecular/clinicopathologic features; preliminary PFS ~8m vs 2m control; FDA BTD for R/M solid ACC.
[Slide 1]
Post-Hoc Analysis of pts with aggressive ACC (n=32)
Aggressive ACC: Solid/basaloid histology and at least one of the following: 1) PD/recurrence within 3 ys of diagnosis or 2) Extra-pulmonary metastatic disease.
Waterfall (Best Change in Target Lesion Size from Baseline %): cORR + uPR: 46.9% (including 1 CR); DCR: 81.3%; DOR: 27.9 weeks (95% CI: 13.6, 41.1).
mPFS 8 mos (historical control = 2 mos). Subjects at Risk (Overall): 32 31 26 20 19 16 11 8 5 4 4 3 2 2 2 1 1 1 1 0 across weeks 0-96.
Hanna G...Ferrarotto R, ASCO, 2026
———
[Slide 2]
ORR in ACC-I (n=45), All doses
Waterfall (Best Change in Target Lesion Size from Baseline %): cORR: 35.6% (including 1 CR); DCR: 82.2%; DOR: 32.1 weeks (95% CI: 13.6, NR).
5/12/2025: Emi-Le granted FDA Breakthrough Therapy Designation for aggressive ACC.
Hanna G...Ferrarotto R, ASCO, 2026
———
[Slide 3]
ACC Patients' Characteristics and AE Profile
Characteristic / Patients with ACC (n=48): Solid/Basaloid histology or HGT, n (%) Yes 37 (77.1) No 1 (2.1) Unknown 10 (20.8); Extra-pulmonary site(s) of metastases Yes 37 (77.1) No 11 (22.9); PD within 3 years of diagnosis, n (%) Yes 33 (68.8) No 15 (31.3); NOTCH 1-4 mutation, n (%) Yes 32 (66.7) No 10 (20.8) Unknown 6 (12.5); High c-Myc, n (%) Yes 14 (29.2) No 4 (8.3) Unknown 30 (62.5); Negative or low p63, n (%) Yes 17 (35.4) No 9 (18.8) Unknown 22 (45.8); B7-H4 expression, n; Median TPS (range) 77.5% (2-100).
TRAE in >= 10% of pts, All ACC patients (N=48) (grade 3+ shown as dark bar / total %): AST increased 25 / 73; Proteinuria 35 / 77; Fatigue 8 / 65; Nausea 2 / 31; Anemia 17 / 31; ALT increased 2 / 42; Decreased appetite 19; ALP increased 31; Platelet count decreased 27; Amylase increased 21; Pyrexia 13; Vomiting 2 / 10; Hypertension 17 / 27; Hypoalbuminemia 25; Diarrhea 4 / 8; Troponin I increased 21.
TRAE leading to treatment D/C: 2.1%.
Hanna G...Ferrarotto R, ASCO, 2026
———
[Slide 4]
Emi-Le: A B7-H4 ADC
Emi-Le (emiltatug ledadotin; XMT-1660): B7-H4-directed ADC with a proprietary auristatin F-HPA microtubule inhibitor payload designed with controlled bystander effect.
Novel ADC platform; Site-specific conjugation; Target-optimized DAR 6; Proprietary auristatin-derived payload.
Sigvotatug vedotin at #DAVALung | Dr. @CoreyLangerMD@PennMedicine: IB6 is highly expressed in NSCLC (>90%); this investigational IB6-directed MMAE ADC had updated Phase 1 NSCLC data. With pembrolizumab in 1L NSCLC, ORR was 61.5% (TPS ≥1%) and 50.0% (TPS <1%).
Be6A-Lung02SGNB6A-001
[Slide 1]
Conclusions
- SV and pembrolizumab demonstrated encouraging and emerging antitumor activity in patients with advanced 1L NSCLC and HNSCC
- 1L NSCLC: PD-L1 TPS >=1 ORR = 61.5%; PD-L1 TPS <1 ORR = 50.0%; All patients with TPS >=50 (n=4) responded
- HNSCC: CPS >=1 ORR = 40.0%; All patients with CPS >= 20 (n=4) responded
- Overall safety is manageable and generally consistent with known safety profiles of individual components
- IRAEs as expected with pembrolizumab monotherapy
- Treatment-related discontinuation was 15.7%
- These data support further development in 1L NSCLC, including the ongoing phase 3 study of SV and pembrolizumab
Be6A Lung-02 Study (NCT06758401):
- Stage IIIB, IIIC, or IV NSCLC
- PD-L1 TPS >=50
- No known AGA mutations with approved 1L therapies
- No prior systemic therapy for locally advanced, unresectable, or metastatic disease
1:1 N=714 -> SV 1.8 mg/kg AiBW Q2W + Pembrolizumab 400 mg Q6W; vs Pembrolizumab 400 mg Q6W
Presented by: Kartik Sehgal; Sehgal, K et al ASCO 2025; Penn Medicine Abramson Cancer Center
———
[Slide 2]
SV AEs of Interest and IRAEs
SV AEs of interest by composite term — All treated patients (N=51); TEAE composite term, n (%) | Any grade | Grade >=3:
Oral/Pharyngeal Mucositis 17 (33.3) | 4 (7.8)
Peripheral neuropathy 16 (31.4) | 1 (2.0)
Hepatotoxicity 10 (19.6) | 2 (3.9)
Neutropenia 6 (11.8) | 6 (11.8)
ILD/pneumonitis 4 (7.8) | 0
Hyperglycemia 3 (5.9) | 0
Immune Related AEs (IRAEs) — All treated patients (N=51); TEAE, n (%) (>=10% Any-grade or Any grade >=3) | Any grade | Grade >=3:
Any event 28 (54.9) | 9 (17.6)
Asthenia 9 (17.6) | 2 (3.9)
Fatigue 9 (17.6) | 0
Decreased appetite 8 (15.7) | 2 (3.9)
Colitis 3 (5.9) | 2 (3.9)
Diarrhea 2 (3.9) | 2 (3.9)
Stevens-Johnson syndrome 2 (3.9) | 2 (3.9)
Adrenal insufficiency 2 (3.9) | 1 (2.0)
Eczema 2 (3.9) | 1 (2.0)
Immune-mediated nephritis 1 (2.0) | 1 (2.0)
- Most common TEAEs were generally consistent with known safety profile of individual components
- IRAE profile was generally consistent with pembrolizumab monotherapy
2 Cases of Stevens-Johnson Syndrome (SJS): 1 Grade 5 event; 1 Grade 4 event, recovering with supportive care; Confounded by exposure to antibiotics, which may be associated with SJS; SJS has been reported with pembrolizumab; No SJS cases have been reported in >500 patients treated with SV monotherapy; Toxicity management guidance added for patients receiving combination
Sehgal, K et al ASCO 2025
———
[Slide 3]
Emerging Efficacy of SV and Pembrolizumab in 1L NSCLC
1L NSCLC (expansion cohort) | All efficacy-evaluable (n=21) | TPS>=1 (n=13) | TPS<1 (n=8):
ORR (95% CI), % — 57.1 (34.0-78.2) | 61.5 (31.6-86.1) | 50.0 (15.7-84.3)
cORR (95% CI), % — 42.9 (21.8-66.0) | 46.2 (19.2-74.9) | 37.5 (8.5-75.5)
BOR, n (%): CR 2 (9.5) | 2 (15.4) | 0; PR 10 (47.6) | 6 (46.2) | 4 (50.0); SD 7 (33.3) | 4 (30.8) | 3 (37.5); PD 0 | 0 | 0; NE 1 (4.8) | 1 (7.7) | 0; No assessment 1 (4.8) | 0 | 1 (12.5)
DCR (95% CI), % — 90.5 (69.6-98.8) | 92.3 (64.0-99.8) | 87.5 (47.3-99.7)
Median DOR has not been reached; Median follow-up was 4.8 months (95% CI, 3.7-6.0)
Waterfall/spider: At data cutoff: 4/4 patients with TPS>=50 had CR or PR; TPS >=50; Treatment ongoing
Sehgal, K et al ASCO 2025
———
[Slide 4]
Study Design and Baseline Characteristics
Ongoing Phase 1 SGNB6A-001 (NCT04389632)
SV and pembrolizumab; Safety cohort (Advanced solid tumors); Expansion cohort:
- Treatment-naive, advanced, metastatic or unresectable NSCLC or HNSCC
- ECOG PS 0/1
- For NSCLC, no known EGFR or ALK mutations
- No contraindication for pembrolizumab monotherapy
- For HNSCC, PD-L1 CPS >=1
SV 1.8 mg/kg AiBW Q2W + Pembrolizumab 400 mg IV Q6W
Endpoints: safety, efficacy, and PK
Initial safety and efficacy results (data cutoff March 3, 2025)
Overall population (including NSCLC and HNSCC) (N=51): Median age (range), years 64.0 (34.0-81.0); Male, n (%) 35 (69); ECOG PS of 1, n (%) 26 (51)
NSCLC characteristics, n (%) (n=27): Treatment-naive in advanced/recurrent or metastatic setting 26 (96); Non-squamous histology 17 (63); PD-L1 status TPS<1 10 (37), TPS>=1 17 (63), TPS>=50 4 (15)
HNSCC characteristics, n (%) (n=23): Treatment-naive in advanced/recurrent or metastatic setting 22 (96); Primary tumor location Oral cavity 14 (61), Oropharynx (4/5 patients p16 positive) 5 (22), Other 4 (17); PD-L1 CPS>=20 4 (17)
Sehgal, K et al ASCO 2025
From ADC design to Phase 3 development, Dr. Melinda Hsu from @UHhospitals reviewed the evolving ZL-1310 story, including the DLLEVATE study versus investigator’s choice. #DAVALung
DLLEVATE
[Slide 2]
ZL-1310 has excellent preclinical activity
ZL-1310 Preclinical Activity
ZL-1310-mediated cytotoxicity in DLL3+ NCI-H69 SCLC Cells
Viability (%) vs Concentration (nM)
- Naked mAb
- ZL1310
ZL-1310-mediated significant TGI in human SCLC LU5215 (DLL3high) PDX Model
Tumor Volume (mm3) vs Treatment days
- Vehicle
- ZL1310, 1 mpk
- ZL1310, 3 mpk
- ZL1310, 6 mpk
Q3W x 3
Liu LN, et al. Poster presented at: ELCC; March 22, 2024; Prague, Czech Republic
———
[Slide 3]
Phase 1 Study: NCT06179069
Phase 1, open-label, dose-escalation and expansion study of ZL-1310 as monotherapy and in combination with atezolizumab for r/r metastatic SCLC
Monotherapy Study Design
Patients with:
- metastatic or extensive-stage SCLC with ≥1 prior PBC regimen and ≤3 prior regimens; prior DLL3-targeted therapy allowed
- asymptomatic brain metastasis (previously treated or untreated) allowed
Part 1A: Dose Escalation (ZL-1310 IV Q3W) -> Part 2: Dose Expansion
Part 1A: Dose Escalation
Primary Endpoints: DLT, TEAEs, and SAEs
Secondary Endpoints: ORR, DOR, PFS, DCR, and OS
PK parameters of ZL-1310, total antibody, and unconjugated payload
Dose escalation cohorts: 0.8 mg/kg N=4; 1.6 mg/kg N=6; 2.0 mg/kg N=4; 2.4 mg/kg N=7; 2.8 mg/kg (Enrolling)
R -> RD 1, RD 2
———
[Slide 4]
DLLEVATE: Randomized, open-label Phase 3 of ZLL-1310 compared to investigator's choice
Key inclusion criteria
- Received 1L platinum based therapy (in combination with an anti-PD-L1 agent) and had documented disease progression after either 1L platinum or 2L tarlatamab
- History of treated and stable CNS metastases, or untreated and asymptomatic CNS metastases not requiring steroids, anticonvulsants, or local therapy is allowed
Eligibility box:
- ES-SCLC
- PD after first line platinum-based regimen, with or without tarlatamab as 2nd line
- At least one measurable lesion
- ECOG 0-1
Randomized 1:1
ZL-1310 1.6 mg/kg Q3W N ≈ 240
Investigator's Choice Therapy Q3W N ≈ 240
Dowlati A, et al. ASCO 2026
Obrixtamig continues to generate interest in DLL3-expressing thoracic and neuroendocrine tumors. @JSabari from @nyulangone summarized the evolving evidence and next steps at #DAVALung.
DAREON-8DAREON-Lung1
[Slide 1]
Study 1438-0001: First-in-human, Phase I, dose-escalation Obrixtamig monotherapy in pts with SCLC, epNEC, or LCNEC-L; WCLC 2023; UPDATE ASCO 2025
NCT04429087
Key inclusion criteria: Advanced SCLC, epNEC, or LCNEC-L; DLL3-positive according to central review; Failed/ineligible for available standard therapies; Adequate organ function; Screening for asymptomatic brain metastasis was not required.
Regimen B1* (n=10): Fixed dose 0-30 ug/kg QW.
Regimen B2 (n=79): BLRM Target dose 90-1580 ug/kg QW; Step-up doses 30 and 80 ug/kg QW.
Regimen B3 (n=55): BLRM Target dose 90-1080 ug/kg QW for 3 weeks then Q3W from Week 7; Step-up doses 10, 30, and 90 ug/kg QW.
Switch to step-up dosing (B2) based on Regimen A and B1 data. Switch to step-up dosing (B3) based on Regimen B2 data.
Primary endpoint: MTD; DLTs in the MTD evaluation period. Secondary endpoints: OR (RECIST v1.1), PK.
———
[Slide 3]
DAREON-8
Phase I dose escalation and expansion of obrixtamig in combination with 1L SoC in ES-SCLC
NCT06077500
Key inclusion criteria: Histologically/cytologically confirmed ES-SCLC; Eligible for carboplatin + etoposide + atezolizumab; Adequate liver, bone marrow, and renal function; No previous T-cell engager or DLL3-targeted therapy; No active/documented history of autoimmune disease requiring systemic treatment; No LMD or symptomatic brain metastases (asymptomatic brain metastases are eligible).
Part A: dose escalation (BLRM with overdose control): Obrixtamig (10, 30, 60 mg) + SoC (carboplatin + etoposide + atezolizumab) -> RP2D.
Part B: dose expansion: Obrixtamig (60 mg) + SoC (carboplatin + etoposide + atezolizumab). Induction Cycle 1-4: Obrixtamig + carboplatin + etoposide + atezolizumab. Maintenance Cycle 5 onwards: Obrixtamig + atezolizumab.
Primary endpoint: DLTs in the MTD evaluation period. Secondary endpoints: AEs and DLTs during the on-treatment period. Further endpoints: Efficacy (ORR, DoR) by RECIST v1.1 (investigator assessed).
———
[Slide 4]
DAREON Lung-1
Phase III, multicenter, open-label, randomized trial of IV obrixtamig in combination with atezolizumab, carboplatin, and etoposide vs. atezolizumab, carboplatin, and etoposide (SoC) as 1L treatment in patients with ES-SCLC
NCT07472517
Key inclusion criteria: Histologically confirmed ES-SCLC; No previous treatment for ES-SCLC; Tested for DLL3 expression status and other biomarkers prior to randomization; ECOG PS 0-1; No previous DLL3-targeted therapy.
Randomized 1:1 -> Obrixtamig + atezolizumab + carboplatin + etoposide (SoC); Atezolizumab + carboplatin + etoposide (SoC). Up to 36 months.
Primary endpoint: OS. Secondary endpoints: PFS, OR, safety, PROs.
YL201 (Tam-peli) in lung cancer: Dr. Jeffrey Petty (@AtriumHealth, @wakeforestmed) presents the B7H3-targeted ADC YL201, showing activity in ES-SCLC, NPC, and LELC, with hematologic toxicity as the main dose-dependent DLT. #DAVALung
[Slide 1]
Phase 1/1b clinical trial design
(CONSORT flow diagram: 418 patients screened; screening failure n=126; enrolled; dose escalation and dose expansion cohorts at 1.6 mg/kg, 2.0 mg/kg, 2.4 mg/kg, 2.8 mg/kg Q3W; disease cohorts ES-SCLC, NPC, relapsed NSCLC, ESCC, Other solid tumors)
Safety table (across dose groups): TRAEs; Associated with treatment discontinuation; Associated with dose reduction; Associated with treatment interruption; Associated with Death; Grade >=3 TRAE; TR-SAE; hematologic TRAEs (Leukopenia, Anemia, Neutropenia, Lymphopenia, Thrombocytopenia) and non-hematologic (Nausea, Alopecia, Hypoalbuminemia, blood alkaline phosphatase increased, Vomiting, Fatigue, Hyponatremia, Diarrhea, aspartate aminotransferase increased, Weight decreased, Constipation, Hypokalemia, Pneumonia, Hypertriglyceridemia); ILD row
Broad activity table by cohort: ES-SCLC (n=73), NPC (n=71), Wild-type NSCLC [Adeno (n=28), Squamous (n=12)], ESCC (n=36), Others (n=45), Total (n=387); Median follow-up months; BOR CR/PR/SD/PD/NE; ORR (confirmed and pending confirmation) 63.0% ES-SCLC; ORR (confirmed) 63.9% ES-SCLC, 43.6% NPC, 54.2% LELC; DCR; mDOR; mPFS
Nature Medicine Volume 31 June 2025: 1949-1957
———
[Slide 2]
Activity in SCLC
(Waterfall plot c: ES-SCLC patients Best change from baseline (%); by dose 1.6 mg/kg (n=2), 2.0 mg/kg (n=37), 2.4 mg/kg (n=36), 2.8 mg/kg (n=3); Pending confirmation (n=1); Confirmed (n=46))
(Swimmer plot d: duration by Months; Response, Stable disease, Progressive disease, Not evaluable; Treatment ongoing)
SCLC brain mets: (bar chart by 2.0 mg/kg and 2.4 mg/kg)
Zhao et al, ELCC 2025; Nature Medicine Volume 31 June 2025: 1949-1957
———
[Slide 3]
Activity beyond lung cancer
(Waterfall plot e: NPC patients Best change from baseline (%); 2.0 mg/kg (n=35), 2.4 mg/kg (n=34), 2.8 mg/kg (n=0); Pending confirmation (n=0); Confirmed (n=34))
(Swimmer plot f: Months; 2.0 mg/kg (n=35), 2.4 mg/kg (n=34), 2.8 mg/kg (n=0); Treatment ongoing; Response; Stable disease; Progressive disease; Not evaluable)
News: MediLink Therapeutics Announces B7-H3 ADC YL201 Met Primary Endpoint in Phase 3 Nasopharyngeal Carcinoma Study
Nature Medicine Volume 31 June 2025: 1949-1957
———
[Slide 4]
What is LELC (lymphoepithelioma like carcinoma)?
(IHC panel: LELC vs Squamous Carcinoma; EBV, PD-L1, CK stains)
"Pulmonary LELC typically affected young patients and was not associated with smoking history; however, pulmonary LELC was associated with Epstein-Barr virus infection in the Asian population. The majority of patients were in early or locally advanced stages and exhibit an improved prognosis compared with other types of NSCLC. Pulmonary LELC was sensitive to chemotherapy and surgery, with postoperative chemotherapy-based multimodality treatment recommended."
(CT chest image)
Oncol Lett. 2017 Jun 30;14(3):3110-3116.
At #DAVALung, Dr. @DasMillie11@StanfordMed discussed ABBV-706, an anti-SEZ6 ADC in SCLC: 1.8 mg/kg 2L monotherapy showed ORR 82% and mDOR 6.6m; ABBV-706 + budigalimabshowed ORR 54.5%, mPFS 8.1m and mOS NR, with no ILD in combo.
ABBV-706
[Slide 1]
ABBV-706 + Budigalimab: Part 3 Efficacy
1.8 mg/kg + Budi, n = 11
Confirmed ORR, n (%): 6 (54.5); 95% CI 23.4, 83.3
Confirmed best response, n (%): CR 0; PR 6 (54.5); SD 3 (27.3); PD 1 (9.1); Not assessed 1 (9.1)
Confirmed CBR, n (%) > 6 months: 9 (81.8); 2 (18.2)
Median DOR, months (95% CI): 6.7 (5.5, NE)
Median follow-up, months: 9.1
PFS KM curve, Median PFS: 8.1 mos.
1.8 mg/kg + Budi [PFS] Median 8.1 (1.4, NE); 1.8 mg/kg + Budi [OS] Median NR (2.5, NE)
K-M estimates at 6 months, % (95% CI): PFS 51 (18, 77); OS 64 (30, 85)
K-M estimates at 9 months, % (95% CI): PFS NR (NE, NE); OS 64 (30, 85)
Byers L, et al. ASCO 2026. Abstract 8008.
———
[Slide 2]
ABBV-706 +/- Budigalimab: Part 2 + 3 Safety
- Most common Grade >= 3 TRAEs were hematologic
- Most GI toxicity events were Grade 1-2
- Rates of dysgeusia, alopecia, and stomatitis were < 5%
- Any-grade treatment-related adjudicated ILD: Monotherapy 7/124 (5.6%) patients; Combination 0/11 patients; 4/7 patients had grade 1-2 events
Tornado bar chart, ABBV-706 monotherapy 1.8 mg/kg as 2L+ (n = 41) vs ABBV-706 1.8 mg/kg + budi (N = 11), Grade 1-2 vs Grade >=3, Percentage %:
Anemia: mono 41.5 / 12.2; combo 27.2 / 27.3
Nausea: mono 36.6; combo 45.5
Neutrophil count decreased/neutropenia: mono 19.5 / 14.6; combo 27.3 / 18.2
Fatigue: mono 2.4 / 31.7; combo 18.2
Platelet count decreased/thrombocytopenia: mono 14.6 / 9.8; combo 36.4
White blood cell count decreased: mono 7.3 / 12.2; combo 45.5
Decreased Appetite: mono 2.4 / 17.1; combo 18.2 / 9.1
Vomiting: mono 17.1; combo 9.1
Byers L, et al. ASCO 2026. Abstract 8008.
———
[Slide 3]
ABBV-706: Part 2 Efficacy (OS)
Overall Survival Rate KM curve. Total, 1.8 mg/kg as 2L+, 1.8 mg/kg as 2L.
Median, months (95% CI): Total 11.3 (9.1, 14.8); 1.8 mg/kg as 2L+ 12.4 (8.2, 17.3); 1.8 mg/kg as 2L 14.3 (7.8, NE)
K-M OS 18-month estimate (95% CI): Total (N=124) 0.24 (0.14, 0.35); 2L+ (n=41) 0.22 (0.08, 0.42); 2L (n=17) 0.43 (0.18, 0.65)
Overall survival by CTFI:
CTFI < 90 days: 36/66 14.3 (9.9,17.4); 16/25 14.3 (7.8,17.3); 7/13 15.2 (7.8,NE)
CTFI < 30 days: 19/29 12.4 (6.8,17.6); 8/11 15.2 (3.8,17.6); 3/4 9.5 (2.0,NE)
Byers L, et al. ASCO 2026. Abstract 8008.
———
[Slide 4]
ABBV-706: Part 2 Efficacy
ORR* Monotherapy by Cohort (Total, 1.8 mg/kg as 2L+, 1.8 mg/kg as 2L):
Total 52% (65/124); 2L+ 56% (23/41); 2L 82% (14/17)
ORR* Monotherapy by CTFI:
CTFI >= 90 days: Total 50% (22/44); 2L+ 58% (7/12); 2L 100% (4/4)
CTFI < 90 days: Total 55% (35/64); 2L+ 56% (14/25); 2L 77% (10/13)
CTFI < 30 days: Total 52% (14/27); 2L+ 46% (5/11); 2L 50% (2/4)
Median DOR, months (95% CI): Total 5.3 (4.1, 6.7); 2L+ 5.9 (3.6, 11.1); 2L 6.6 (3.1, 12.5)
Byers L, et al. ASCO 2026. Abstract 8008.
B7-H3 ADCs in SCLC: Dr. @DasMillie11 (@stanfordmed) reviews emerging B7-H3-targeting ADCs in SCLC, including I-DXd, HS-20093, YL201, MHB088C, 7MW3711, and SYS6043 at #DAVALung
IDeate-Lung02IDeate-Lung03YL201
[Slide 1]
I-DXd: Safety
TRAEs reported in >=10% of patients in the total I-DXd 12-mg/kg group (N=137). Incidence (any grade / Grade >=3), %:
Nausea 43.1 / 2.2; Neutropenia 34.3 / 13.9; Anemia 34.3 / 10.2; Decreased appetite 32.8 / 1.5; Leukopenia 23.4 / 3.6; Lymphopenia 19.7 / 12.4; Thrombocytopenia 19.0 / 5.8; Asthenia 19.0 / 1.5; Fatigue 16.1 / 2.2; Diarrhea 15.3 / 1.5; Constipation 12.4 / 0; Vomiting 11.7 / 0.7.
- Among the most common TRAEs, the majority were Grade 1 or 2
- Adjudicated treatment-related ILD/pneumonitis was reported in 17 (12.4%) patients: Grade 1 or 2, n=11 (8.0%); Grade 3, n=4 (2.9%); Grade 5, n=2 (1.5%)
- No ILD events were pending adjudication at data cutoff
FDA Priority Review Ongoing Trials in SCLC:
IDeate-Lung02: Phase 3 Trial of 2nd line I-DXd (NCT06203210)
IDeate-Lung03: Phase 1b/2 Trial of First-Line I-DXd + Atezo/Chemo in ES-SCLC (NCT06362252)
Ahn MJ, et al. WCLC 2025. Abstract OA06.03. Rudin CM, et al. J Clin Oncol. Published online October 14, 2025. doi:10.1200/JCO-25-02142.
———
[Slide 2]
YL201: Efficacy and Safety
Best Objective Response waterfall plot (ES-SCLC patients), doses 1.6/2.0/2.4/2.8 mg/kg.
Outcome | YL201:
Confirmed ORR, % (95% CI): 63.9 (51.7-74.9)
DCR, % (95% CI): 91.7 (82.7-96.9)
mDoR, mo (95% CI): 5.7 (3.9-6.4)
mPFS, mo (95% CI): 6.3 (5.6-7.6)
TRAE in >=20% of All Patients, n (%), All (n=312) / 2.0 mg/kg (n=96) / 2.4 mg/kg (n=195), P-Value (2.0 vs 2.4):
Leukopenia 207 (66.3); 58 (60.4); 138 (70.8); Any Grade 0.0766, Grade>=3 0.0014
Anemia 202 (64.7); 59 (61.5); 133 (68.2)
Neutropenia 192 (61.5); 49 (51.0); 134 (68.7); Grade>=3 0.0096
Lymphopenia 111 (35.6); 26 (27.1); 77 (39.5)
Thrombocytopenia 104 (33.3); 32 (33.3); 65 (33.3)
Anorexia 111 (35.6); 25 (26.0); 81 (41.5)
Nausea 82 (26.3); 25 (26.0); 50 (25.6)
Hypoalbuminemia 71 (22.8); 21 (21.9); 48 (24.6)
AESI ILD 4 (1.3); 2 (2.1); 2 (1.0); IRR 1 (0.3); 0; 0
FDA Breakthrough Designation. Ongoing phase III trial in SCLC: Phase III trial of 2nd line YL201 (NCT06612151)
Ma Y, et al. Nat Med. 2025;31(6):1949-1957.
———
[Slide 3]
7MW3711: Phase I/II Study
Payload: Camptothecin (topo I inhibitor); DAR: 4:1. NCT06008366
Dose escalation (Accelerated titration & 3+3+3): 1.5 mg/kg Q3W (N=1); 3.0 mg/kg Q3W (N=4); 4.5 mg/kg Q3W (N=3); 4.0 mg/kg Q2W (N=4); 6.0 mg/kg Q3W (N=3).
Dose expansion: 6.0 mg/kg Q3W (N=14); 4.0 mg/kg Q2W (N=31); 4.5 mg/kg Q3W (N=14). Indications: Lung cancer, Esophageal Carcinoma, Ovarian Cancer, Prostate Cancer, Others.
Primary Endpoint: Safety, Tolerability, MTD, RP2D. Secondary Endpoint: PK, ORR, DOR, DCR, PFS, TTR, ADA. Data cutoff: Sep. 15, 2025.
Small Cell Lung Cancer (4.0 mg/kg Q2W): ORR = 50.0%, DCR = 90.0%. Waterfall plot with B7-H3 H-Score.
Grade >=3 TEAEs (>=5% pts), N=67: WBC Count Decreased 29 (43.3); Neutrophil Count Decreased 27 (40.3); Anemia 24 (35.8); Lymphocyte Count Decreased 23 (34.3); Platelet Count Decreased 9 (13.4); Hypokalemia 7 (10.4); Diarrhea 7 (10.4).
FDA Orphan Drug Designation for SCLC. Ongoing phase I/II trial in solid tumors: 7MW3711 + JS207 (bispecific anti PD-1/VEGF-A) +/- chemotherapy (NCT07466160)
Liang X, et al. ESMO 2025. Abstract 958P.
———
[Slide 4]
SYS6043: Phase I/II Study
Payload: JS-1 (topo I inhibitor); DAR: 6:1.
Key eligibility criteria: ECOG PS of 0-1; Aged 18-75 years; Histologically confirmed advanced and/or metastatic solid tumors; At least a measurable lesion as per RECIST version 1.1; Relapsed or progressed after standard treatment.
Phase I dose escalation (BOIN design): 1.2/2.4/4.0/6.0/8.0/10.0 mg/kg Q3W and 4.0/6.0 mg/kg Q2W.
Phase II dose expansion: 4.0 mg/kg Q3W, 6.0 mg/kg Q3W, 8.0 mg/kg Q3W, 6.0 mg/kg Q2W. Indications: Lung Cancer, Breast Cancer, Gynecologic Cancer, Nasopharyngeal Cancer, HNSCC, ESCC, Liver cancer, Others.
SCLC ORR: 66.7% (waterfall plot).
TEAE incidence bar chart (All grade vs >=grade 3): TRAEs 96.7% / 37.2%; Anemia 59.5% / 14.1%; Leukopenia 49.6%; Neutropenia 49.0%; and others.
FDA Orphan Drug Designation for SCLC.
Zhang L, et al. ASCO 2026. Abstract 3002.
I-DXd in previously treated ES-SCLC: Dr. @LaurenByersMD (@MDAndersonNews) presented IDeate-Lung01, a phase 2 study of ifinatamab deruxtecan (B7-H3 ADC). At 12 mg/kg: ORR 48.2%, mPFS 4.9 mo, mOS 10.3 mo. #DAVALung
IDeate-Lung01
[Slide 1]
I-DXd 12 mg/kg demonstrated promising antitumor activity
Waterfall: Best percentage change in sum of lesion diameters from baseline. I-DXd LOT 2L (orange) / 3L+ (blue); Baseline brain metastases Yes/No; Select prior therapy * DLL3-targeting TCE, † TOPO I inhibitor.
I-DXd 12 mg/kg | Total (N=137) | 2L (n=32) | 3L+ (n=105)
Confirmed ORR, % (95% CI): 48.2 (39.6-56.9) | 56.3 (37.7-73.6) | 45.7 (36.0-55.7)
CR, n (%): 3 (2.2) | 0 | 3 (2.9)
PR, n (%): 63 (46.0) | 18 (56.3) | 45 (42.9)
DCR, % (95% CI): 87.6 (80.9-92.6) | 96.9 (83.8-99.9) | 84.8 (76.4-91.0)
Data cutoff: March 3, 2025.
———
[Slide 2]
Responses with I-DXd 12 mg/kg were rapid and durable
Spider plot: Percentage change in sum of lesion diameters from baseline over Months.
Total I-DXd 12 mg/kg (N=137; 66 with confirmed CR/PR):
TTR, median (range), months: 1.4 (1.0-8.1)
DOR, median (95% CI), months: 5.3 (4.0-6.5)
Among patients who received I-DXd 12 mg/kg as 2L therapy (n=32), median TTR was 1.4 months (range, 1.2-4.0) and median DOR was 7.2 months (95% CI, 3.6-NE)
Data cutoff: March 3, 2025.
———
[Slide 3]
mPFS was 4.9 months and mOS was 10.3 months with I-DXd 12 mg/kg
PFS KM — Total I-DXd 12 mg/kg (N=137): mPFS (95% CI), months 4.9 (4.2-5.5); PFS rate % (95% CI): 3 months 68.0 (59.4-75.2), 6 months 35.3 (27.3-43.4), 9 months 19.3 (12.9-26.5).
OS KM — Total I-DXd 12 mg/kg (N=137): mOS (95% CI), months 10.3 (9.1-13.3); OS rate % (95% CI): 3 months 89.1 (82.5-93.2), 6 months 77.4 (69.4-83.5), 9 months 59.1 (50.4-66.8).
Among patients who received I-DXd 12 mg/kg as 2L therapy (n=32), mPFS was 5.6 months (95% CI, 3.9-8.1) and mOS was 12.0 months (95% CI, 7.3-19.1)
Data cutoff: March 3, 2025.
———
[Slide 4]
The most common TRAEs were hematologic or gastrointestinal in nature, and fatigue
TRAEs reported in ≥10% of patients in the total I-DXd 12-mg/kg group (N=137). Incidence (any grade / Grade ≥3), %:
Nausea 43.1 / 2.2
Neutropenia 34.3 / 13.9
Anemia 34.3 / 10.2
Decreased appetite 32.8 / 1.5
Leukopenia 23.4 / 3.6
Lymphopenia 19.7 / 12.4
Thrombocytopenia 19.0 / 5.8
Asthenia 19.0 / 1.5
Fatigue 16.1 / 2.2
Diarrhea 15.3 / 1.5
Constipation 12.4 / 0
Vomiting 11.7 / 0.7
• Among the most common TRAEs, the majority were Grade 1 or 2
• Adjudicated treatment-related ILD/pneumonitis was reported in 17 (12.4%) patients: Grade 1 or 2, n=11 (8.0%); Grade 3, n=4 (2.9%); Grade 5, n=2 (1.5%)
• No ILD events were pending adjudication at data cutoff
Data cutoff: March 3, 2025.
Mehmet Altan (@UTMDAnderson) reviews BNT324/DB-1311, a B7-H3 ADC, with pumitamig/BNT327 (PD-L1×VEGF-A). Elfe-D showed activity in SCLC/NSCLC, with SCLC ORR 56.2%, supporting Phase 1b/2 combination testing. #DAVALung
BNT324/DB-1311Elfe-D
[Slide 1]
Open-label, two-part Phase 1b/2 trial to evaluate the efficacy, safety, PK, and recommended dose of Elfetabart drozuntecan (BNT324) in combination with Pumitamig in Advanced Lung Cancer
Part 1: Dose escalation (BOIN Design) / Backfill. NCT06892548.
Key Inclusion Criteria: Unresectable advanced/metastatic lung cancer (SCLC or NSCLC); Measurable disease (RECIST v1.1); ECOG PS 0-1; Adequate organ function; Life expectancy >=3 months; Eligible regardless of PD-L1 status.
Key Exclusion Criteria: Prior treatment with B7H3 targeted therapy; History of significant hematologic toxicity to prior lines of therapy.
Dose optimization: DO1 1L nsq NSCLC AGA-; DO2 2L+ SCLC, post-chemo +/- IO.
BNT324/DB-1311 dose (mg/kg): DL0-1 BNT324 4.5 + BNT327 30; DL1-1 BNT324 6 + BNT327 30; DL2-1 BNT324 9 + BNT327 30; Starting Dose DL0-0 BNT324 4.5 + BNT327 20; DL1-0 BNT324 6 + BNT327 20; DL2-0 BNT324 9 + BNT327 20.
Part 1, patients with SCLC or NSCLC receive BNT324/DB-1311 + pumitamig Q3W using a Bayesian optimal interval dose escalation design. 3 dose levels for Elfe-D; 2 dose levels for Pumitamig.
MD Anderson Cancer Center
———
[Slide 2]
Combination of Pumitamig (BNT327) with Elfe-D (BNT324)
Pumitamig is an investigational anti-PD-L1 x VEGF-A bispecific antibody designed to enhance anti-tumor immunity and normalize tumor vasculature. By anchoring to PD-L1-expressing cells in the TME, it localizes VEGF-A blockade, aiming to reverse immune suppression and increases immune cell infiltration. Combining Pumitamig with Elfe-D aims to improve efficacy.
BNT324 MOA: Cytotoxicity; G2M cell cycle arrest; Cell apoptosis; Bystander killing effect; TME reactivation; B7H3+ angiogenic tumor vessels; B7H3+ tumor stromal cells. Pumitamig MOA: PD-L1 checkpoint blockade; Reverses T cell immunosuppression; VEGF-A neutralization; Vascular normalization; Immune cell infiltration and activation; Dendritic cell differentiation and maturation; Regulatory T cell proliferation.
Miao X, et al. AACR 2025 #6061; Heymach J, et al. WCLC 2025 #OA13.02
MD Anderson Cancer Center
———
[Slide 3]
Elfetabart drozuntecan (Elfe-D; BNT324/DB-1311)
Elfe-D (BNT324) is an investigational topoisomerase I-inhibitor-based anti-B7H3 ADC with a cleavable linker. Fc silenced. Selectively endocytosed into the lysosome of B7-H3 expressing cells. It has shown to have a bystander antitumor effect. In clinical studies demonstrated manageable safety and encouraging early clinical activity in patients with SCLC and NSCLC.
Cheng Y, et al. ESMO Asia 2024 #57O; Li C, et al. AACR 2023 #2967
MD Anderson Cancer Center
———
[Slide 4]
Elfe-D on SCLC and NSCLC: Efficacy summary
SCLC (n=73) ORR 56.2%: No prior IO (n=19) 11 (57.9); IO pretreated (n=54) 30 (55.6); Prior IO + no prior TOP1i 6 mg/kg (n=15) 7 (46.7); 9 mg/kg (n=34) 19 (70.4).
nsqNSCLC (n=41) ORR 22.0% (EGFRm n=14 ORR 21.4%).
sqNSCLC (n=25) ORR 16.0%.
Waterfall: Best change from baseline. Data cut-off: 27-Sep-2024. Cheng Y et al. ESMO Asia 2024. #57O
LCNEC remains an aggressive lung cancer subtype with no clear first-line standard. @thenasheffect from @StephensonCC reviewed the rationale for LAG-3 targeting and biomarker-driven approaches. #DAVALung
[Slide 1]
Aggressive Biological Behavior of LCNEC
- LCNEC constitutes 3-5% of lung cancer
- LCNEC displays a small-cell lung cancer-like clinical phenotype and biological behavior
- 5-year overall survival (OS) rate in the advanced stage of approximately <10% (SEER database)
- LCNECs seem to have higher FDG uptake than the typical well-differentiated neuroendocrine cancers, which is thought to be due to the higher expression of glucose transporter 1 (GLUT1)
- No first-line standard of care therapies (extrapolation from NSCLC or SCLC treatments)
Huang et al. BMC Cancer 2023
———
[Slide 2]
Genomic and Transcriptomic Subtyping of LCNECs
High-grade neuroendocrine lung tumors: LCNEC (Type I LCNECs, Type II LCNECs), SCLC (SCLC-P)
Type I LCNEC has a mutational pattern similar to NSCLC but gene expression profiles typical of SCLC, whereas type II LCNEC has a mutational pattern of SCLC but low expression of neuroendocrine markers, similar to NSCLC
Genomic profile: Type I TP53mut + STK11/KEAP1mut; Type II TP53mut + RB1mut; SCLC TP53mut + RB1mut
Transcriptional profile: Type I ASCL1high DLL3high NOTCHlow; Type II ASCL1low DLL3low NOTCHhigh; SCLC ASCL1high DLL3high NOTCHlow
Neuroendocrine profile; NOTCH profile immune profile; Neuroendocrine profile; Cellular respiration and metabolism; Cell cycle, mitosis
George J et al Nature Comm 2018; Rekhtman N et al. CCR 2016
———
[Slide 3]
LAG-3 as a Targetable Immune Checkpoint
- Cell surface receptor expressed on immune cells, including T cells, T reg cells, and a subset of NK cells, and binds to FGL1 on tumors
- LAG3 is co-expressed with PD-1 on TILs and acts together to disrupt immune responses to cancer cells
- Functions as an inhibitory immune checkpoint and is involved in tumor-mediated T cell exhaustion
- Combination therapy of nivolumab (anti-PD1) and relatlimab (anti-LAG3) can restore immune cell function and is approved for treating melanoma (FDA approved)
(Diagram: APC, MHCII, LSECtin, Lag-3, CD4+ T cell, CD8+ T cell or NK cell)
———
[Slide 4]
Conclusions
- LCNEC demonstrates a tumor-intrinsic FGL-1 high phenotype nominating FGL1/LAG3 as a potential immune evasion mechanism
- Likely Spatial proximity of LAG3+ T-cells to FGL1-high tumor cells, and reciprocal compartmentalization of FGL1 vs. LAG3 (single cell RNA seq) suggests a plausible functional ligand-receptor immune-suppressive niche
- Need for biomarker-guided therapies in prospective trials for LCNEC
With p53 alterations nearly ubiquitous in SCLC, Dr. @drshieldsmd from @IUCancerCenter discussed how p53 reactivators and MCL-1 inhibitors may offer a rational combination approach. #DAVALung
[Slide 1]
Nearly Ubiquitous p53 Alterations in SCLC
[Genomic landscape mutation matrix: Mutation frequency (%); TP53 highest frequency; genes listed include TP53, KMR2E1, RB1, PTEN, PIK3CA, BRAF, NOTCH1, NOTCH2, NOTCH3, NOTCH4, EP300, CREBBP, ASPM, ADAM17, PTGFRN, FBXW7, COBLL1, MYCL1, FMN2, and others. Mutation types: Missense, In frame indel, Rearrangements, C:G>G:C, C:G>A:T; Splice site, Nonsense, Frameshift, A:T>C:G, A:T>T:A, A:T>G:C; Synonymous / Nonsynonymous]
George et al. Nature 2015.
———
[Slide 2]
APR-246 Leads to Induction of Apoptosis with BAK Cleavage
[Western blot H524: 24 hours and 48 hours; DMSO, 1uM, 5uM lanes]
Cleaved PARP 89 kDa
Cleaved Caspase-3 19, 17 kDa
Vinculin 124 kDa
BAK 25 kDa
Vinculin 124 kDa
BAX 20 kDa
Vinculin 124 kDa
[Schematic: Mitochondria; MCL1; APR-246 (Eprenetapopt); Mutant p53; WT p53; Apoptosis]
———
[Slide 3]
Unbiased 500-Compound Screen Identifies MCL-1 as Potential Combinatorial Agent with APR-246
[COCTAIL Drug Screen schematic; Input H82 H524; Output heatmaps]
[Dose-response viability curves: A) HBEC30KT; B) H146; C) H82; D) H524 - DMSO / DMSO + APR-246 1 uM; Viability (%) vs Drug (uM)]
———
[Slide 4]
Questions Remain
- What driver(s) cleaves BAK? Is this event required for apoptosis?
- How do MDK and NPNT induce acquired APR-246 resistance? Could integrins play a role in inducing proliferation?
- Synergy studies with combination of rezatapopt and MCL-1i (underway)
Relapsed SCLC through a multi-omics lens. Brendan Knapp (@washumedicine) reviews paired-sample data (n=54): platinum/APOBEC signatures in >80%, MYC/MYCN/MYCL gains in 22%, and ASCL1-high dominance. ASCL1 high was most common SCLC type (70%) #DAVALung
[Slide 1]
Multi-omic evaluation of relapsed SCLC
Treatment-naive (n=27): WGS 18, WES 27, RNAseq 12
Pair: WGS 18, WES 26, RNAseq 6
Relapse (n=54): WGS 28, WES 54, RNAseq 31
Mutation oncoprint (Relapse [N=54] vs TN [N=27]) genes top to bottom: KMT2D, SYNE1, LRP1B, USH2A, ZFHX4, MUC16, CSMD3, RYR2, RB1, TTN, TP53. Percent of cases. Legend: Frame_Shift_Del, Frame_Shift_Ins, In_Frame_Del, Missense_Mutation, Multi_Hit, Nonsense_Mutation, Splice_Site.
No significant difference in individual mutations between treatment naive (TN) and relapsed SCLC.
Unpublished data, under revision. Slide 271
———
[Slide 2]
Mutation signature analysis of relapsed SCLC
Stacked bar chart: Fraction of mutations (0-1.00) across Relapsed SCLC Samples (SCLC8, SCLC30, SCLC59, ... SCLC54).
Signatures:
- SBS4 Exposure to tobacco (smoking) mutagens: Samples 46; Pct. of samples 85.2%
- SBS35 Prior chemotherapy treatment with platinum drugs: Samples 44; Pct. of samples 81.5%
- SBS13 APOBEC Cytidine Deaminase (C>G): Samples 45; Pct. of samples 83.3%
- SBS5 Unknown: Samples 47; Pct. of samples 87.0%
- Other: Samples 53; Pct. of samples 98.1%
Markers: Never smoker (diamond), Former smoker (triangle), Never smoker with marijuana (square).
Platinum exposure and APOBEC (dysfunctional cytidine deaminase) signatures were found in >80% relapsed SCLC samples (vs 0% treatment naive). Slide 272
———
[Slide 3]
Transcriptomic features of relapsed SCLC
- ASCL1-high was most common SCLC subtype (70%)
- No subtype dominance switching was observed in paired samples
- Differential gene expression between chemo-responders vs non-responders and TN vs R-SCLC; e.g. WNT signaling (APC2) and immune evasion (IDO1)
Volcano plots: (left) TN vs Relapse [-log10(pvalue) vs log2FoldChange] highlighting APC2, IDO1 and others (IGF2, TTLL10, TCHH, MUC13, C1QL2, etc.); (right) Responder vs DNRp highlighting KIAA2012, FOS, HLA-B, COL9A3, SLC17A1, EGR3, RBFOX3, PLG, ALOX15, G6PC1, CYP3A4, APOA2, PKD1L3, AQCXL, GALNTL6, MSX2, IL26RA, SLITRK6, UGT2A1, GRRH.
———
[Slide 4]
Neoantigen landscape of SCLC
- Level of HLA gene expression inversely correlated with neuroendocrine expression signature
- Neoantigen loss was observed in 6/18 paired samples at relapse
A. Neoantigen count (0-400) for Treatment naive (TN, blue) vs Relapse (R, pink); Paired samples (SCLC1-SCLC45) and Non-paired samples.
B. NE ssGSEA score vs HLA expression (TPM): R = -0.45, p = 0.014.
C. Gene / Neoantigens / Patients: TP53 30 / 21 (47.73%); RYR2 29 / 15 (35.09%); CSMD3 25 / 13 (29.55%); USH2A 25 / 12 (27.27%); PAPPA2 14 / 8 (18.18%); CSMD2 9 / 7 (15.91%); RB1 9 / 6 (13.64%). Slide 277
Lurbinectedin had a 35% response in phase 2 relapsed SCLC, yet biomarkers remain key. @drshieldsmd (@IUCancerCenter) spotlights ISL1 as a top proteomic hit linked to response and ISL1-high sensitivity. #DAVALung
[Slide 1]
Tangible Progress in SCLC
FDA Approvals in SCLC (timeline 2020-2026)
2020: Lurbinectedin*; Trilaciclib
2024: Tarlatamab*; Durvalumab post CCRT in LS-SCLC
2025: Tarlatamab; Lurbinectedin + Atezolizumab in 1L maintenance
*accelerated approval based on Phase II study
Indiana University Melvin and Bren Simon Comprehensive Cancer Center
———
[Slide 2]
Lurbinectedin
Derived from the sea squirt
Chemotherapy that binds minor groove of DNA
Phase 2 single-arm basket trial
Given every 3 weeks as an IV
2.6 or 3.2 mg/m2 dose
35% of patients on study responded
Accelerated FDA approval (June 2020)
Waterfall plot of duration of response by best objective assessment; Need: Predictive biomarkers to lurbinectedin
Trigo, et al. Lancet Oncol. 2020.
———
[Slide 3]
Durable Responders to Lurbinectedin Exist
A. Timeline: Day -30 Right hilar mass, liver, and adrenal lesions; Day -2; Day +1 SCLC; Day +19 Cycle 1, day 1, carboplatin, etoposide, and atezolizumab; x14; Day +574 Cycle 1, day 1, lurbinectedin; Day +689 Right thalamic brain metastasis.
B. CT images: Day +1 Diagnosis of ES-SCLC; Day +122 After 4 cycles chemoimmunotherapy; Day +566 Progressive disease on maintenance atezolizumab; Day +615 Interval response after cycle 2 of lurbinectedin; Day +1,193 Long-term response after cycle 24 of lurbinectedin.
In 2026: This patient is alive, not on active therapy, & NED x 4 years
Indiana University Melvin and Bren Simon Comprehensive Cancer Center
———
[Slide 4]
What is ISL1?
- Islet-1 is a LIM1 homeobox domain transcription factor
- Required for epigenetic regulation of cell fate, including pancreatic lineages & tracheoesophageal differentiation
- Directly interacts with NKX2.1 (TTF-1) and SOX family proteins
- Limited data in SCLC noted ISL1 & FOXA2 in the "ON" state in a data-driven TF network model
- ISL1 may coordinate the transition from a non-NE to NE state
Indiana University Melvin and Bren Simon Comprehensive Cancer Center
Dr. @Oser_Lab from @DanaFarber presented compelling translational data showing that SCLC transcription factor subtype influences both response and acquired resistance to tarlatamab. #DAVALung
IMpower133
[Slide 1]
Patient Cohort: DFCI Patients Receiving Standard of Care Tarlatamab from September 2024 to January 2026
ChIP-seq from cell-free circulating chromatin in plasma (Baca et al. Nature Medicine 2023)
-SCLC an ideal cancer type for this approach
-high cfDNA tumor fraction
-challenging to biopsy and not clinically indicated to biopsy
-cancer defined by lineage transcription factor epigenomic signatures
46 patients
22 with clinical benefit
18 no clinical benefit
(a) 46 Post Platinum ES-SCLC Patients; Tarlatamab Infusion C1D1 C1D8 C1D15, CxDx, First Evaluation C3D1; OligoPD, PD -> No clinical benefit n=18; NE -> Other n=6; PR, SD -> Clinical benefit n=22. n = 43, 20, 39, 22, 17. 167 Plasma Samples Collected. cfChIP-seq -> cfMeDIP-seq -> LPWGS (Gain/Neutral/Loss; Tumor fraction). H3K27ac, H3K4me3, H3K36me3.
(b) Time on treatment (months) swimmer plot 0-16; Legend: Death, Epigenomic profiling, Oligoprogression, Partial response, Progressive disease, Stable disease; No clinical benefit, Clinical benefit, Other.
———
[Slide 2]
The ASCL1 Subtype is Correlated with Tarlatamab Response whereas the NEUROD1 and POU2F3 Subtypes are Inherently Resistant
34 patients: 20 ASCL1, 10 NEUROD1, 4 POU2F3
Genes tracks: ACTB (chr7:5,564,779-5,572,232), CHGA (chr14:93,387,495-93,403,630), DLL3 (chr19:39,987,587-40,001,109), ASCL1 (chr12:103,349,452-103,356,291), NEUROD1 (chr2:182,531,022-182,547,244), NHLH1 (chr1:160,334,861-160,344,636), POU2F3 (chr11:120,105,347-120,192,654). Rows: SCLC-A, SCLC-N, SCLC-P, Healthy.
Progression-free survival KM: SCLC-A (ASCL1), SCLC-N (NEUROD1), SCLC-P (POU2F3); p = 0.0054; at-risk 20/10/4.
Clinical benefit contingency (Fisher's test): SCLC-A vs Others Yes 16/2 No 4/12 p=0.0003; SCLC-A vs SCLC-N Yes 16/2 No 4/8 p=0.0041; SCLC-A vs SCLC-P Yes 16/0 No 4/4 p=0.0066; SCLC-N vs SCLC-P Yes 2/0 No 8/4 p=1.0.
DLL3 mRNA Expression from 271 Primary Human SCLCs: DLL3 log2(TPM+1) ASCL1 vs NEUROD1 vs POU2F3, ****.
-SCLC subtypes were assigned by applying a Random Forest classifier trained on IMpower133 tumor RNA-seq data (271 samples) to APEX-inferred plasma gene expression.
———
[Slide 3]
Acquired Resistance to Tarlatamab in Human SCLC: Selection for the NEUROD1 Subtype with DLL3 Loss
Patient 6527 swimmer: Tumor fraction 0.41, 0.0, 0.0, 0.09, 0.18, 0.57, 0.57 across Months 0-7.5; Legend: Death, Epigenomic profiling, Partial response, Progressive disease, Stable disease.
APEX at acquired resistance vs baseline scatter (C9D1 z-score vs C1D1 z-score): labels INSM1, GAPDH, NEUROD4, MYCN, CHGA, NHLH1, TCF15, NEUROD1, ASCL1, PHOX2B, MYC, MYCL, YAP1, POU2F3, DLL3, FOXA2.
Gene tracks ACTB, ASCL1, NEUROD1, DLL3 for C1D1 and C9D1.
Signature score (mean log2TPM) over timepoints C1D1, C1D15, C3D1, C5D15, C7D15, C9D1 for SCLC-A and SCLC-N; ns, ns, ns, **, *, ****.
Also observed in patient 6940.
———
[Slide 4]
Transcription Factor Subtype Governs Response and Resistance to DLL3-Directed T-Cell Engagement in Small Cell Lung Cancer
Schematic: ASCL1-high DLL3-high -> In vivo selective pressure -> NEUROD1-high DLL3-low; Cell Intrinsic selection; CD3+ T cells; Cell Extrinsic selection; Tex, Treg; T cell exhaustion, Regulatory T cells. Tumor size vs Time after Tarlatamab. Legend: Tarlatamab, DLL3, T cell inhibitory molecules.
Vasseur* Saito* et al. BioRxiv 2026 https://doi.org/10.64898/2026.04.02.715020
How common is Lambert-Eaton myasthenic syndrome in veterans with SCLC? @kelleymic from @DukeCancer shared VA registry data assessing prevalence, outcomes, and pharmacologic treatment patterns. #DAVALung
[Slide 1]
Background
- Lambert-Eaton Myasthenic Syndrome (LEMS) is a rare autoimmune disorder characterized by muscle weakness, fatigue, and autonomic dysfunction
- 50-60% of LEMS are paraneoplastic, mostly with SCLC, which express P/Q type VGCC
- Amifampridine is FDA approved for LEMS
- US Veterans have higher rates of SCLC incidence due primarily to increased tobacco use
- ICI use has been associated with LEMS
(Diagram: Nerve stimulus, ACh, K+ channel, Voltage gated Ca++ channel Ab, ACh receptors, Muscle)
———
[Slide 2]
Methods
- Patients identified from VA Corporate Data Warehouse and VA Cancer Registry System
- Study period: October 1, 1999 to December 31, 2024
- LEMS cohort: both SCLC diagnosis and LEMS diagnosis
- LEMS diagnosis:
- ICD 9/10 codes for LEMS, myasthenic syndrome, or myoneural disorders
- LEMS confirmed via text matching in hematology, oncology, or neurology notes
- Descriptive statistics were used for frequency of LEMS
- Cox proportional hazards ratio (HR) and Kaplan-Meier survival model used for survival analyses
- Analyses performed using R
———
[Slide 3]
Results: Overall Survival
Strata: SCLC only vs SCLC + LEMS
mOS: 7.8 v 12.0 m
OS HR: 0.74 (95% CI: 0.54 - 0.99)
p = 0.00022
Number at risk: SCLC only 25882, 10502, 4757, 2917, 2109; SCLC + LEMS 78, 51, 26, 19, 16 (at 0, 10, 20, 30, 40 months since diagnosis)
———
[Slide 4]
Conclusions
- Lambert-Eaton Myasthenic Syndrome (LEMS) is rare in Veterans with SCLC
- No increase in prevalence of LEMS was seen since approval of atezolizumab (2019) and durvalumab (2020) for SCLC
- LEMS is associated with a modest improved survival in SCLC
- LEMS is uncommonly treated with amifampridine in VA
Are TAMs bad in SCLC? IMforte set a new bar in ES-SCLC maintenance: atezolizumab+lurbinectedin improved PFS, OS and QoL vs chemo-IO alone. W. Jeffrey Petty (@AtriumHealth) explores TAM biology and real-world use. #DAVALung
IMforteIMpower133
[Slide 1]
IMforte vs IMpower
INV-PFS (%) KM curve - IMforte vs IMpower 133; landmarks at 12 Mo and 24 Mo.
Forest plot IRF-PFS (Favours lurbi + atezo vs Favours atezo), Unstratified HR (95% CI):
BEP: n=412, HR 0.55 (0.44, 0.69)
PD-L1 status by SP263:
IC or TC >=1%: n=193, 0.66 (0.48, 0.93)
IC or TC <1%: n=219, 0.43 (0.32, 0.58)
IC or TC >=5%: n=57, 0.91 (0.48, 1.73)
IC or TC <5%: n=356, 0.51 (0.40, 0.65)
Paz-Arez, ESMO IO 2025
———
[Slide 2]
TAM biomarker provides proof of principle
IRF-PFS and OS by TAM/T-eff
- Patients with high TAM/high T-eff in the atezolizumab arm had a numerically shorter IRF-PFS and OS (mPFS: 2.63 months and mOS: 12.25 months) versus those with low TAM/high T-eff (mPFS: 4.76 months and mOS: 16.39 months), reiterating the potential inhibitory effect of TAMs with atezolizumab treatment.
- Numerical trends in IRF-PFS and OS suggest that lurbinectedin may overcome TAM-mediated resistance to atezolizumab.
High TAM/high T-eff: IRF-PFS Atezo 2.63 vs Lurbi+Atezo 5.59, HR 0.64 (0.4, 1.03); OS Atezo 12.25 vs Lurbi+Atezo 22.20, HR 0.55 (0.29, 1.01).
Low TAM/high T-eff: IRF-PFS Atezo 4.76 vs Lurbi+Atezo 6.97, HR 0.82 (0.4, 1.65); OS Atezo 16.39 vs Lurbi+Atezo 12.75, HR 0.95 (0.42, 2.14).
Summary: TAM low OS = 16.4 mo -> TAM high = 12.3 mo -> TAM high + lurbi = 17.2 mo
———
[Slide 3]
Rationale for IMforte: Lurbi attacks TAMs
[IHC CD68 Untreated vs Treated, quantification bar chart ***, 50 um]
LURBINECTEDIN: Inhibition of cell migration; Induction of apoptosis; Reduced cancer-related inflammation. Tumour -> CCL2 -> Monocyte -> TAM; CCL2, CXCL8, VEGF.
Cancer Cell 2013 23, 249-262 DOI: (10.1016/j.ccr.2013.01.008); Br J Cancer. 2017 Aug 22;117(5):628-638
———
[Slide 4]
Rationale for IMforte: TAMs are bad in small cell
[Myeloid differentiation schematic: Bone marrow/spleen -> Bloodstream -> Tumor site; Mo-MDSC, Monocytes, PMN-MDSC, Neutrophils, LyGC CD11b, CD16, TAMs, F4/80, MHC II, CD68; increasing requirement for resistance to apoptosis (BCL-A1), increased APO1 expression, increasing requirement for survival factors/cytokines]
TAMs (CD68+) are the PD-L1 expressing cells in SCLC. [IHC panels C: PD-L1; D: CD68]
Nature Communications volume 7, Article number: 12160 (2016) doi:10.1038/ncomms12160; European Journal of Cancer Volume 51, Issue 3, Pages 421-426
Concurrent or sequential? Dr James Urbanic (@UCSDHealth) discusses lung cancer trial reveals on radiation & checkpoint therapy timing across early-stage, stage III, oligometastatic disease & SCLC, highlighting impact of field size, host vulnerability & duration of IO exposure
[Slide 2]
STAGE I
Early-Stage NSCLC: A Signal That Didn't Survive Phase III
I-SABR - Phase II: 53% -> 77% 4-yr event-free survival, SBRT alone vs. + nivolumab (HR 0.42). Randomized phase II signal: adding nivolumab to SBRT improved EFS across all subgroups.
SWOG/NRG S1914 - Phase III: No OS Benefit. Grade >=3 AEs: 12% vs. 2% (1 grade 5 respiratory failure). Daly et al., ASCO 2025. Neoadjuvant/concurrent/adjuvant atezolizumab + SBRT vs. SBRT alone, high-risk stage I-II NSCLC.
Why did a "small field" trial fail?
- Eligibility to 7 cm, central tumors allowed - not uniformly tiny fields
- Medically inoperable population - limited pulmonary reserve by definition
- ~6 months of systemic IO exposure - pneumonitis risk independent of field
- Small absolute effect size to chase - local control already >85% with SBRT alone
Footer: Timing of RT + Immunotherapy in Lung Cancer | J. Urbanic, MD | UC San Diego Moores Cancer Center
———
[Slide 3]
Clinical Evidence Base: SBRT Immunopriming in NSCLC
Convergent evidence across four independent trials
Altorki / Weill Cornell: NCT02904954 | Lancet Oncol 2021. Stage I-IIIA resectable | 8 Gy x 3 GTV only. MPR 53% vs 7%. 8-fold increase over durvalumab alone. pCR 27% | EGFR wt subgroup MPR 70%.
SACTION01: NCT05319574 | Lancet Respir Med 2024. Stage IIA-IIIB (EGFR wt) | 8 Gy x 3 GTV only. MPR 76%, pCR 52%. SBRT added to full chemoimmuno backbone; most direct precedent for CHIO3-PRIME.
SQUAT / WJOG 12119L: JTO 2025;20:1097 | Pathologic N2 specific. Stage IIIA/B N2+ (identical to CHIO3-PRIME) | 50 Gy/25 fx CRT + durvalumab (concurrent, not SBRT immunopriming). MPR 63%, pCR 23%. Conventional CRT - different mechanism. Anchors Arm A control rate at ~40-50%.
CheckMate 77T (N2 subgroup): Nature Cancer 2026. Stage III N2 resectable | No SBRT (reference). 1-yr EFS: 70% vs 45%. HR 0.46 in N2 subgroup. pCR 22% vs 5.6% | Phase III anchor.
Footer: KEYNOTE-671 5-yr OS update (ASCO 2025): 64.6% (periop pembro) vs 53.6% (placebo), HR 0.74 - anchors Phase III OS target
———
[Slide 4]
STAGE III, UNRESECTABLE
Concurrent IO Fails - Three Independent Phase III Trials
PACIFIC-2: No PFS/OS Benefit. Concurrent durvalumab + CRT -> consolidation, vs. the PACIFIC regimen. More toxicity and treatment discontinuation.
CheckMate 73L: 23% vs 10%. Immune-mediated pneumonitis with concurrent nivolumab +/- ipilimumab vs. durvalumab consolidation. 15 treatment-related deaths from pneumonitis.
EA5181: No OS Benefit. Concurrent + consolidative durvalumab vs. consolidation alone. Confirms: earlier isn't better.
Three different concurrent strategies, three negative trials: consolidation durvalumab after CRT (PACIFIC) remains the standard of care.
Footer: Timing of RT + Immunotherapy in Lung Cancer | J. Urbanic, MD | UC San Diego Moores Cancer Center
Relapsed SCLC remains a difficult-to-treat setting. Dr. Zhonglin Hao from @UKMarkey discussed a novel epigenetic strategy combining tazemetostat, topotecan, and pembrolizumab. #DAVALung
[Slide 1]
Enhancer of Zeste Homologue 2 (EZH2).
- Catalytic subunit of the polycomb repressive complex 2 (PRC2).
- Add 3 methyl groups to histone H3 lysine 27 (H3K27me3).
- Control gene expression by cooperates with other epigenetic silencing enzymes.
UK HealthCare Markey Cancer Center.
———
[Slide 2]
Diagram: Tazemetostat / EZH2 inhibition; MHC-I antigen presentation; T-cell activation and cytokine secretion; DNA replication arrest and cell death; SLFN11.
- Can EZH2 inhibitors, by restoring SLFN11 expression, augment topotecan response and prevent resistance.
- Can EZH2 inhibitors, by alleviating MHC-I transcriptional repression, help potentiate immune responses and increase immune infiltration.
UK HealthCare Markey Cancer Center.
———
[Slide 3]
Tazemetostat, is a methyltransferase inhibitor.
- Preclinical data showed: depleted EZH2 expression in animal M. Highly selective for EZH2 over other methyltransferases and EZH1.
- Approval- (accelerated): Adult and Pediatric Locally advanced/metastatic epithelioid sarcoma. Adult Relapsed (after 2 or more lines) FL (with EZH2 mutation/without mutation- No other option).
- Safety Epithelioid sarcoma (>20%)- Pain, fatigue, nausea, anorexia, vomiting, constipation. FL (>20%)- Fatigue, Upper respiratory infections, MSK pain, nausea, abdominal pain. DLT grade 4 thrombocytopenia at highest dose (1600 mg BID). Mesothelioma- (>20%)- Fatigue, anorexia, cancer pain, nausea, dyspnea, G3/4- Hyperglycemia (7%), Hyponatremia (7%), anemia (5%). Combination with atezolizumab: anemia and fatigue. Grade >=3 AEs were anemia, thrombocytopenia and neutropenia.
UK HealthCare Markey Cancer Center.
———
[Slide 4]
PRIMARY OBJECTIVES:
Dose Escalation cohort (Tazemetostat + Topotecan (C1)): 1. MTD 2. RP2D.
Dose Expansion cohort (Tazemetostat + Topotecan + Pembro): 1. Safety/Tolerability.
SECONDARY OBJECTIVES:
- Efficacy outcomes (PFS, DOR, OS)
- N=33-39. 18 (Escalation) Max 24 and 15 (Expansion)
UK HealthCare Markey Cancer Center.
Dr. @BZhangMD@UTMDAnderson presented the latest evidence supporting tarlatamab in relapsed/refractory SCLC, covering DeLLphi-304 outcomes, CNS efficacy, toxicities, and the role of biomarkers in guiding treatment. #DAVALung
FucGM1 is overexpressed in ~68% of SCLC. Sid Devarakonda (@WSUPullman) reviews atigotatug (BMS-986012)+nivolumab, including phase I/II ES-SCLC signals: ORR 71% in 1L and 13.7% in phase III relapse. #DAVALung
[Slide 1]
What are glycolipids?
Ganglioside structures shown (illustrated with sailboat analogy: One-Mast, Two-Mast, Three-Mast): GM1, GM2, GM3, GM4, GD3, Galactocerebroside (GC); GD1a, GD1b, GT1b, GQ1b, Sulfatide. Legend: galactose, glucose, sialic acid, N-acetyl-galactosamine, ceramide (Cer).
“Fucosylated” monosialotetrahexosylganglioside = FucGM1
• Over-expressed in ~68% of SCLCs
Moriguchi et al. IIMS, 2023; Ponath et al. Clin Can Res, 2018
———
[Slide 2]
Atitotatug (BMS986012)
• Fucosyl-GM1 is a monosialoganglioside with limited expression in normal tissues but high expression on the surface of tumor cells in SCLC
• BMS-986012 is a nonfucosylated, first-in-class, fully human IgG1 mAb that binds to fucosyl-GM1 with high affinity and specificity
• Lack of fucosylation is associated with higher binding on NK cells and increased ADCC
• The current study presents the preliminary safety findings from a phase 1/2 trial of BMS-986012 combined with platinum/etoposide, followed by BMS-986012 monotherapy maintenance in previously untreated patients with extensive-stage SCLC
Mechanism: Anti-fucosyl-GM1 → tumor cell death, ADCC-mediated tumor cell death, Complement-dependent cytotoxicity (Phagocyte, Tumor cell, NK cell).
A: FcγRIIIA-CHO Binding; B: ADCC (BMS-986012 IgG1 nf vs 7E4 Ab IgG1).
Ponath et al. Clin Can Res, 2018
———
[Slide 3]
Phase I/II in ES-SCLC: Relapsed setting — Study design
Key eligibility criteria
• Patients ≥ 18 years old with histologically or cytologically confirmed pulmonary SCLC
• No prior treatment with anti-PD-1, anti-PD-L1, anti-PD-L2, anti-CD137, anti-CTLA-4 or any other antibody targeting T-cell costimulation or checkpoint pathways
• ECOG PS 0-1
• Part 1: ≥ 1 prior line of therapy (dose escalation); Part 2: relapsed or refractory to only 1 prior line of therapy (dose expansion)
Part 1: dose escalation IV Q3W: BMS-986012 400 mg + nivolumab 360 mg (n=8); BMS-986012 1000 mg + nivolumab 360 mg (n=8)
Part 2: dose expansion IV Q3W: BMS-986012 400 mg + nivolumab 360 mg (n=13)
Primary endpoint: Safety
Secondary endpoints: investigator-assessed ORR, median DOR, median PFS
Exploratory endpoint: median OS
Data cutoff: July 22, 2020
Platinum sensitive relapses: 69%; N=29; 86% received 1 prior line of treatment
Ready et al. WCLC 2020
———
[Slide 4]
Interim analysis of a randomized study of 1L BMS-986012 (anti-fucosyl-GM-1) with Chemotherapy and nivolumab in ES-SCLC
Authors: Shunichi Sugawara, Ewa Kalinka, Idris Bahce, Alejandro Navarro, Neal Ready, Quincy Chu, Anne Sibille, Mariano Provencio, T. Jeroen Hiltermann, Melissa Johnson, Tudor Ciuleanu, Rafal Dziadziuszko, Antonio Santo, Yinan Zhang, Yu Liu, Rafael Sarmiento, Sarah Tannenbaum-Dvir, Laureen S. Ojalvo, Jiaju Wu, Kenneth O'Byrne
Key eligibility criteria: Age ≥ 18 years; Histologically/cytologically confirmed ES-SCLC; No prior systemic therapy/newly diagnosed; ≥ 1 measurable lesion; ECOG PS (0/1). Stratification: Liver metastases (yes/no); ECOG PS (0/1).
R 1:1 — Induction (4 cycles, 1 cycle = 21 days): Atigotatug 420 mg + NIVO 360 mg IV Q3W + chemo; Maintenance (2 years): Atigotatug 560 mg + NIVO 480 mg IV Q4W vs NIVO 360 mg IV Q3W + chemo → NIVO 480 mg IV Q4W.
Primary endpoints: Safety; PFS by BICR (per RECIST v1.1). Secondary endpoints: OS; ORR, DOR and TTR by BICR; PFS by investigator; Immunogenicity. Ad hoc exploratory endpoint: OS by baseline brain metastases.
• The prespecified interim analysis took place when ~75% of PFS information was available: data cutoff August 28, 2023
• An additional analysis took place after longer follow-up to allow a more meaningful assessment of OS: data cutoff February 26, 2024
Sugawara et al. ESMO 2024
The final morning at #DAVALung covers patient quality of life, vaccines & cellular therapy, neuroendocrine carcinomas, mesothelioma, AI/ML in lung cancer, and novel synergistic agents for ICI response. A comprehensive close to an outstanding summit. 🫁
🔗
Dr. @rdhalljr from @uvaCancerCenter discussed real-world data on tarlatamab in relapsed/refractory SCLC, highlighting outcomes comparable to clinical trials, and insights into CRS and ICANS management. #DAVALung
A new angle on SCLC biology Dr. @Oser_Lab from @DanaFarber, reviewed how POU2F3 dependency may be therapeutically exploited through SMARCA4/2 inhibition in a defined SCLC subtype. #DAVALung
[Slide 1]
The POU2F3 Subtype is Highly Dependent on POU2F3
(SCLC molecular subtype heatmap: ASCL1 (A) ~60%, NEUROD1 (N) ~20%, POU2F3 (P) ~10%, Inflammatory/MHC class I positive (I) ~10%)
POU2F3 dependency (dependency plot by lineage): Lung (133); Lung Carcinoid (1); Mesothelioma (17); NSCLC (94); SCLC (21) — POU2F3 Dependency!
Direct approaches to drug POU2F3 are challenging!
Huang et al. Genes Dev 2018; Wu et al. Nature 2022
———
[Slide 2]
Genome-wide CRISPR/Cas9 Screen Identifies Candidate POU2F3 Regulators
Day 0: Infect NCI-H1048 cells expressing endogenous POU2F3-DCK* with Cas9 whole genome sgRNA library (Brunello CP0043)
Day 9: BVDU 10 uM (arm 1) or Untreated (arm 2)
Day 16: Harvest Genomic DNA for Deep Sequencing; Compare sgRNA enrichment at Day 16 in the BVdU arm to the untreated arm
BVdU vs. Untreated at Day 16 (Target Z-score vs Log2FC by Gene Symbol; hits for validation include DCK, EBF1, POU2F3, SMARCA4; all other genes; control sgRNAs)
CP0043 includes >=77,741 targeting sgRNAs, 1000 control sgRNAs; BVdU vs. Untreated 7 days after BVdU treatment; Apron analysis; 2 biological replicates
Duplaquet*, So*, et al. Cancer Cell 2024
———
[Slide 3]
All POU2F3-Positive SCLC Cell Lines are Highly Sensitive to Clinical Grade SMARCA4/2 Inhibitors
(Western blots: POU2F3, SMARCA4, SMARCA2, beta-ACTIN across cell lines NCI-H1048, NCI-H211, NCI-H526, COR-L311; agents FHD-286, AU-15330, BRM014)
(Dose-response curves; EC50 nM table by cell line for FHD-286, AU-15330, BRM014)
SMARCA4/2 Inhibitors; ncBAF, cBAF, PBAF; mSWI/SNF Complexes
All POU2F3+ cell lines are highly dependent on the mSWI/SNF complex!
In contrast, ASCL1+ and NEUROD1+ cell lines are inherently resistant to mSWI/SNF inhibition
Duplaquet*, So*, et al. Cancer Cell 2024
———
[Slide 4]
Translational Strategy for SMARCA4/2 Inhibition in POU2F3-Positive SCLCs
Screen for POU2F3-positive tumors by IHC -> Enroll in Clinical Trial
(IHC panel: H&E, Ki-67, CD56, INSM1, ITF-1, POU2F3)
SMARCA4/2 Inhibitor for POU2F3-Positive SCLC
ClinicalTrials.gov ID: NCT07551635
Sponsor: Dana-Farber Cancer Institute
Information provided by: Jacob Sands, MD, Dana-Farber Cancer Institute (Responsible Party)
Last Update Posted: 2026-04-27
Great insights from @BZhangMD, @UTMDAnderson, on DLL3 as an emerging pan-neuroendocrine carcinoma target and the potential role of Alveltamig (ZG006) in SCLC and NEC. #DAVALung
[Slide 1]
DLL3 as a pan-neuroendocrine carcinoma target
a. DLL3 Total expression in tumor cells (Total H-Score)
P-NEN: Lung - Small cell carcinoma; Lung - Large cell neuroendocrine carcinoma; Lung - Combined histology
EP-NEN: Uterine cervix - Small cell carcinoma; Skin - Merkel cell carcinoma; Prostate - AVPC = NEC; Bladder - Small cell carcinoma; Uterine cervix - Combined histology; Uterine cervix - Large cell neuroendocrine carcinoma; Head and Neck - Neuroendocrine carcinoma; Thyroid - Medullary; Adrenal - Adenoma; Neuroblastoma - Olfactory; Neuroblastoma - Conventional; Pancreas - Neuroendocrine tumor; Head and Neck - Paraganglioma; Adrenal - Adenocortical carcinoma; Prostate - AVPC nonNEC; Adrenal - Pheochromocytoma
Serrano et al, npj Precision Oncology, 2024
———
[Slide 2]
Alveltamig (ZG006) phase 2 study in neuroendocrine carcinoma
DLL3 TC* >= 50%: ZG006 10 mg Q2W (N=18); ZG006 30 mg Q2W (N=16)
DLL3 TC* < 50%: ZG006 10 mg Q2W (N=12); ZG006 30 mg Q2W (N=14)
All: ZG006 10 mg Q2W (N=32); ZG006 30 mg Q2W (N=32)
ORR, % (95% CI): 33.3 (13.3, 59.0) | 56.3 (29.9, 80.2) | 0 (0.0, 26.5) | 7.1 (0.2, 33.9) | 21.9 (9.3, 40.0) | 37.5 (21.1, 56.3)
PR, n (%): 6 (33.3) | 9 (56.3) | 0 | 1 (7.1) | 7 (21.9) | 12 (37.5)
DCR, % (95% CI): 50.0 (26.0, 74.0) | 75.0 (47.6, 92.7) | 16.7 (2.1, 48.4) | 42.9 (17.7, 71.1) | 40.6 (23.7, 59.4) | 62.5 (43.7, 78.9)
SD, n (%): 3 (16.7) | 3 (18.8) | 2 (16.7) | 5 (35.7) | 6 (18.8) | 8 (25.0)
PD, n (%): 7 (38.9) | 4 (25.0) | 10 (83.3) | 7 (50.0) | 17 (53.1) | 11 (34.4)
NE, n (%): 2 (11.1) | 0 | 0 | 1 (7.1) | 2 (6.3) | 1 (3.1)
Waterfall plots: DLL3 TC >= 50% and DLL3 TC < 50% (10mg Q2W, 30mg Q2W), Change from baseline SOD (%).
Presented by Dr. Chuanhua Zhao, ASCO 2026
———
[Slide 3]
Conclusion
- DLL3 is a pan-neuroendocrine carcinoma (NEC) target.
- Alveltamig (ZG006), a biparatopic DLL3 T cell engager, showed promising clinical efficacy in SCLC and NEC.
- Future direction: "SCLC is having an AGA NSCLC moment" - good problem to have?
- Biomarkers of response and resistance for DLL3 T cell engagers
- DLL3 may not be the best target for everyone: SEZ6, B7H3, TROP2...
DLL3 CAR-T moves into SCLC/LCNEC: LB2102 phase 1 tested 20 pts; at dose level ≥3, ORR was 28.6% and DCR 78.6%, with CRS 30% (all ≤G2). @BZhangMD (@UTMDAnderson) shares the data. #DAVALung
LB2102
[Slide 1]
LB2102 overview
LB2102 CAR-T Cell Design
- Chimeric antigen receptor (CAR): dual single-domain antibodies (sdAb) with high-affinity binding for DLL3
- dnTGFBR2 blocks TGF-b mediated signaling to SMAD2, leading to their increased activation, proliferation, and anti-tumor effector functions
CAR: CD8a Hinge, CD8a TM, 4-1BB, CD3z
dnTGFBR2: TGF-b, TRI, SMAD2
Oral abstract, no. 339 ASCGT Congress 2026
———
[Slide 2]
LB2102 First-in-human Phase 1 study
Part A: Dose escalation i3+3 Design (Nmax=36)
DL1 0.3 x10^6 -> DL2 1.0 x10^6 -> DL3 2.0 x10^6 -> DL4 4.0 x10^6 -> DL5 8.0 x10^6 -> DL6 12.0 x10^6 -> DL7 16.0 x10^6 (DL6 skipped based on safety data)
Cohort Expansion (N=2-17) Simon's 2-stage design (Not recruiting)
DL: Dose levels (CAR+ T cells/kg)
Study Flow Diagram: Screening (28 days) -> Bridging therapy -> Lympho-depletion -> CAR-T cell infusion -> Follow up
Key Eligibility Criteria:
- Unresectable small cell lung carcinoma (SCLC), large cell neuroendocrine lung carcinoma (LCNEC)
- >= 1 prior line of systemic treatment and have progressed after or have had an insufficient response
- Presence of >= 1 radiological measurable lesion
- ECOG 0 or 1 and adequate organ function
- No prior CAR-T or DLL3-targeted therapy
- No symptomatic brain metastases. Subjects with treated and stable brain metastasis are allowed
Study Objectives for Part A:
Primary Objective: To characterize the safety and tolerability of LB2102 and determine the recommended dose for expansion (RDE)
Secondary Objective: To evaluate the preliminary efficacy, pharmacokinetics and immunogenicity
Presented by Dr. Zhonglin Hao, ASCO 2026
———
[Slide 3]
LB2102 trial in progress
At DL3 and Above, ORR is 28.6%, DCR is 78.6%
Best change from baseline waterfall plot. Primary tumor type: SCLC (star), LCNEC (triangle). Dose Levels 1-7. Responses labeled PD, SD, PR across subjects.
UT MD Anderson. Presented by Dr. Zhonglin Hao, ASCO 2026
———
[Slide 4]
LB2102 trial in progress
Swimmer plot: Days Since LB2102 Infusion (0-400). Subjects grouped LCNEC and SCLC. Dose Levels 1-7. Overall Response: Partial response (PR), Stable disease (SD), Progressive disease (PD), Death, Subsequent cancer therapy.
Duration of Response (DOR): 185 days *; DOR: 208 days; DOR: 36+ days; DOR: 31+ days
- At median follow up 12.5 mo; median DOR was 6.5 mo (95% CI, 6.1-NR), ongoing response in 2 subjects
- At >=DL3 (median follow up 9.5 mo), median duration of disease control was 6.1 mo (95% CI, 1.3-6.8 mo)
Presented by Dr. Zhonglin Hao, ASCO 2026
Dr. @BZhangMD (@MDAndersonnews) frames alpha-emitter RLT as an emerging modality in SCLC. RYZ101 (225Ac-DOTATATE) is under first-line study in SSTR-expressing ES-SCLC; target expression heterogeneity and bone marrow toxicity are main considerations #DAVALung
NETTER-2
[Slide 1]
177Lu-PRRT now SoC in first line neuroendocrine tumors.
NETTER-2: phase 3 first line NET.
Screening phase: Patients >=15 years; N=226. Advanced, SSTR+, well-differentiated, G2 or G3 GEP-NET (Ki67 >=10% and <=55%). Diagnosis within last 6 months prior to enrollment. No prior PRRT or systemic therapy.
Randomized treatment phase R 2:1: 177Lu-DOTATATE 4 x 7.4 GBq + octreotide LAR (30 mg) Q8W; vs High dose octreotide LAR (60 mg) Q4W.
Optional treatment extension phase: Retreatment with 177Lu-DOTATATE (7.4 GBq/200mCi) Q8W x 2-4 cycles; Cross-over treatment 177Lu-DOTATATE (7.4 GBq/200mCi) Q8W x 4 cycles + octreotide LAR (30 mg).
Stratification factors: Grade (G2 vs G3); Tumor origin (pancreas vs other origin). Study endpoints: Primary: PFS; Key secondary: ORR, QOL.
PFS KM: 177Lu-DOTATATE arm vs High dose octreotide arm. PFS median, months (95% CI): 177Lu-DOTATATE n=151: 22.8 (19.4, NE); High dose octreotide n=75: 8.5 (7.7, 13.8). Stratified HR (95% CI): 0.276 (0.182, 0.418). p-value <0.0001.
Singh S et al, presented in 2024 ASCO GI Cancer Symposium; published Lancet 2024.
———
[Slide 2]
RZY101 (SSTR2 225Ac-Dotatate) in SCLC.
Mechanism: 1. RYZ101 binds to SSTR on the cell membrane. 2. RYZ101 and SSTR enter the cell by endocytosis. 3. Decay of 225Ac releases alpha-particles causing ds-DNA breaks leading to cell death. alpha-particle emission from 225Ac. RYZ101 (225Ac-DOTATATE).
SSTR PET Imaging: Tumor SUVmax 34.91; Normal liver SUVmean 5.56; Tumor SUVmax 7.52.
Presented by Aaron S. Mansfield et al, IASLC WCLC 2025.
———
[Slide 3]
RZY101 (225Ac-Dotatate) + EP+atezolizumab in 1st line SSTR-expressing SCLC.
Dose escalation (Standard 3+3 design, n=3-6 in each dose level; <=N=18 in total): Dose level 1 (n=4) RYZ101 6.5 MBq; Dose level 2 (n=5) RYZ101 8.3 MBq; Dose level 3 (n=6) RYZ101 10.2 MBq. 6-week DLT window. RYZ101 + SoC at RP2D.
Dose expansion N=37.
Induction phase: RYZ101 plus SoC (A + C + E): RYZ101 at escalating doses IV Q6W x 2 cycles; Atezolizumab 1200 mg IV on day 1 Q3W x 4 cycles; Carboplatin AUC 5-6 IV on day 1 Q3W x 4 cycles; Etoposide 80-100 mg/m2 IV on 3 consecutive days starting on day 1 Q3W x 4 cycles.
Maintenance phase: RYZ101 at dose level IV Q4W <=6 cycles total; Atezolizumab 1680 mg IV Q4W until disease progression.
Key eligibility criteria: Histologically or cytologically proven ES-SCLC; Untreated or <=1 cycle of SoC (platinum-etoposide with PD-L1 inhibitor); >=1 SSTR+ RECIST v1.1 measurable site of disease; >=50% of measurable lesions must be SSTR+ on regulatory agency-approved SSTR-PET; ECOG PS <=1; Adequate renal, hematologic, and hepatic function; Asymptomatic, adequately treated CNS metastases receiving stable or decreasing dose of steroids permitted.
Endpoints: Primary: RP2D, Safety, tolerability. Secondary: Efficacy, Pharmacokinetics.
Presented by Aaron S. Mansfield et al, IASLC WCLC 2025.
———
[Slide 4]
RZY101 (225Ac-Dotatate) +EP/IO in 1st line SCLC.
Patients | Value: Screened, N 51; Screen failure: negative SSTR-PET, n (%) 25 (49.0); Enrolled, N 16; Safety population, N 15. Main reason for screen failure was not meeting minimum SSTR positivity criterion. One enrolled patient did not receive RYZ101 because of adverse events associated with the first cycle of SoC.
Exposure (N=15) | Median (range): Total treatment duration, months 6.5 (1.4-11.9); No. of RYZ101 doses administered 3.0 (1.0-6.0); Total RYZ101 dose administered, MBq 25.1 (6.2-60.3). No. of SoC doses administered: Atezolizumab 6 (2-12); Carboplatin 4 (2-4); Etoposide 12 (6-12).
Treatment-emergent AEs (in >=20% of patients), All patients N=15, Grade 1/2 vs Grade 3/4: Fatigue, Neutrophil count decreased, Anemia, Nausea, Hypokalemia, Alopecia, White blood cell count decreased, Weight decreased, Vomiting, Urinary tract infection, Hypomagnesemia, Diarrhea, Constipation, Blood alkaline phosphatase decreased, Pyrexia, Platelet count decreased, Hyponatremia, Dysgeusia, Decreased appetite, Syncope, Pulmonary embolism, Pneumonia, Neutropenia, Lymphocyte count decreased, Hypotension, Hypertension, Dizziness, Dehydration, ALT increased, AST increased.
Presented by Aaron S. Mansfield et al, IASLC WCLC 2025.
Molecular profiling is redefining pulmonary LCNEC. Umit Tapan, MD (@The_BMC) reviews emerging genomic subtypes of pulmonary LCNEC, actionable alterations enriched in NSCLC-like disease (38% vs 9% in SCLC-like), and the potential role of NGS in guiding systemic therapy. #DAVALung
[Slide 1]
LCNEC Subgroup-Defining GA's Across Lung Cancer Types
Stacked bar chart - Submitted diagnosis (n), % from 0 to 100%. Categories: SCLC-like (pink); Unclassified (grey); NSCLC-like (blue); Carcinoid-like (yellow).
SCLC (4,688): 72% | 21% | 7%
LCNEC (1,426): 39% | 22% | 37%
LUSC (20,031): 9% | 38% | 53%
LUAD (62,541): 6% | 15% | 79%
Carcinoid Atypical (326): 3% | 66% | 14% | 16%
Carcinoid Typical (115): 70% | 8% | 23%
[Boston University / Boston Medical]
———
[Slide 2]
Actionable genomic alterations
NSCLC-like (n = 530) pie chart: No driver (330, 62%); KRAS other (106, 20%); KRAS G12C (49, 9.2%); KRAS G12D (19, 3.6%); (26, 4.9%); ALK fusion (5, 0.9%); RET fusion (5, 0.9%); BRAF V600E (1, 0.2%); MET exon14 (1, 0.2%); HER2 mut (1, 0.2%); EGFR driver (13, 2.5%).
SCLC-like (n = 557) pie chart: No driver (504, 91%); KRAS other (30, 5.4%); KRAS G12C (10, 1.8%); KRAS G12D (5, 0.9%); (8, 1.4%); HER2 mut (3, 0.5%); EGFR driver (5, 0.9%).
NSCLC-like: 38% potentially actionable GAs, majority KRAS (G12C most common), followed by EGFR, RET/ALK fusion, BRAF V600E, Met exon 14 and Her2
SCLC-like: 9% potentially actionable GAs, majority KRAS, followed by EGFR and Her2
———
[Slide 3]
Can NGS impact systemic treatment decisions?
- Improved outcomes with NSCLC type regimen (Gemcitabine/Taxane) in patients with RB1 wild type LCNEC (Derks JL et al. Clin Cancer Res. 2018)
- Limited data re: targeted treatment
- BRAF Non-V600 (+) (Chae YK et al., JCO Precis. Onc. 2018)
- ALK fusion (+) (Hayashi N et al., Internal Medicine 2018, Masuda K et al, Resp. Case Rep. 2021, Zheng Q et al, Onco Target Therapy 2018)
- EGFR (+) (Muto S et al., Case Rep Oncol.)
———
[Slide 4]
BACK TO OUR PATIENT
- 57 years old male, former tobacco use disorder (20 pack/year) -> right knee pain
- Work up: lytic distal femoral lesion, FDG avid lung mass & adrenal metastasis
- Soft tissue biopsy of the lytic lesion: high-grade neuroendocrine carcinoma
- TTF-1, synaptophysin, chromogranin (+), Ki-67 (70 %) -> favoring LCNEC
- NGS: KRAS amplification, STK11 deletion (exon 1), TP53 mutation
- TMB: 15 mut/mb. RB1 retained, no MEN1 alterations
- Carboplatin/paclitaxel/pembrolizumab -> 4 cycles -> maintenance pembrolizumab
- Consolidative RT to the lung primary and adrenal metastasis
- Disease free and off therapy, ~ 2 years after diagnosis
Biomarker spotlight Dr. @triparnasen from @OSUCCC_James discussed CD8/MHC-I as a potential marker of immunotherapy benefit in SCLC and its relevance for refining patient selection. #DAVALung
CASPIANIMpower133
[Slide 1]
Genome Profiles - Tumor Evolution
What defines sensitivity to first-line chemotherapy?
Genes: TP53, RB1, TP73, CREBBP/EP300, RGS7, COL22A1, FMN2, ASPM, CNTNAP2, KPHB1, MYC family gene amplification, KMT2D, NOTCH family gene mutations, PDE4DIP, KIAA1211, ploidy.
Cox regression (Backward Wald). Study cohort (n = 55 of 65). p53 missense vs Other TP53 gene-damaging: *P = 0.0026. p53 point mutations: CREBBP/EP300 TP73/FMN2 vs Other TP53 gene-damaging: *P < 0.001.
TP53 and RB1 part of the common ancestor C0.
- TP53-damaging alterations associate with resistance to chemotherapy
- in patients with TP53 point mutations: co-alterations of TP73, CREBBP/EP300 or FMN2 compromise efficacy of chemotherapy
George et al., Nature, 2024
———
[Slide 2]
Immunotherapy can work
IMpower133, CASPIAN, etc
...but usually doesn't
Median 10.5 vs. 12.9 mo
3-year survival 5.8 vs. 17.6%
OS KM curve: Durvalumab + EP vs EP; Time from randomization (months).
Paz-Ares et al., ESMO Open 2022
———
[Slide 3]
Epigenetic modifiers predicts outcome to immunotherapy
LSD1 as a single-gene determinant of outcome: Nivolumab OS by strata (Low/Mid/High) p = 0.005; Nivolumab + Ipilimumab p = 0.02.
EZH1/2 as a single-gene determinant of outcome: Nivolumab OS p = 0.076; Nivolumab + Ipilimumab p = 0.27.
KM curves with number at risk tables by strata (Low/Mid/High).
———
[Slide 4]
Conclusions and Future Directions
- Immunotherapy is now standard of care, but benefit is modest
- Baseline tumor genomics shape chemotherapy sensitivity
- TP53 and RB1 loss are founding events, and co-alterations in TP73, CREBBP/EP300, or FMN2 compromise chemotherapy efficacy
- Antigen presentation and epigenetic state drive IO response
- CD8/MHC-I status and single genes such as LSD1 and EZH1/2 predict immunotherapy outcome, and targeting these epigenetic modifiers can restore antigen presentation
- Transcriptional subtypes and plasticity reveal resistance biology
- Plasticity contributes to treatment resistance and complicates biomarker-driven strategies. Can targeting subtype plasticity provide previously unknown therapeutic opportunities?
- Liquid biopsy platforms show promise for identifying predictive and prognostic markers.
- Can cfDNA capture subtype heterogeneity and switching over time? If so, is it clinically actionable - and when should we test? The optimal timing and method for NE subtype assessment remain unclear.
Can treatment strategies for SCLC inform the management of extrapulmonary neuroendocrine carcinoma? Jeff Petty, MD (@AtriumHealth) reviews the ongoing SWOG S2012 trial, comparable DLL3 expression to SCLC, limited second-line outcomes (median OS 6.2 months), and the rationale for
IMpower133SWOG S2012
[Slide 1]
Extrapulmonary small cell carcinoma
SWOG S2012: Randomized phase II/III trial of first line platinum (P)/etoposide (E) with or without atezolizumab (NSC #783608) in patients with advanced or metastatic poorly differentiated extrapulmonary neuroendocrine carcinomas (NEC).
"With 189 pts (168 eligible), the study has 84% power to detect an improvement in 12-months OS from 35% to 57.5% (HR 0.53). This study was activated December 2021 with 3 pts enrolled over 1 year due to restricting NEC of small cell histology only. The protocol was amended in January 2023 to broaden eligibility to all NEC subtypes (small cell, large cell, and undefined histology with Ki-67 >=55%). As of January 2024, 35 patients have been enrolled. A protocol amendment is planned to remove the need for Ki-67 index for NEC of genitourinary origin to improve accrual."
Annotation: HR for OS in IMpower133 was 0.76.
ASCO 2024. J Clin Oncol 42, TPS4201 (2024).
———
[Slide 2]
DLL3 in extrapulmonary small cell (DLL3 expression by IRS score, % of cases, Pulmonary vs GEP-NEC)
G - small cell NEC: DLL3 negative (IRS0-1) Pulmonary 16.5% / GEP-NEC 33.3%; DLL3 weak (IRS2-3) 6.6% / 4.8%; DLL3 moderate (IRS4-8) 18.7% / 9.5%; DLL3 strong (IRS9-12) 58.2% / 52.4%; p = 0.32.
H - large cell NEC: DLL3 negative (IRS0-1) 24.2% / 49.3%; DLL3 weak (IRS2-3) 9.7% / 4.3%; DLL3 moderate (IRS4-8) 12.9% / 17.4%; DLL3 strong (IRS9-12) 53.2% / 29.0%; p = 0.007.
J - DLL3 expression in pulmonary TC/AC (TC vs AC): DLL3 negative (IRS0-1) 61.5% / 51.3%; DLL3 weak (IRS2-3) 6.3% / 7.7%; DLL3 moderate (IRS4-8) 13.5% / 10.3%; DLL3 strong (IRS9-12) 18.8% / 30.8%; p = 0.45.
Endocrine Pathology (2025) 36:9.
———
[Slide 3]
Case for tarlatamab for extrapulmonary small cell
Left KM curve: EPNEC Second Line Median OS = 6.2 mo (irinotecan, paclitaxel, paclitaxel + topotecan, temozolomide, topotecan). Surviving over Months Since Initiating 2nd-line Therapy.
Right KM curve (Percentage of Patients over Months since Randomization): Tarlatamab vs Chemotherapy. Median Overall Survival (95% CI), mo: Tarlatamab (N=254) 13.6 (11.1-NR); Chemotherapy (N=255) 8.3 (7.0-10.2). Stratified hazard ratio for death, 0.60 (95% CI, 0.47-0.77); P<0.001. No. at Risk: Tarlatamab 254, 220, 192, 131, 60, 17, 0; Chemotherapy 255, 210, 156, 97, 42, 9, 2, 0.
- Extrapulmonary small cell expresses DLL3 at similar rate to SCLC
- Current second line treatments are ineffective
- Data collection is ongoing through NPP through Amgen single patient IND program
- 120 pts approved but only 67 received treatment as many died during application process
- Prospective trials are ongoing
New England Journal of Medicine, Volume 393 - Number 4 - July 24, 2025, Pages 349-361.
———
[Slide 4]
Lessons from SCLC genetics
Oncoprint (B) - Ancestry (EUR/AFR/AMR/EAS/SAS), TMB level (Low <10 mut/Mb / High >=10 mut/Mb), MSI status (MSS / MSI ambiguous / MSI-H / Undetermined). Gene alteration frequencies:
- TP53: 91.6%
- RB1: 73.5%
- KMT2D: 12.9%
- PTEN: 9.9%
- MYCL: 7.2%
- CREBBP: 6.1%
- MYC: 6.0%
- NOTCH1: 5.6%
- PIK3CA: 5.6%
- RICTOR: 5.0%
- CCNE1: 4.9%
- FGF10: 4.3%
- CDKN2A: 4.1%
- FGFR1: 3.9%
- EGFR: 3.4% (highlighted)
- SOX2
- KRAS: 3.3%
- NF1: 3.3%
- ZNF703: 2.9%
Legend: Amplification; Deletion; Truncation; Fusion/rearrangement; Amplification & point mutation/indel; Deletion & truncation; Point mutation/indel; Other multiple.
From retrospective datasets to prospective platform trials, Jay Lee @UCLAHealth outlines the evolving perioperative landscape for high-grade neuroendocrine carcinoma- integrating surgery, immunotherapy, safety, and biomarker discovery to inform future clinical research. #DAVALung
ADRIATIC
[Slide 1]
ADRIATIC safety population: high AE, pneumonitis, and drug-modification burden
cCRT + durvalumab consolidation (N=262) vs cCRT + placebo (N=265). Values are patients, n (%).
Any immune-mediated AE 32.1% vs 10.2%; Pneumonitis/radiation pneumonitis 38.2% vs 30.2%; Drug discontinuation 8.8% vs 3.0%. Diff shown = Durva - placebo.
Columns: Event | cCRT + durvalumab Any grade | cCRT + durvalumab Grade 3/4 | cCRT + placebo Any grade | cCRT + placebo Grade 3/4 | Absolute diff (any grade)
Global safety events:
Any adverse event of any cause: 247 (94.3) | 64 (24.4) | 234 (88.3) | 64 (24.2) | +6.0 pp
Any serious adverse event, including events with outcome of death: 78 (29.8) | - | 64 (24.2) | - | +5.6 pp
Any adverse event with outcome of death: 7 (2.7) | - | 5 (1.9) | - | +0.8 pp
Any event leading to discontinuation of durvalumab or placebo: 43 (16.4) | - | 28 (10.6) | - | +5.8 pp
Any event leading to dose interruption: 91 (34.7) | - | 76 (28.7) | - | +6.0 pp
Any immune-mediated adverse event: 84 (32.1) | 14 (5.3) | 27 (10.2) | 4 (1.5) | +21.9 pp
Pulmonary events of interest:
Radiation pneumonitis: 60 (22.9) | 3 (1.1) | 62 (23.4) | 5 (1.9) | -0.5 pp
Pneumonitis: 28 (10.7) | 3 (1.1) | 16 (6.0) | 2 (0.8) | +4.7 pp
Pneumonitis or radiation pneumonitis: 100 (38.2) | 8 (3.1) | 80 (30.2) | 7 (2.6) | +8.0 pp
Pneumonitis or radiation pneumonitis leading to discontinuation of durvalumab or placebo: 23 (8.8) | - | 8 (3.0) | - | +5.8 pp
References: Cheng Y et al, N Engl J Med. 2024;391(14):1313-1327. doi:10.1056/NEJMoa2404873; Iyengar P et al, ASTRO 2024 Annual Meeting, LBA13.
Presenter: Jay M. Lee, M.D.
———
[Slide 2]
SEER: Overall survival after propensity matching: surgery vs chemoradiotherapy
Stage T1-2N0M0 SCLC | SEER 2000-2020 | PSM cohort: 151 surgery vs 151 concurrent chemoradiotherapy
A (KM curve): Overall survival vs Months (0-132). Surgery vs CXRT. Median: 29 vs 61 months; HR = 0.59, 95% CI 0.45-0.78; P < 0.001. Number at risk: surgery 151...; chemoradiotherapy 151...
B (Forest plot, Hazard ratio): Age 1.03 (1.02, 1.05) <0.001; Sex: female Reference, male 1.00 (0.75, 1.34) 0.982; Race: white Reference, black 0.74 (0.36, 1.54) 0.424, others 2.24 (0.90, 5.55) 0.081; Site: upper lobe Reference, middle lobe 1.15 (0.65, 2.04) 0.629, lower lobe 0.83 (0.59, 1.15) 0.262, others 1.08 (0.56, 2.09) 0.823; Laterality: left Reference, right 0.96 (0.71, 1.27) 0.714; Grade: III/IV Reference, I/II unknown 0.86 (0.66, 1.14) 0.291; T stage: T1N0M0 Reference, T2N0M0 1.10 (0.83, 1.47) 0.511; Treatment: chemoradiotherapy Reference, surgery 0.60 (0.45, 0.80) <0.001.
Median OS: 61 vs 29 mo (Surgery vs chemoradiotherapy)
5-year OS: 50.1% vs 33.8% (Surgery vs chemoradiotherapy)
Multivariable OS HR: 0.60 (0.45-0.80) Mortality HR for surgery; P<0.001
Interpretation boundary: Retrospective SEER. No immunotherapy; residual confounding possible.
Zhou L, Wang S-F, Ma C-X, Huang W, Pan X-B. Journal of Cardiothoracic Surgery. 2026;21:226. doi:10.1186/s13019-026-03995-0.
Presenter: Jay M. Lee, M.D.
———
[Slide 3]
NCDB: Underutilization of Surgery in Stage I SCLC
NCDB 2004-2018: guideline-recommended surgery increased over time, but most stage I patients were still treated without surgery.
Cohort derivation and treatment allocation: All SCLC in NCDB 2004-2018 N = 296,583; Analytic restrictions (Stage I disease, Complete staging, Non-palliative surgery); Stage I SCLC identified N = 13,279 = 4.5% of all SCLC; Treatment-classified stage I cohort N = 13,003; Surgical resection N = 3,823 (29.4%); No surgery N = 9,180 (70.6%). Even after restricting to stage I disease, surgery was received by only ~3 in 10 patients.
Annual receipt of surgery among stage I SCLC patients (bar chart 2004-2017, Patients n and Surgery rate %): No surgery (blue) vs Surgery (orange).
Surgery increased from 15.6% in 2004 to 39.6% in 2017, but remained the minority treatment.
Source: Fong AJ et al. Disparities and Underutilization of Surgery for Early Stage Small Cell Lung Cancer. Ann Thorac Surg. 2024;117:1095-1102. doi:10.1016/j.athoracsur.2024.01.012.
Presenter: Jay M. Lee, MD
———
[Slide 4]
Perioperative IO in High-Grade Neuroendocrine Carcinoma
Jay M. Lee, MD, Thoracic Surgery | UCLA. Concept design | March 27, 2025
Pathway to escalation/combination treatment strategies and HG NEC/SCLC subtyping and biomarker discovery (window of opportunity)
Phase 2 platform trial. Population: Stage I-III (LS) SCLC or high-grade NEC - Small cell lung carcinoma; Mixed small and large cell high-grade neuroendocrine carcinoma; Large cell carcinoma; Highly proliferative (G3) carcinoid tumors; +/- intermediate-grade neuroendocrine carcinoma.
Part 1: initial safety and feasibility. NEOADJUVANT -> RESECTION -> ADJUVANT.
Arm 1: CT-ICI + DLL3-TCE x 4 cycles -> Surgery -> ICI + DLL3-TCE until PD +
Arm 2: CT-ICI x 4 cycles -> Surgery -> ICI until PD
Arm 3: ICI + DLL3-TCE + novel agent -> Surgery -> +/- CT, then ICI + DLL3-TCE + novel agent until PD ++
+ Adjuvant regimen may be ICI + DLL3-TCE. ++ Adjuvant CT may precede ICI + DLL3-TCE + novel agent.
PRIMARY: pCR, Safety. SECONDARY: MPR, ORR. EXPLORATORY: ctDNA clearance, EFS, biomarker studies.
Presenter: Jay M. Lee, MD
The CROWN 7-year update: lorlatinib achieved 55% 7-year PFS and 92% 7-year intracranial time-to-progression in ALK+ NSCLC, with no new safety signals. @MNagasaka (@UCIrvineHealth) reviews the data. #DAVALung
[Slide 1]
PFS in the ITT Population (5-Year follow up) [CROWN, ASCO 2026]
PFS KM - Lorlatinib (n=149) vs Crizotinib (n=147); Events n: 55 vs 115; PFS median (95% CI) months: (64.3-NR) vs 9.1 (7.4-10.9); HR (95% CI) 0.19 (0.13-0.27). Lorlatinib PFS landmarks approximately: 70% (~12 mo), 65%, 62%, 60% (~60 mo); Crizotinib approximately 19%, 10%, 10%, 8%.
Tony S. K. Mok et al, ASCO 2026.
———
[Slide 2]
Time to IC (intracranial) Progression in the ITT Population [CROWN]
KM curve - Lorlatinib essentially flat near 90%+ (approximately 92% landmark, boxed) vs Crizotinib declining. Lorlatinib time to IC progression not reached. No new IC progression events occurred after the first 16 months on lorlatinib. (Numeric detail in table largely illegible.)
———
[Slide 3]
CROWN: A Randomized, Global, Ph3 Study
Key eligibility criteria: Stage IIIB/IV ALK+ NSCLC; No prior systemic treatment for metastatic disease; ECOG PS 0-2; Asymptomatic treated or untreated CNS metastases were permitted; >=1 extracranial measurable target lesion (RECIST 1.1) with no prior radiation required.
Randomized 1:1, N=296. Lorlatinib 100 mg once daily n=149; Crizotinib 250 mg twice daily n=147. Stratified by: Presence of brain metastases (yes vs no); Ethnicity (Asian vs non-Asian). No crossover between treatment arms.
Primary endpoint: PFS by BICR. Key secondary endpoint: OS. Other secondary endpoints: PFS by investigator; ORR by BICR and investigator; IC ORR, IC TTP, IC DOR, TTR and IC TTR by BICR and investigator; Safety; Quality of life; Biomarker analyses.
In this post hoc analysis with 7 years of follow-up, investigator-assessed efficacy outcomes, safety, and biomarker analyses (data cutoff: October 31, 2025) were presented. At data cutoff, the required number of OS events for a protocol-specified second interim analysis (at least 139 deaths) has not been reached; 123 of 296 (42%) discontinued the study in both arms due to death.
Tony S. K. Mok et al, ASCO 2026.
———
[Slide 4]
Adverse Events [CROWN, ASCO 2026]
- No increase in frequency of grade 3 or 4 AEs since the 5-year analysis (77%). Majority were due to an increase in lipid values.
- Despite higher rates of hyperlipidemia with lorlatinib, no increase in cardiovascular AEs was observed compared with crizotinib.
- Frequency of CNS AEs was consistent with longer follow-up; most were grade 1 or 2.
- Dose reductions were reported in 34% of patients in the lorlatinib group; median time to dose reduction was 25 weeks.
- All treatment-related discontinuations (5%) occurred within the first 26 months.
AEs of special interest - Lorlatinib vs Crizotinib:
Edema 58% vs 43%; Hypertriglyceridemia 71% vs 6%; Hypercholesterolemia 73% vs 4%; Peripheral neuropathy 46% vs 16%; Weight gain 45% vs 13%; Cognitive effects 30% vs 7%; Mood effects 21% vs 7%; Psychotic effects 5% vs 1%; Speech effects 6% vs 0%.
Safety profile of lorlatinib was consistent with prior analyses with no new safety signals with longer follow-up.
Tony S. K. Mok et al, ASCO 2026.
MTAP-deleted NSCLC at #DAVALung: Dr. @matt_cw_lee@cityofhope presented AMG 193/anvumetostat, a CNS-penetrant MTA-cooperative PRMT5 inhibitor. Phase I: ORR 21.4%; NSCLC had 2 PR, 3 uPR, 6 SD. AMG 193 development was discontinued; other PRMT5/MAT2A inhibitors remain in trials.
[Slide 1]
Other PRMT5 and MAT2A inhibitors still in development
Drugs | MOA | Trials | Preliminary Outcomes
BMS-986504 | MTA cooperative PRMT5 inhibitor | NCT05245500 | ORR 29.0% (NSCLC), ORR 57% (EGFR), ORR 50% (ALK)
CTS3497 | MTA cooperative PRMT5 inhibitor | NCT06971523 | ORR 60% (NSCLC)
HSK41959 | MTA cooperative PRMT5 inhibitor | NCT06968572 | ORR 27.3%
Vopimetostat (TNG462) | MTA cooperative PRMT5 inhibitor | NCT05732831 | ORR 27.0%
IDE397 (IDEAYA) | MAT2A competitive inhibitor | NCT04794699 | ORR (22% adeno, 38% SCC)
———
[Slide 2]
Anvumetostat (AMG 193) discontinued in development
• 3/1/26 Amgen revealed that it has ended development on anvumetostat (AM193) and Amgen has stopped four phase 1b or phase 2 trials of anvumetostat after “the overall efficacy observed did not meet our high bar for additional internal investment”
• Similarly, my patient has also stopped anvumetostat (AMG 193) and is on another clinical trial
———
[Slide 3]
Efficacy of AMG 193
AMG 193 (N = 60). Top: Treatment duration (weeks) swimmer plot with Status legend (AE-related discontinuation, Patient withdrew, Clinical PD, Death). Bottom: Waterfall of Tumor size change (%) with Pre-assessment, PR (green), SD (blue), PD (red), NE. Tumor types include Esophageal, ACC, SCLC, PDAC, Sarcoma, GBM, MESO, NSCLC, Melanoma, Endometrial, CRC, CCA, RCC, GIST, Bladder, Gallbladder, etc. Doses 40–1200 mg o.d./b.i.d.
• ORR 21.4% with responses observed overall
– NSCLC: 2 PR, 3 unconfirmed PRs, 6 SD
• Median duration of response was 8.3 months (95% CI, 2.7-NE)
• Responses reportedly occurred at 8 or 16 weeks
J Rodon ESMO 2024
———
[Slide 4]
Anvumetostat (AMG 193): Safety Profile
Adverse Events in Dose Exploration and Expansion (N = 167): Treatment-emergent / Treatment-related; Nausea, Vomiting, Fatigue, Decreased appetite, Dizziness, Constipation, Anaemia, Diarrhoea, Headache, Abdominal pain, Asthenia, Dysgeusia, Weight decreased, Blood bilirubin increased, Dyspnoea, Confusional state, Pyrexia, COVID-19, Cough, Hypoalbuminaemia. Grade 3&4 vs Grade 1&2.
Related Events in Dose Expansion with 1200 mg QD (N = 87):
TRAE | Any grade | Grade 3
All Events 83.9% | 18.4%
Nausea 57.5% | 4.6%
Vomiting 34.5% | 3.4%
Fatigue 25.3% | 1.1%
Dizziness 21.8% | 1.1%
Decreased appetite 20.7% | 0%
Diarrhea 13.8% | 0%
Dysgeusia 5.7% | 0%
Asthenia 4.6% | 1.1%
Headache 4.6% | 0%
Anemia 4.6% | 0%
Balance disorder 4.6% | 0%
Constipation 4.6% | 0%
Disturbance in attention 4.6% | 0%
Blood bilirubin↑ 3.4% | 0%
Malaise 3.4% | 0%
• AMG 193 most common TRAEs were mainly nausea, vomiting and fatigue with 85% reporting any grade TRAEs, ≥G3 13.8%
• 27.5% treatment interruption and 2.5% discontinuation
J Rodon ESMO 2024
ALK Positive is at the 5th Summit on Thoracic Malignancies
Our Executive & Medical Director, Dr. Ken Culver, is attending this invitation-only DAVA Oncology meeting alongside leading thoracic oncology experts advancing research and precision medicine.
#ALKpositive
Treatment beyond progression in NRG1+ NSCLC: Dr. Zhaohui (Ann) Liao Arter (@UCIrvineHealth) presented zenocutuzumab data in 27 pts—81% had oligoprogression, 22% received adjunct local therapy, 30% stayed on >6m beyond PD, with no AE-related discontinuations. #DAVALung
[Slide 1]
Case studies: Selected patients continuing >9 months beyond PD
Case 1: 64-year-old male with NRG1+ NSCLC. Stage at diagnosis: IV. Fusion: CD74-NRG1. Metastatic sites at baseline: bone, liver, lung, lymph nodes, visceral. Baseline genetics: HER2 unknown, HER3 unknown, KRAS wild type. Prior treatment history: No prior systemic therapy. Zenocutuzumab (pre-progression) best overall response: PR (Cycles 3-37). Zenocutuzumab beyond progression rationale: Asymptomatic oligoprogressive disease and continued clinical benefit; duration beyond progression 0.8 years (total zenocutuzumab exposure >3.5 years (44.65 months)).
Case 2: 75-year-old female with NRG1+ NSCLC. Stage at diagnosis: IB. Fusion: CD74-NRG1. Metastatic sites at baseline: lung, lymph nodes, visceral. Baseline genetics: HER2 unknown, HER3 unknown. Prior treatment history (Jan 2015 to Aug 2022): Jan 2015 Lobectomy; Metastatic setting May 2022 to Jul 2022: Carboplatin + paclitaxel with radiation. Zenocutuzumab (pre-progression) BOR: PR (Cycles 5-11). Beyond progression: Minimal and asymptomatic tumor growth; duration beyond progression >2.3 years (to Dec 2025, ongoing; total exposure ~3.2 years (38 months)).
Case 3: 63-year-old female with NRG1+ NSCLC. Stage at diagnosis: IV. Fusion: CD74-NRG1. Metastatic sites at baseline: lung, visceral. Baseline genetics: HER2 unknown, HER3 unknown, EGFR/ALK/ROS1 negative, PD-L1 <1%. Prior treatment: adjuvant no prior systemic; Metastatic May 2022 to Jun 2022: Cisplatin + pembrolizumab + pemetrexed. Zenocutuzumab BOR: SD (Cycles 3-5). Beyond progression: Stable symptoms and ECOG PS 1; imaging showed waxing and waning disease; treatment well tolerated; duration beyond progression ~1 year (total exposure ~1.4 years (17.1 months)).
———
[Slide 2]
Zenocutuzumab Safety Profile in Patients Treated beyond PD in NRG1+ NSCLC
Adverse events, n (%) N=27, All grades / Grade 3-4: Patients with >=1 TRAE 21 (78) / 1 (4); TRAEs in >=10% of patients: Diarrhea 9 (33) / 0 (0); Paronychia 3 (11) / 0 (0); Anemia 1 (4) / 1 (4); Patients with >=1 serious TRAE 0 (0) / 0 (0); TEAE leading to discontinuation 0 (0) / 0 (0).
Data cutoff date: August 4, 2025. N=27. Treatment-related anemia occurred in <10% of patients; however, it is included as this event was Grade >=3. Arter ZL et al. Presented at IASLC 2026 Targeted Therapies of Lung Cancer (TTLC) Meeting; February 18-21, 2026; Huntington Beach, CA, USA.
———
[Slide 3]
Zenocutuzumab Exposure and Treatment Beyond PD in NRG1+ NSCLC
Duration of zenocutuzumab exposure, months, median (range): Total 9.9 (3.3-44.7); Before PD 7.3 (0.5-36.8); Beyond PD 3.1 (1.3-23.2). TTR months median (range): 1.8 (1.7-9.2). DOR months median (range): 7.4 (3.6-35.1). Patients with treatment ongoing: 4 (15%). Best overall response: PR (n=14), SD (n=10), PR (n=3).
Progression characteristics on zenocutuzumab, N=27: Oligoprogression 22 (81); 1 lesion 14 (52); 2 lesions 6 (22); 3 lesions 2 (7); Diffuse progression 5 (19); 3 lesions 1 (4); 4 lesions 4 (15); Progression including brain metastases 5 (19).
Treatment beyond PD, N=27: Local therapy adjunct to zenocutuzumab beyond PD 6 (22); Gamma knife surgery 2 (7); Radiotherapy 3 (11); Surgical resection 2 (7); Zenocutuzumab >6 months beyond PD 8 (30); 6-9 months 4 (15); >9-23 months 3 (11); >23 months (ongoing) 1 (4).
Data cutoff date: August 4, 2025. Arter ZL et al. Presented at IASLC 2026 TTLC Meeting.
———
[Slide 4]
Zenocutuzumab Median PFS in NRG1+ NSCLC
Median PFS, months, median (95% CI): Treatment naive (n=20): 7.5 (3.9-13.2); Previously treated (n=121): 6.8 (5.5-7.4).
Data cutoff date: August 4, 2025. Primary efficacy set. Liu SV et al. Presented at IASLC-ASCO North America Conference on Lung Cancer; December 5-7, 2025; Chicago, IL, USA.
At #DAVALung, Dr. @ElaineShumMD@nyulangone presented zidesamtinib/NVL-520, an investigational ROS1 TKI designed for CNS activity, avoidance of TRK inhibition, and G2032R resistance mutation. ARROS-1: pretreated ORR 44%, DOR ≥12m 78%; dose reduction 10%, discontinuation 2%.
ARROS-1
[Slide 1]
CNS activity [ARROS-1 / taletrectinib comparator context; ROS1+ NSCLC]
Measurable CNS lesions by BICR at baseline. Advanced ROS1+ NSCLC, Analysis by BICR:
Any prior ROS1 TKI +/- chemotherapy | Prior crizotinib only +/- chemotherapy
IC-ORR, % (n/N) [95% CI]: 48% (27/56)(a) [35, 62] | 85% (11/13) [55, 98]
IC-CR, % (n/N): 20% (11/56) | 54% (7/13)
% IC-DOR >= 6 months [95% CI]: 79% [56, 91] | 91%(c) [51, 99]
% IC-DOR >= 12 months [95% CI]: 71% [46, 87] | 91%(c) [51, 99]
- CNS responses also observed in patients who had received >=1 prior brain-penetrant TKI, including prior entrectinib, lorlatinib, repotrectinib, or taletrectinib: IC-ORR: 37% (16/43)(a); [95% CI 23, 53]), including 4 IC-CRs
- No CNS progression among patients who entered the study without brain metastases at baseline per BICR
(a) Includes 2 unconfirmed intracranial partial responses (PR). (b) Analyses of DOR based on Kaplan-Meier estimates. (c) One CNS progression event among CNS responders (n=11).
Taletrectinib-refractory patient with CD74-ROS1 NSCLC and G2032R mutation - CR maintained throughout treatment course, DOR 11+ months. [Baseline vs 3 months MRI]
Drilon A. WCLC 2025.; Liu G. AACR 2026.
———
[Slide 2]
Duration of Response and Progression-Free Survival [Advanced ROS1+ NSCLC, Kaplan-Meier Estimate]
Duration of Response - Any prior ROS1 TKIs (range 1-4) +/- chemo(a) | 1 prior ROS1 TKI (crizotinib or entrectinib) +/- chemo(b):
% >= 6 months [95% CI]: 84% [71, 92] | 93% [74, 98]
% >= 12 months [95% CI]: 78% [62, 88] | 93% [74, 98]
% >= 18 months [95% CI]: 62% [28, 84] | 93% [74, 98]
Progression-Free Survival - Any prior ROS1 TKIs | 1 prior ROS1 TKI:
% >= 6 months: 57% [47, 66] | 70% [56, 81]
% >= 12 months: 48% [38, 57] | 68% [53, 79]
% >= 18 months: 40% [24, 55] | 68% [53, 79]
Data cut-off: March 21, 2025. (a) Any prior ROS1 TKI: Emerging median DOR of 22 months (95% CI: 17, NE) continues to mature. Median PFS was 9.7 [5.5, NE] months with median follow-up of 11.1 months (range 0.2-25.6). (b) 1 prior ROS1 TKI (crizotinib [C] or entrectinib [E]): Emerging median DOR of 22 months (95% CI: 22, NE) and median PFS of 23.8 months (95% CI: 23.8, NE) continue to mature, median follow-up 11.8 months (range 1.2-25.6).
- In patients that received prior crizotinib only, there were no progression events among responders (DOR range: 7.3+ to 23.2+ months). PFS rate was 89% (95% CI: 70, 96) at 6, 12, and 18 months with median not reached.
- In patients that received >=2 prior ROS1 TKIs +/- chemotherapy, DOR rate was 71% (95% CI: 46, 86) at 6 months and 56% (95% CI: 29, 76) at 12 months.
Drilon A. WCLC 2025.
———
[Slide 3]
Objective Response in ROS1 TKI Pre-treated Patients [Advanced ROS1+ NSCLC, RECIST 1.1 by BICR]
Any prior ROS1 TKI (range 1-4) +/- chemotherapy | 1 prior ROS1 TKI (crizotinib or entrectinib) +/- chemotherapy:
ORR, % (n/N) [95% CI]: 44% (51/117) [34, 53] | 51% (28/55)(a) [37, 65]
CR, % (n/N): 1% (1/117) | 2% (1/55)
(a) Prior crizotinib only +/- chemotherapy: ORR = 68% (19/28). Prior entrectinib only +/- chemotherapy: ORR = 33% (9/27).
Responses were also observed in patients previously treated with:
- >=2 prior ROS1 TKIs +/- chemotherapy: ORR = 38% (22/58; 95% CI: 26, 52)
- Prior repotrectinib: ORR = 47% (8/17), DOR range 3.5 to 17.2 months
- Prior taletrectinib: ORR = 43% (3/7), DOR range 5.2 to 7.0+ months
[Waterfall plot: 1 Prior ROS1 TKI (crizotinib or entrectinib) +/- chemotherapy; Prior crizotinib, Prior entrectinib, + Prior chemotherapy]
Data cut-off: March 21, 2025.
Drilon A. WCLC 2025.
———
[Slide 4]
Zidesamtinib (NVL-520)
- An investigational ROS1 tyrosine kinase inhibitor.
- Drug design goals: Activity against resistance mutations; CNS activity; Avoid TRK inhibition.
[Structural model: ROS1 G2032R, Zidesamtinib, G2032R]
NYU Langone Health
Exploring in the next session: The science behind precision oncology at #DAVALung. Moderator Ravi Salgia leads a panel on how genomics, epigenomics, proteomics, and metabolomics are uncovering new biomarkers and informing more personalized treatment strategies.
At #DAVALung, Dr. @MNagasaka@UCIrvineHealth presented Taletrectinib TRUST-I/II pooled data: TKI-naïve cORR89.8%, DOR 49.7m, PFS 46.1m; TKI-pretreated cORR55.8%, DOR 16.6m, PFS 9.7m. No new safety signals with longer follow-up.
TRUST-ITRUST-II
[Slide 1]
Integrated safety analysis (N=363)
Most frequent TEAEs (>=20% of patients), n (%): Any grade / Grade 1 / Grade 2 / Grade >=3
AST increased: 261 (71.9) / 166 (45.7) / 65 (17.9) / 30 (8.3)
ALT increased: 248 (68.3) / 143 (39.4) / 65 (17.9) / 40 (11.0)
Diarrhea: 234 (64.5) / 181 (49.9) / 44 (12.1) / 9 (2.5)
Nausea: 174 (47.9) / 131 (36.1) / 38 (10.5) / 5 (1.4)
Vomiting: 164 (45.2) / 127 (35.0) / 32 (8.8) / 5 (1.4)
Anemia: 139 (38.3) / 80 (22.0) / 44 (12.1) / 15 (4.1)
Dizziness: 78 (21.5) / 67 (18.5) / 10 (2.8) / 1 (0.3)
Electrocardiogram QT prolonged: 76 (20.9) / 52 (14.3) / 11 (3.0) / 13 (3.6)
Constipation: 74 (20.4) / 62 (17.1) / 12 (3.3) / 0
Blood creatinine increased: 73 (20.1) / 62 (17.1) / 11 (3.0) / 0
- With longer follow-up, no new safety signals were identified, and safety was consistent between the integrated safety population and TKI-naive patients
- Most common (any grade) TEAEs were increased AST, increased ALT, diarrhea, nausea, and vomiting
- Rates of neurologic TEAEs were low and mostly Grade 1 or 2: Dizziness 18.5% Grade 1; 2.8% Grade 2. Dysgeusia: 13.2% Grade 1; 2.2% Grade 2
- TEAEs led to dose interruptions in 42.7% of patients, dose reductions in 31.3%, and treatment discontinuations in 8.5%
Bazhenova L, Nieva J, Nagasaka M, et al, AACR 2026.
———
[Slide 2]
DOR in TKI pretreated
Pooled (N=113). Median follow-up: 35.8 months.
Median DOR: 16.6 months (95% CI: 10.7-24.9).
Events: 39/63 (61.9%).
No. at risk: 63, 57, 50, 37, 31, 22, 17, 12, 6, 0 (0-48 months).
Liu G, Nieva J, Bazhenova L, et al, AACR 2026 (poster).
———
[Slide 3]
Tumor Response in TKI-Naive Patients
Best Change in Sum of Diameters from Baseline (%). Pooled Efficacy Population (N=157). cCR, cPR, SD, PD; Brain metastasis marked.
Efficacy: TRUST-I (n=103) | TRUST-II (n=54) | Pooled (N=157)
cORR, % (95% CI): 90.3 (82.9-95.3) | 88.9 (77.4-95.8) | 89.8 (84.0-94.1)
Prior chemotherapy: (n=20) 85.0 (62.1-96.8) | (n=10) 100 (69.2-100) | (n=30) 90.0 (73.5-97.9)
IC Efficacy: (n=8) | (n=9) | (n=17)
IC-cORR, % (95% CI): 87.5 (47.4-99.7) | 66.7 (29.9-92.5) | 76.5 (50.1-93.2)
Data cutoff: August 31, 2025
———
[Slide 4]
TRUST-I and TRUST-II
Key Eligibility Criteria: Locally advanced or metastatic NSCLC with ROS1 fusion; Age >=18 years; ECOG PS 0-1; Brain metastases were allowed if stable.
TRUST-I China Phase 2 Study (NCT04395677): Cohort 1 TKI-naive; Cohort 2 TKI-pretreated.
TRUST-II Global Phase 2 Study (NCT04919811): Cohort 1 TKI-naive; Cohort 2 TKI-pretreated.
Taletrectinib 600 mg QD.
Endpoints - Primary: IRC-assessed cORR per RECIST v1.1. Key Secondary: DOR, PFS, OS, IC-ORR, Safety.
- The efficacy population reported here included TKI-naive patients from TRUST-I and TRUST-II with >=1 measurable baseline lesion per RECIST v1.1 by IRC who started treatment on taletrectinib 600 mg QD
- Safety was evaluated in TKI-naive and TKI-pretreated patients with ROS1+ NSCLC from Phase 1 and Phase 2 trials who received >=1 dose of taletrectinib 600 mg QD
Perol M, et al. J Clin Oncol 2025;43:1920-1929. Bazhenova L, Nieva J, Nagasaka M, et al, AACR 2026.
Neoadjuvant ALK TKIs are moving earlier: NAUTIKA1/ALNEO reported MPR 61%/42%, pCR 25%/12%, and LORIN saw 79% proceed to resection or CRT after lorlatinib. Jay M. Lee, MD (@UCLAHealth) reviews perioperative ALK care. #DAVALung
ALKOVE-1 enrolled 394 pts in 10 months (39.4 pts/mo) across 68 sites/15 countries. Ken Culver, MD (@ALKPositiveinc) shows how patient-led outreach can accelerate ALK+ trial recruitment as 40 therapy trials emerge. #DAVALung
ALKOVE-1
[Slide 1]
Enrollment in ALKOVE-1 Was Robust! This was the first trial we actively promoted across our communication channels.
Enrollment curve: ALKOVE-1 December 11, 2024: 596 (133 Phase 1 + ALK Phase 2). Phase 1 + 2 September 2024: 362. Transition to Phase 2 February 2024: 133. Phase 1 August 2023: 93. Phase 1 Initiation June 2022.
39.4 pts/month (N=394). (68 sites in 15 countries). Feb 2024 - Nov 2024 (10 months).
Our Contributions to Enrollment | Number Reached: Social Media (6 platforms) ~14,000; Newsletters (Every other month) ~11,000; ALKtALK Expert presentations (2 per month) 150-300 each ZOOM meeting (Thousands of views on YouTube); ALK Patient Summit (Each July) ~1,500 (550 in person, 1000 virtually, Thousands of views on YouTube); Patient/Care Partner Medical Committee meetings (Weekly) 30/week; Patient dialogue on the ALK Positive private Facebook group 3,000-4,000.
Draft courtesy of Jim Porter - CEO, Nuvalent. ALK POSITIVE Improving Patient Outcomes Worldwide.
———
[Slide 2]
How Many Trials Need to be Enrolled? Not including FIH, general solid tumor or country-specific trials not in clinicaltrials.gov.
Drug | No. of ALK Lung Cancer Therapy Trials | No. of ALK Observational Studies: Alectinib 6 / 4; AQUA07 1 / 0; Brigatinib 0 / 2; Ensartinib 11 / 2; Gilteritinib 2 / 0; Immunotherapy 4 / 0; Iruplinalkib 3 / 3; Lorlatinib 8 / 5; Neladalkib 3 / 0; Other 1 / 1; TRI-611 1 / 0. TOTAL 40 / 16.
Immunotherapy: ARCHER, BNT116, Ivonescimab, and Pembrolizumab + bevacizumab. Other: Radiotherapy.
More Trials Are Coming! Company/Institution | MOA | Start Dates: Nuvectis Pharma SRC/YES1 inhibitor 2026; Tango Therapeutics PRMT5 inhibitor 2026; NIH combination study TBD 2026; Break Through Cancer ALK Vaccine 2027; ALKemist Bio ALK TCR-T 2027.
We are focused on enrolling 13 trials and we will add the Nuvectis and Tango trials opening this year.
ALK POSITIVE.
———
[Slide 4]
ALK Positive Enrollment Support Activities (1) - Enhanced Recruitment Activities.
1. Speaking with new investigators about facilitating enrollment: a. Sending emails to zip codes around sites to create awareness. b. Planning to add webpages for trials to highlight sites.
2. New clinical trial education programs: a. Started a monthly clinical trial newsletter. b. Initiated monthly evening clinical trial ZOOM calls. c. Created an ALK Clinical Trial Finder.
3. Continue multi-channel communications: a. General email announcements about trials. b. Announcements on ALKtALK and social media platforms. c. Acknowledging and informing our donors.
4. Expand collaborations with other ALK groups globally: a. Sharing upcoming trial site openings. b. Establish a common global communication platform.
5. Collaborating with sponsoring companies (examples): a. Joining with Astellas when they speak with investigators. b. Meeting with Triana once or twice per month.
NEW TREATMENT OPTION FOR ALK+ IN ST. LOUIS, MO. A clinical trial for ALK-positive lung cancer is now open at Washington University School of Medicine in St. Louis.
ALK POSITIVE Improving Patient Outcomes Worldwide.
Theme · 15 talks
Radiation, Theranostics & Locally Advanced
SBRT, hypofractionation, MR-guided and biology-guided RT, radioenhancers (NBTXR3), TTFields, theranostics, and the post-PACIFIC stage III landscape.
Where does the field go beyond PACIFIC? @HenryParkMD from @YaleMed discussed ongoing efforts in NSCLC, including consolidative IO combinations, induction chemo-IO before chemo-RT, and ctDNA as a biomarker for future trial design. #DAVALung
AFT-16APOLOPACIFIC
[Slide 1]
Unresectable: Consolidative Immunotherapy
PACIFIC
- Unresectable stage III NSCLC randomized to durvalumab x 12 months vs. placebo AFTER completing chemo-RT to 54-66 Gy
- PFS and OS improved on durvalumab arm (persisted at 5-year follow-up)
- 5-year OS 43%, PFS 33%
OS KM curve (OS probability vs Time Since Random Assignment, months); Durvalumab vs Placebo.
Antonia et al, NEJM 2017 and 2018; Spigel et al, JCO 2022
———
[Slide 2]
Induction Chemo-IO then Chemo-RT?
CURRENT STANDARD VS EMERGING APPROACH
Current Standard: PACIFIC Paradigm - Concurrent Chemoradiotherapy (cCRT) -> Consolidation ICI; Reliance on ICI sensitivity to eradicate micrometastatic disease
Emerging Approach: Induction ChemoICI - Induction Chemo + ICI -> Concurrent Chemoradiotherapy (cCRT) -> Consolidation ICI; Upfront systemic therapy may treat micrometastatic disease and downstage tumor
POTENTIAL BENEFITS & CONCERNS OF INDUCTION: Improved PFS & OS suggested; Tumor downstaging (smaller RT fields); Early micrometastatic eradication; Delays local therapy initiation; Potential additional toxicity
Piper-Vallillo and Park, Lung Cancer 2026
———
[Slide 3]
Induction Chemo-IO then Chemo-RT?
Approach | Study (Phase, R) | Treatment Schedule | Consolidation ICI | Sample Size | Endpoints (1/2) | 24-mo PFS | 24-mo OS | Pneumonitis Risk
Consolidative ICI: PACIFIC (3R) | No Induction, No Concurrent | Durva (12 mo) vs Placebo | 713 pts | 1/2 PFS; OS, ORR, DoR, Safety (SS) | 45% vs 25% (SS) | 66% vs 55% (SS) | 3.4% vs 2.6% G3/4
Induction & Consolidative ICI:
AFT-16 (2) | Atezo (4) | Atezo (12 mo) | 62 pts | 12-wk DCR; PFS, OS, ORR, Safety | 54% | 74% | 3.2% (2 G3) 1 case "pneumonia"
APOLO (2) | Chemo-atezo (3) | Atezo (12 mo) | 38 pts | PFS; OS, ORR, Safety | 50% | 60.5% | C3 (consolidation phase)
inTrist/CCOG0074 (2R) | Tori (1) vs. Chemo | Tori (12 mo) | 52 pts | PFS; ORR, Pneumonitis | 85.6% vs 54.5% (12 mo, SS); 77.8% vs 40% (24 mo) | NR | C3: 11.3 vs 4% C2: 18.3 vs 36% No G4/5
GASTO-1091/CA207-7AL (2R) | Chemo-nivo (2) | Nivo (12 mo) vs Obs | 172 pts | PFS; OS, ORR, Safety | 64.8% vs 42.3% (18 mo, SS) | 73% vs 61% (18 mo, SS) | G3 Induction 15% C3; cCRT 2.9%; consolidation 9.9%; Consolidation obs 2.3 vs 7.3%
Piper-Vallillo and Park, Lung Cancer 2026
———
[Slide 4]
Take-Home Points
- PACIFIC with concurrent chemo-RT to 60 Gy in 30 fractions then consolidative immunotherapy for up to 12 months is standard-of-care if negative for EGFR/ALK driver mutations
- Do NOT use concurrent immunotherapy with chemo-RT
- No improvement on PACIFIC in the past decade, but exciting areas for clinical trials:
- Combination consolidative IO after chemo-RT
- Induction sequencing of chemo-IO before chemo-RT
- Assess role of ctDNA as biomarker
Resectability is changing in stage III NSCLC. @ErinGillaspie discusses MDT-BRIDGE, neoadjuvant durvalumab+chemo, ctDNA, and why guidelines must adapt to immunotherapy-era nodal clearance. #DAVALung @VUMChealth
MDT-BRIDGE
[Slide 1]
EORTC Survey
Resectability by T and N stage (N0, N1, N2-single, N2-multi, N2-bulky, N2-invasive):
T1-2: N2-single POTENTIALLY RESECTABLE (95%); N2-multi NO AGREEMENT (50%); N2-bulky UNRESECTABLE (75%); N2-invasive UNRESECTABLE (84%)
T3 size: N1 RESECTABLE (83%); N2-single POTENTIALLY RESECTABLE (87%); N2-multi NO AGREEMENT (39%); N2-bulky UNRESECTABLE (80%); N2-invasive UNRESECTABLE (88%)
T3 satellite: N1 POTENTIALLY RESECTABLE (94%); N2-single POTENTIALLY RESECTABLE (79%); N2-multi NO AGREEMENT (34%); N2-bulky UNRESECTABLE (84%); N2-invasive UNRESECTABLE (91%)
T3 invasion: N1 POTENTIALLY RESECTABLE (89%); N2-single NO AGREEMENT (71%); N2-multi NO AGREEMENT (28%); N2-bulky UNRESECTABLE (87%); N2-invasive UNRESECTABLE (92%)
T4 size: N0 POTENTIALLY RESECTABLE (94%); N1 POTENTIALLY RESECTABLE (90%); N2-single NO AGREEMENT (66%); N2-multi UNRESECTABLE (77%); N2-bulky UNRESECTABLE (88%); N2-invasive UNRESECTABLE (93%)
T4 satellite: N0 POTENTIALLY RESECTABLE (78%); N1 NO AGREEMENT (71%); N2-single NO AGREEMENT (44%); N2-multi UNRESECTABLE (85%); N2-bulky UNRESECTABLE (92%); N2-invasive UNRESECTABLE (94%)
T4 invasion: N0 NO AGREEMENT (62%); N1 NO AGREEMENT (57%); N2-single NO AGREEMENT (34%); N2-multi UNRESECTABLE (90%); N2-bulky UNRESECTABLE (95%); N2-invasive UNRESECTABLE (94%)
———
[Slide 2]
Stage III is heterogeneous
IIIA - SURGERY: Surgical opportunities More likely (T4 N0, T4 N1, T3 N1; T4inv N0,1; T3inv N1; T3 5-7 N1)
IIIB (T2 N2a, T3 N2a, T1 N2b, T4 N2a; T4inv N2a; T3 4 N2b; T3inv N2a; T3 5-7 N2a; T2 N2b; T2a,b N3; T2b N3)
IIIC - ?? SURGERY: Surgical opportunities Less likely (T1a,b,c N3, T4 N3; T3 N3, T4 N3; T3 N3)
———
[Slide 3]
ASCO
"Patients with Stage III NSCLC should not be excluded from consideration from surgery by non-surgery physicians"
(Treatment algorithm flowchart: Patients with confirmed stage III NSCLC -> Multidisciplinary discussion or consult with the surgeon -> Resectable vs Unresectable pathways; neoadjuvant chemotherapy; surgery with resected stage III/complete resection; EGFR-mutation osimertinib; PD-L1 ≥1% atezolizumab; concurrent chemotherapy and RT; consolidation durvalumab. PMID: 37671675)
———
[Slide 4]
MDT-BRIDGE: neoadjuvant durvalumab + CTx followed by surgery and durvalumab or CRT and consolidation durvalumab in resectable, Stage IIB-IIIB NSCLC
Neoadjuvant period A: Baseline MDT assessment -> Durvalumab + CTx q3w x 2 cycles -> MDT decision, restaging/pathological confirmation
Neoadjuvant period B: Resectable -> Durvalumab + CTx q3w x 1-2 cycles -> Surgery; Unresectable -> CRT 6 one-week cycles for 6 weeks
Adjuvant/consolidation treatment: Durvalumab monotherapy q4w for 1 year
Key inclusion criteria:
- Resectable and borderline resectable, previously untreated Stage IIB-IIIB N2 NSCLC
- WHO/ECOG PS 0-1
- ≥1 target lesion
- EGFRwt / ALKwt
N=140
Primary endpoint: Resection rate, defined as proportion of all participants who underwent definitive surgery
Blood samples for ctDNA assessment; whole blood and plasma at C1D1, only plasma at subsequent timepoints. Tissue sample (ie, biopsy); not required post-CRT timepoint.
Reck M, et al. Poster presented at ESMO IO 2023 (Abstract 115TiP)
Where does ablative RT fit in the immunotherapy era? @ajuloorimd from @UChicagoMed, reviewed multi-site SBRT with dual checkpoint blockade as a potential strategy to improve outcomes in metastatic NSCLC. #DAVALung
[Slide 1]
Local therapies may be additive to systemic therapy
Upfront:
- relieve large tumor bulk related immunosuppression via cytoreduction
- ablate sites of existing disease that may be early sites of treatment failure, leading to declining performance status or tumor-related death
COSINR (current study)
Consolidation:
Can help perhaps improve long term outcomes in patients who have already shown a response to treatment
NORTHSTAR, Gomez Trial, SABR-COMET, NRG LU002
———
[Slide 2]
COSINR Trial
Resectable NSCLC, C-metastasis mine, autopsy rejection of PD-L1 expression (study schema)
RANDOMIZE Bioreaction selection
SEQUENTIAL ARM (a): SBRT to all metastases; Ipilimumab/nivolumab following SBRT; then continue maintenance
CONCURRENT ARM (b): Nivolumab/ipilimumab QD +/- SBRT to all metastases; Ipi/nivo continuation
- Dose-Finding Cohort
- N = 37 patients randomized to sequential or concurrent treatment
19 sequential
18 concurrent
———
[Slide 3]
SBRT
Goal of RT here is to be safe, short course, small field, and ablative
As such:
- Prioritized organ at risk (eg. heart, esophagus, trachea/bronchi, bowel) dose constraints over target coverage
- Large tumors allowed (only central 65 cc of tumor treated)
- Not all metastases were treated (goal is cytoreduction). Up to 4 isocenters allowed for treatment
Mediastinal/Hilar SBRT: R lung, bilateral hila, subcarinal nodal disease treated with 50 Gy in 5 fractions with prioritization of esophagus and proximal bronchial tree constraints
———
[Slide 4]
Results
- Of 97 patients screened, 75 patients enrolled between 2017-2022 and all received SBRT and at least one cycle of immunotherapy
56 patients treated concurrently, 19 patients treated sequentially
- Data lock 6 months after final patient was enrolled
- Median F/U of 16.3 months (IQR 7.6-34.7 months)
- Median time from treatment to data lock - 36.6 months
Conclusions
- CYTOREDUCTIVE multi-target SBRT appears to be safe with dual checkpoint immunotherapy
- overall survival is promising, with a median of 34 months
- RT may have a role outside of oligometastatic/'abscopal' domains
- Selection criteria needed for who is likely to benefit from upfront multi-site local therapy
Dr. @Lawson_Eng (@pmcancercentre) presented data linking pre-ICI antibiotic and PPI exposure to poor outcome via gut microbiome changes, including a PACIFIC trial analysis, with FMT explored to restore the microbiome. #DAVALung
PACIFIC
[Slide 1]
[Slide A] Impact of Prior Antibiotic Exposure on ICI Outcomes
- Total sample size n=2737; majority of patients had metastatic disease; median OS 306 days
- 59% exposed to antibiotics 1 year prior to ICIs; 19% exposed 60 days prior to ICIs; 53% of patients had lung cancer
OS curves: 1 Year before ICI Exposure (Log rank test P=.0002) and 60 days before ICI Exposure (Log rank test P=.004); Not exposed vs Exposed.
Table:
- Any Antibiotic Exposure (Yes vs No): 1 year before ICI aHR = 1.12 (1.01-1.24), p=0.03; 60 days before ICI aHR = 1.06 (0.94-1.20), p=0.35
- Total weeks of Exposure (Per 1 week increase): 1 year aHR = 1.01 (1.00-1.02), p=0.10; 60 days aHR = 1.02 (0.98-1.06), p=0.39
Multivariate results adjusted for age, sex, BMI, facility level of cancer centre, autoimmunity history, John Hopkin's ACG score and hospitalization within the last year.
Any antibiotic exposure up to 1 year before ICI was associated with poorer OS. Source: Eng L. J Clin Oncol. 2023 Jun 10;41(17):3122-3134
[Slide B] Impact of Prior Antibiotic Exposure on ICI Outcomes
- What about the effects of specific antibiotic classes? Subgroup analysis based on major classes
- 29% exposed to penicillin, 24% cephalosporins, 28% fluoroquinolones 1 year prior to ICIs
OS curves: 1 Year before ICI Exposure (Log rank test P<.0001) and 60 days before ICI Exposure (Log rank test P=.0007).
Table:
- Any Fluoroquinolone Exposure (Yes vs No): 1 year aHR = 1.26 (1.13-1.40), p<0.001; 60 days aHR = 1.20 (0.99-1.45), p=0.06
- Total weeks of Exposure (Per 1 week increase): 1 year aHR = 1.07 (1.03-1.11), p=0.0002; 60 days aHR = 1.12 (1.03-1.23), p=0.01
- Fluoroquinolone exposure 1 year and 60 days before ICI was associated with poorer OS
- No significant associations seen with other classes of antibiotics (Penicillin, Cephalosporins)
Source: Eng L. J Clin Oncol. 2023 Jun 10;41(17):3122-3134
———
[Slide 2]
[Slide A] Impact of Antibiotic Exposure on PACIFIC trial
- Secondary analysis evaluating exposure to antibiotics and PPIs 30 days prior to starting on Durvalumab on PFS and OS among patients on PACIFIC trial
- 10% of Durvalumab arm patients exposed to antibiotics, 11% in placebo arm
Progression Free Survival: Median PFS (95% CI) - No antibiotic exposure 15.6 months (95% CI 13.4-17.6); Previous antibiotic exposure 9.2 months (95% CI 4.9-18.1); HR 1.50 (95% CI 1.08-2.10); p=0.016.
Overall Survival: Median OS (95% CI) - No antibiotic exposure 49.2 months (95% CI 39.7-57.3); Previous antibiotic exposure 37.7 months (95% CI 18.8-NC); HR 1.33 (95% CI 0.90-1.97); p=0.16.
- Exposure to antibiotics worsened PFS and a trend towards worse OS among patients receiving Durvalumab in PACIFIC trial
- Exposure to antibiotics did not impact the placebo arm
Source: Brunetti L. Lancet Oncol. 2026 Jul 3:S1470-2045(26)00191-9
[Slide B] What about other concomitant drugs?
- Many other drugs being explored that potentially impact ICI efficacy (i.e. PPIs)
Re-analysis of Ontario-wide cohort on PPI exposure (1 Year and 60 days before ICI Exposure; Log Rank Test p<0.0001 and p<0.0001).
Analysis of PPI Exposure on PACIFIC data: OS - No PPI exposure 51.9 months (95% CI 43.8-NC); Previous PPI exposure 33.0 months (95% CI 21.9-46.7); HR 1.66 (95% CI 1.19-2.31); p=0.003. PFS - No PPI exposure 17.2 months (95% CI 15.4-23.2); Previous PPI exposure 9.6 months (95% CI 7.4-13.7); HR 1.30 (95% CI 0.93-1.82).
Table:
- Any PPI Exposure (Yes vs No): 1 year aHR = 1.21 95% CI (1.09-1.33), p<0.001; 60 days aHR = 1.26 95% CI (1.13-1.40), p<0.001
- Total weeks of PPI Exposure (Per 1 week increase): 1 year aHR = 1.00 per week (1.00-1.01), p=0.05; 60 days aHR = 1.01 per week (1.00-1.02), p=0.009
- Exposure to PPIs prior to starting ICI leads to poorer outcomes; Dose effect observed with exposure to PPI
Source: Eng L. ESMO 2023; Brunetti L. Lancet Oncol. 2026 Jul 3:S1470-2045(26)00191-9
———
[Slide 3]
[Slide A] What are some ways to limit the effects of antibiotics?
BOX 1. Recommendations for Judicious Use of ATB in Patients Treated With Immune Checkpoint Inhibitors: Oncologists should follow the joint IDSA/ASCO guidelines, which recommend antibiotic (ATB) stewardship in patients with cancer, particularly for those treated with ICI. ATB should be used judiciously by: 1. Confirming and documenting the presence of a bacterial infection using a culture, when possible; 2. Following local ATB stewardship guidelines; 3. Opting for the narrowest-spectrum ATB for the shortest effective duration when ATB are necessary; 4. Continuously reassessing the need for ATB; 5. Establishing multidisciplinary care with infectious disease experts.
- Focus on antibiotic stewardship
- Try to confirm an infection first prior to treatment
- Use a narrow spectrum and short duration of antibiotics to limit negative effects of antibiotics on ICI outcomes
- Limit polypharmacy for other drugs (i.e., PPIs) that can potentially impact gut microbiome or use alternative drugs (i.e. H2 blockers instead of PPIs)
Source: Elkrief et al. Am Soc Clin Oncol Educ Book. 2025 Jun;45(3):e472902
[Slide B] What are some strategies to reverse this?
- Multiple strategies are underway to try to modulate the gut microbiome
Table of TYPES OF INTERVENTIONS: DIET, PREBIOTICS, PROBIOTICS, FMT, STOOL SUBSTITUTES, ANTIBIOTICS (rows: How it works, Advantages, Disadvantages, Examples of ongoing trials with NCT numbers e.g. NCT03700437, NCT04316620, NCT03595540, NCT03870607, NCT02763033, NCT04046653, NCT01895530, NCT03829111, NCT04225307, NCT03341143, NCT03772899, NCT03353402, NCT04264975, NCT03686202, NCT03388601, NCT04208958, NCT03817125, NCT03962920, NCT04208958).
Source: Araujo et al. Cancer Treatment Reviews 92 (2021) 102072
———
[Slide 4]
Early Results from Fecal Microbiome Transplant Studies
- Phase II open label study for patients with metastatic NSCLC and melanoma
- Patients receive single dose of FMT from a healthy donor prior to starting ICI therapy
FMT-LUMINate clinical trial design NCT04951583: Bowel preparation PEG Lyte -> 24h -> Healthy Donor 1 donor per FMT -> 7d -> Cohorts: NSCLC (PD-L1 >50%, Pembrolizumab, n=20); Cutaneous melanoma (Ipilimumab + nivolumab, n=20); Uveal melanoma (Ipilimumab + nivolumab, n=5). Primary: ORR in NSCLC. Secondary: ORR, PFS, OS, Safety, Donor-host similarity. Salvage FMT if antibiotics on trial.
NSCLC: ORR 80% (16/20); DoR: 9 months; No Grade 3 irAEs
Melanoma: ORR 75% (15/20); DoR: 10 months; 60% developed grade 3 irAEs
- Responders developed a distinct post-FMT gut microbiome composition compared to non-responders independent of donor-recipient similarity
- Correlative analysis evaluating re-introduction of some baseline bacterial species in FMT in antibiotic treated mice from 2 NSCLC responder patients lead to inhibition of ICI responses
Source: Duttagupta et al. Nat Med. 2026 Apr;32(4):1337-1350
Can HPV ctDNA act as a real time biomarker and personalize chemoradiation? Jonathan Schoenfeld (@jdschoenfeld1, @DanaFarber) discusses ReACT 1.0, using HPV ctDNA response to guide RT intensity and monitor recurrence risk in HPV+ OPC. #DAVALung
[Slide 1]
ReACT Outcomes
All de-escalated patients: 2-year PFS 0.93, 95% CI (0.87-0.99). Number at risk (Follow-up time in months 0-48): 89, 85, 65, 50, 39, 22, 15, 4, 0. Median follow-up: 24.7 months (5.1-51+).
Initially low-risk de-escalated patients (Non-T4, <=10 py): 2-year PFS 0.93, 95% CI (0.88-1). Number at risk: 60, 59, 46, 40, 30, 20, 12, 4, 0.
Initially intermediate-risk de-escalated patients (T4, >10 py): 2-year PFS 0.90, 95% CI (0.83-1). Number at risk: 29, 26, 19, 10, 9, 2, 3, 0, 0.
———
[Slide 2]
Improving patient selection / treatment adaptation
(Old paradigm, struck through:) Diagnosis -> Risk Group (p16/stage) -> Fixed Treatment -> Outcome
New paradigm: Diagnosis -> Improved patient selection (ctDNA) -> Initial Treatment -> On-Treatment Feedback (ctDNA) -> Adaptive De-escalation or Escalation. [Highlighted:] ctDNA guided de-escalation. Slide 226
———
[Slide 3]
ReACT 1.0: Unfavorable HPV ctDNA profile predicts recurrence
Study flow: Total patients screened (N=143) -> Excluded, screen-failed (N=41) [Undetectable HPV DNA score pre-treatment (N=15); HPV DNA score <200 and intermediate risk (N=13); Non-HPV16 disease (N=9); No follow-up recorded (N=3); Comorbid conditions (N=1)]. Total patients enrolled, safety set (N=102) -> Efficacy evaluable set (N=102) -> Low-risk (N=60) received de-escalation treatment; Intermediate-risk, cleared HPV DNA (N=29) received de-escalation treatment; Intermediate-risk, failed to clear HPV DNA (N=13) received standard treatment.
Source: Schoenfeld et al. ESMO 2025. Slide 232
———
[Slide 4]
ctDNA-guided response adapted de-escalation: ReACT 1.0
Columns: Clinical risk | TTMV-HPV DNA | Treatment
LOW-RISK ARM: T0-3, N0-2 disease and <=10 pack-year smoking history | Any detectable score pre-treatment | Reduced dose IMRT +/- lower dose chemotherapy
INTERMEDIATE-RISK ARM: T4, N0-2 disease and/or >10 pack-year smoking history | FAVORABLE: Score >200 pre-treatment and >95% clearance by week 4-5 of treatment -> Reduced dose IMRT +/- lower dose chemotherapy | UNFAVORABLE: Score <=200 pre-treatment or <=95% clearance by week 4-5 of treatment -> Standard dose IMRT with chemotherapy
Source: NCT04900623, ASCO 2025. PI: Glenn Hanna, Jonathan Schoenfeld. Hanna...Schoenfeld Nat Comm 2026, in press. Slide 227
Which patients with oligometastatic NSCLC benefit most from local consolidative therapy? At #DAVALung, Dr. @sgswisher (@MDAndersonNews) reviews NRG-LU002, contrasts it with MDACC Phase II trial & explores emerging selection factors lke disease burden, induction response, & ctDNA
[Slide 1]
Local consolidative therapy versus maintenance therapy or observation for patients with oligometastatic non-small-cell lung cancer without progression after first-line systemic therapy: a multicentre, randomised, controlled, phase 2 study. Local Consolidative Therapy Vs. Maintenance Therapy or Observation for Patients With Oligometastatic Non-Small-Cell Lung Cancer: Long-Term Results of a Multi-Institutional, Phase II, Randomized Study.
PFS: 11.9 vs 3.9 mos; HR: 0.35; p=0.0054.
OS: 41.2 vs 17 mos; HR: 0.46; p=0.017.
Gomez, Swisher, Heymach et al., Lancet Oncol, 17:1673, 2016. Gomez, Swisher, Heymach et al., JCO, 37:1558, 2019.
———
[Slide 2]
Oligo NSCLC: NRG-LU002 Trial
Gr 2 Pneumonitis; PFS/OS > 3 mos
PFS: p=0.0039 (logrank) HR (95% CI)=3.17 (1.39, 7.28). No Pneumonitis at-risk 170 108 91 71 50 34 22; Pneumonitis 7 1 1 1 1 1. 2 yr 14% vs 42%; HR: 3.17, p=0.0039.
OS: p=0.0002 (logrank) HR (95% CI)=4.26 (1.85, 9.81). No Pneumonitis at-risk 188 158 136 111 78 52 36; Pneumonitis 7 1 1 1 1 1. 2 yr 57% vs 14%; HR: 4.26, p=0.002.
1: No Pneumonitis; 2: Pneumonitis. Iyengar et al, ASCO 2024
———
[Slide 3]
Oligo NSCLC - Insights on NRG vs MDACC Trial Differences
1. Immunotherapy (86%) vs Chemo (14%): Better Systemic/Local Control - diluting out effect of LCT; Higher Toxicity - RT after IO: Grade >=3 pneumonitis (10% vs 1%, p=0.02); Early pneumonitis associated worse PFS/OS; Surgery not allowed to treat primary in LU002; Radiation induced immunosuppression?
2. More induced Oligomet on LCT arm (13% vs 7%): OS for induced oligo in multivariate: HR 1.68, P=0.08.
3. No EGFR/Alk pts - most benefitted by LCT?
4. IO may have led to no repeated consolidation?
———
[Slide 4]
Combinations of LCT with Targeted Therapy
NorthStar Trial - EGFR+ - Ph II Rand - MDACC
BrightStar Trial - ALK+ - Single Arm Ph I - MDACC
Mutation pie chart: EGFR 14.5%, KRAS 19.3%, KIT 6.8%, PIK3CA 6.8%, MET 3.9%, ALK 2.1%, RET 0.5%, BRAF 1.9%, HER2 0.2%, ROS1 0.3%, Others 50.4%.
NorthStar Progression Free Survival: PFS events (%) Osi+/-LCT: Osimertinib 50 (79.3%), Osimertinib plus LCT 42 (75%); Median PFS month Osi 17.5 (14.4, 24.3), Osi+LCT 29.5 (19.4, 45.0); HR 0.86; 95% CI (0.30, 0.67); P value (1-sided log rank) 0.025. Gandhi et al.
BrightStar Progression Free Survival: PFS Ratio BrightStar / ALTA-1L (first line single agent targeted therapy): 5-yr 51% / 30%; 6-yr 61% / 30%; 7-yr 61% / 47%. (Includes only patients who did not progress at 12 mos on ALTA-1L). Elamin et al.
PI: Y. Elamin; J. Heymach, S. Gandhi, D. Gomez, B. Sepesi, M. Antonoff, S. Swisher et al. NCCN Funded. MDACC, MSKCC, UCSF, U of CO.
In metastatic NSCLC progressing after platinum, adding TTFields to SOC improved median OS (13.2 vs 9.9 mo; HR 0.74, P=0.035) without a PFS or ORR benefit, effect concentrated in the ICI subgroup. Dr. Corey Langer (@PennCancer) on LUNAR. #DAVALung
[Slide 1]
LUNAR Phase 3 Study Design
Objective: To evaluate safety and efficacy of TTFields therapy with standard of care (SOC) compared to SOC alone in metastatic NSCLC progressing on or after platinum-based therapy
Key eligibility criteria: >=22 years of age; Metastatic NSCLC; Progression on/after platinum-based therapy; ECOG PS 0-2
Baseline evaluation (incl. MRI) -> N=276 Randomized(1:1) -> TTFields therapy + SOC (Investigator's choice ICI or docetaxel) / SOC (Investigator's choice ICI or docetaxel); Q6W follow-up until progression; 3 post-progression follow-up visits; Survival follow-up
Stratified by (1) Region, (2) SOC treatment, (3) Histology
Data cut-off: November 26, 2022
Study sites: 124 in 17 countries (North America, Europe, Asia)
Ticiana Leal, MD, Winship Cancer Institute - Emory University, ASCO 2023
———
[Slide 2]
Overall Survival in the ITT Population
TTFields + SOC (n=137) / SOC (n=139)
Median OS (95% CI), months: 13.2 (10.3-15.5) / 9.9 (8.1-11.5)
1-year survival (95% CI): 53% (44-61) / 42% (34-50)
3-year survival (95% CI): 18% (11-27) / 7% (2-15)
HR (95% CI): 0.74 (0.56-0.98); P=0.035
Median (range) follow-up 10.0 (0.03-58.7) months
Overall Survival in ICI and DOC-Treated Patients
TTFields + ICI (n=66) / ICI (n=66):
Median OS (95% CI), months: 18.5 (10.6-30.3) / 10.8 (8.2-18.4)
1-year survival: 60% (47-71) / 46% (33-57)
3-year survival: 27% (15-42) / 9% (3-21)
HR (95% CI): 0.63 (0.41-0.96); P=0.03
TTFields + DTX (n=71) / DTX (n=71):
Median OS (95% CI), months: 11.1 (8.2-14.1) / 8.7 (6.3-11.3)
1-year survival: 46% (33-57) / 38% (27-49)
3-year survival: 9% (3-20) / 5% (0-18)
HR (95% CI): 0.81 (0.55-1.19); P=0.28
———
[Slide 3]
Response Rates in the ITT Population
TTFields + SOC (n=137) / SOC (n=139)
Patients with a follow-up scan: n=122 / n=127
ORR, % (95% CI): 20% (14-28) / 17% (11-25)
Difference in ORR, % (95% CI): 3% (-8.5-15.0); P=0.5
Best overall response, %: Complete response 3% / 1%; Partial response 18% / 17%; Stable disease 49% / 47%; Progressive disease 18% / 26%; Not evaluable 2% / 1%
- All 5 complete responses occurred in patients receiving an ICI - 4 with TTFields therapy - 1 with ICI alone
- Analysis of patterns of progression (infield vs outfield) is ongoing
Safety and Tolerability
TTFields + SOC (n=133) / SOC (n=134); All grades / Grade >=3
Any AE: 97% / 59% ; 91% / 56%
Dermatitis: 43% / 2% ; 2% / 0%
Fatigue: 28% / 4% ; 37% / 8%
Musculoskeletal pain: 36% / 3% ; 27% / 4%
Dyspnea: 20% / 7% ; 25% / 3%
Anemia: 23% / 8% ; 22% / 8%
Diarrhea: 19% / 2% ; 19% / 0%
Cough: 18% / 0% ; 19% / 1%
Nausea: 19% / 0% ; 16% / 0%
Leukopenia: 17% / 14% ; 18% / 14%
Pneumonia: 15% / 11% ; 17% / 11%
Alopecia: 10% / 0% ; 17% / 1%
Respiratory tract infection: 15% / 3% ; 16% / 0%
Localized edema: 15% / 1% ; 16% / 2%
Any serious AE: 53% / 38%; Any AE leading to discontinuation: 36% / 20%; Any AE leading to death: 10% / 8%
- Increased inc of dermatitis associated with Tx arrays, mostly gr 1-2; Majority of patients (94%) had >=1 AE; Comparable incidence of grade >=3 AEs between arms; No difference in rate of pneumonitis or other immune-related AEs; No exacerbation of systemic toxicities; No notable differences in HRQoL when TTFields therapy was added to SOC
———
[Slide 4]
Langer's Modified Conclusions
- Pivotal, phase 3 LUNAR study met its primary endpoint
- TTFields therapy with SOC provided a statistically significant and clinically meaningful 3-month improvement in median OS vs SOC (HR: 0.74, P=0.035) with no added systemic toxicities, despite the absence of an improvement in RR% or PFS
- Statistically significant ~8-month increase in median OS (from 10.8 to 18.5 months) was demonstrated with TTFields therapy and an ICI (HR: 0.63, P=0.030)
- The survival benefit of TTFields therapy + ICI (vs ICI alone) appeared more pronounced in patients with PD-L1-positive (TPS >=1%) tumors
- PD-L1-positive: median OS was 23.6 months vs 10.5 months; HR 0.49; P=0.045
- PD-L1-negative: median OS was 9.6 months vs 9.1 months; HR 0.98; P=0.95
- There was a 2.4-month difference in median OS (from 8.7 to 11.1) for TTFields therapy and docetaxel vs docetaxel alone (HR: 0.81, P=0.28)
- TTFields therapy should be considered part of SOC for metastatic NSCLC after progression on/after platinum-based therapy
- TTFields therapy is a potentially paradigm shifting new treatment modality
- Phase III trial of TTFields therapy with current SOC for first-line metastatic is underway (EF-36/Keynote B36/NCT04892472), and being considered as consolidation in locally advanced NSCLC
LUNAR 2: Study Design, Eligibility and Objectives
Adults with non-driver mutated, previously untreated mNSCLC (N=734)
7 days Screening and baseline evaluation
Induction: TTFields (150 kHz) + pembrolizumab (200 mg) + platinum-based chemotherapy / pembrolizumab (200 mg) + platinum-based chemotherapy
4 cycles Q3W
Maintenance: TTFields (150 kHz) + pembrolizumab (200 mg) +/- pemetrexed / pembrolizumab (200 mg) +/- pemetrexed
Follow-up Q3W; treatment until progression; CT scan Q9W
Endpoints: Primary OS and PFS; Secondary OS and PFS by histology and PD-L1 TPS, ORR DoR and DCR, PFS rates at 6/12/24/36 months, 1/2/3-year survival rates, Safety profile; Exploratory PFS and OS by in-field and out-of-field location
Stratification factors: PD-L1 TPS (<1% vs 1-49% vs >=50%); Histology (squamous vs non-squamous); Prior immunotherapy (yes vs no)
Inclusion criteria: Histologically/cytologically confirmed mNSCLC; No prior systemic treatment for mNSCLC; Evaluable disease in the thorax per RECIST v1.1; >=18 years old; ECOG PS 0-1
What has head and neck cancer taught us about radiation-IO sequencing? At #DAVALung, Dr. Jonathan Schoenfeld (@MassGenBrigham) reviews CRT + IO, adjuvant and neoadjuvant PD-1 strategies, NIVOPOSTOP, and KEYNOTE-689 EFS data.
IMvoke010KEYNOTE-412KEYNOTE-689NIVOPOSTOP
[Slide 1]
Benefit of PD-1/PD-L1 inhibitors in R/M HNSCC patients led to studies in patients with locally advanced disease (surgical and non-surgical patients)
Mucosal squamous cell carcinoma (HNSCC): nasopharynx, main nasal cavity, oropharynx, oral vestibule, hypopharynx, main oral cavity, esophagus, larynx, trachea
Vorwerk and Hess Radiation Oncology 2011, 6:97
Timing of immunotherapy in HNSCC studies (surgical and definitive RT): IMRT +/- chemotherapy (Definitive and adjuvant); Neoadjuvant/induction immunotherapy; Concurrent immunotherapy; Outback immunotherapy
———
[Slide 2]
Concurrent IO (JAVELIN / KN412 Studies) Results: Starting immunotherapy concurrently with CRT doesn't improve outcomes
[JAVELIN HN: Red: Placebo; Blue: Avelumab; Avelumab plus chemoradiotherapy (n=350); Placebo plus chemoradiotherapy (n=347); Median overall survival (95% CI): Not reached (not estimable-not estimable) both arms; Stratified hazard ratio (95% CI): 1.31 (0.93-1.85); One-sided stratified log-rank p value 0.94]
JAVELIN HN results: No benefit in OS, PFS. Lee et al., Lancet Oncol 2021
[Keynote 412: Pembrolizumab group vs Placebo group; HR 0.90 (95% CI 0.71-1.15)]
Keynote 412 results: No benefit in OS, EFS. Machiels et al., Lancet Oncol 2024
———
[Slide 3]
Adjuvant PD-1 inhibition in HNSCC Imvoke 010 did not show benefit
[Median investigator-assessed event-free survival: Placebo (n=203); Atezolizumab (n=203); Stratified HR (95% CI) 0.94 (0.70-1.26); Time, mo]
Mix of definitive and adjuvant patients (about 60/40%)
Did not select based on PD-L1 expression
Allowed up to 16-20 weeks to start adjuvant treatment
Ongoing phase 3 studies: JADE, eVOLVE
Imvoke 010 Results, Haddad et al., JAMA 2025
———
[Slide 4]
PD-1 inhibition after surgery for high-risk features: NIVOPOSTOP Trial
[Disease-free survival probability curves: Cisplatin and radiotherapy (n=334); Nivolumab, cisplatin, and radiotherapy (n=352); Time since randomisation (months)]
Bourhis et al., Lancet 2025
For stage III NSCLC, resectability can be complex and multidisciplinary. @sgswisher from @UTMDAnderson highlighted the MDT-BRIDGE approach to reassessing patients after neoadjuvant durvalumab + chemotherapy. #DAVALung
[Slide 1]
MDT-BRIDGE study design
Global, phase 2, non-randomised study (NCT05925530)
Neoadjuvant period A: Baseline MDT resectability assessment (resectable or borderline resectable) -> Durvalumab + investigator's choice of platinum-based CT Q3W for 2 cycles -> MDT reassessment (Restaging/optional pathologic confirmation)
Resectable -> Neoadjuvant period B: Durvalumab + investigator's choice of platinum-based CT Q3W for 1-2 cycles -> Surgery -> Adjuvant/consolidation period: Durvalumab monotherapy Q4W for 12 cycles
Unresectable -> CRT
Key inclusion criteria and study requirements: Aged >=18 years; Previously untreated and pathologically confirmed, resectable or borderline resectable, stage IIB-IIIB NSCLC (per AJCC 8th edition); EGFR/ALKwt (per local test); WHO/ECOG PS 0-1; At least 1 target lesion not previously irradiated; Pre-operative RT not allowed
Primary endpoint: Resection rate, defined as the proportion of all patients who underwent definitive surgery
Secondary endpoints: Resection rate in patients deemed resectable/borderline resectable at baseline; Surgical outcomes in patients who underwent surgery; ORR in patients deemed resectable/unresectable at reassessment; pCR in patients deemed resectable at reassessment; Safety
———
[Slide 2]
Resection rates and outcomes (efficacy subset)
- The overall resection rate was 85.7% and the majority (70/72 patients) had R0 resection
Resection rate, %:
All patients (N=84): 85.7% (95% CI 76.4, 92.4)
Baseline resectable (n=56): 92.9% (95% CI 82.7, 98.0)
Baseline borderline resectable (n=28): 71.4% (95% CI 51.3, 86.8)
Resection outcomes, % (95% CI) - Resected cohort:
All patients (n=72): R0 97.2% (86.7, 98.5); R1 1.4% (0, 7.5); R2 1.4% (0, 7.5)
Baseline resectable (n=52): R0 98.1% (89.7, 100); R1 1.9% (0, 10.3); R2 0% (0, 6.8)
Baseline borderline resectable (n=20): R0 95.0% (65.1, 97.1); R1 5.0% (0.1, 24.9); R2 0% (0, 16.8)
DCO 8 May 2025
———
[Slide 3]
Safety during the post-surgery and CRT-treated period (resected patients subset and safety population)
90-day post-surgery safety summary in patients deemed resectable and borderline resectable at baseline
Post-surgery period, n (%) - Total (N=72) / Resectable at baseline (n=52) / Borderline resectable at baseline (n=20):
Any-grade, all-cause AEs: 56 (77.8) / 40 (76.9) / 16 (80.0)
Maximum grade 3 or 4: 15 (20.8) / 12 (23.1) / 3 (15.0)
Serious AE: 15 (20.8) / 11 (21.2) / 4 (20.0)
Outcome of death: 1 (1.4) / 1 (1.9) / 0
Leading to discontinuation of durvalumab: 1 (1.4) / 1 (1.9) / 0
Any-grade AEs, possibly related to surgery: 12 (16.7) / 8 (15.4) / 4 (20.0)
SAE possibly related to surgery, n (%): Any 6 (8.3); Post-procedural pneumonia 1 (1.4); Pneumothorax 2 (2.8); Duodenal ulcer 1 (1.4); Post-procedural haemorrhage 1 (1.4); Fatigue 1 (1.4)
Safety summary in patients treated with CRT - CRT treatment period, n (%) - All CRT-treated patients (N=18):
Any-grade, all-cause AEs: 14 (77.8)
Maximum grade 3 or 4: 5 (27.8)
Serious AE: 2 (11.1)
Outcome of death: 0
Leading to discontinuation of any study treatment: 1 (5.6)
Leading to dose interruption of any study treatment: 1 (5.6)
Leading to a delay in RT: 1 (5.6)
Any-grade AEs, possibly related to study treatment: 13 (72.2); related to SOC CT 12 (66.7); related to RT 9 (50.0)
Any-grade, immune-mediated AEs; Pneumonitis (any grade): 1 (5.6)
———
[Slide 4]
Conclusions
- 95.2% of patients were able to receive either surgery or CRT
- 85.7% of patients received definitive resection:
- 53/56 (94.6%) patients deemed resectable at baseline remained resectable at reassessment
- 23/28 (82.1%) patients deemed borderline resectable at baseline were reassessed as resectable
- R0 resection rate was 97.2% similar to that observed in AEGEAN (R0 resection rate was 94.7%) despite inclusion of borderline resectable patients
- AEs were similar in the baseline resectable and borderline resectable cohorts; no pneumonitis was noted in those treated with definitive CRT after induction Durva
Initiation of neoadjuvant treatment with durvalumab + CT and close MDT follow-up could allow more patients to receive curative-intent treatment (surgery or CRT)
1. Heymach JV, et al. N Engl J Med. 2023;389(18):1672-84.
Hypofractionation in stage III NSCLC: Dr. @PercyLeeMD (@cityofhope) presents SBRT to the primary tumor followed by chemoradiation to the mediastinum, with phase II median OS 47.1 mo, now tested in phase III NRG LU008. #DAVALung
NRG-LU008PACIFIC
[Slide 1]
PACIFIC: Dominant patterns of failure remains loco-regional
Incidence of New Lesions (BICR): New Lesion Site - Durvalumab (n=476) vs Placebo (n=237)
Any, No. (%): 115 (24.2) vs 79 (33.3)
Lung: 64 (13.4) vs 43 (18.1)
Lymph nodes: 35 (7.4) vs 28 (11.8)
Brain: 31 (6.5) vs 28 (11.8)
Liver: 11 (2.3) vs 8 (3.4)
Bone: 9 (1.9) vs 8 (3.4)
Adrenal: 3 (0.6) vs 5 (2.1)
Others: 10 (2.1) vs 4 (1.7)
TTDM (BICR) in the ITT Population: Durvalumab 226/476 (47.5) median TTDM 36.5 (28.1 to 45.2); Placebo 149/237 (62.9) median TTDM 17.7 (12.7 to 22.1). Stratified HR (95% CI): 0.59 (0.47 to 0.74).
No. at risk: Durvalumab 476...0; Placebo 237...0 (0-72 months).
Spigel DR, et al. J Clin Oncol. 2022;40(12):1301. @PercyLeeMD
———
[Slide 2]
[Slide A] HyCRT-SABR Phase II Study
JAMA Oncology Original Investigation: Accelerated Hypofractionated Chemoradiation Followed by Stereotactic Ablative Radiotherapy Boost for Locally Advanced, Unresectable Non-Small Cell Lung Cancer - A Nonrandomized Controlled Trial. Trudy C. Wu, Elaine Lutenstein, Beth K. Neilson, Jonathan W. Goldman, Edward B. Garon, Jay M. Lee, Carol Felix, Minsong Cao, Stephen E. Tenn, Daniel A. Low, Patrick A. Kupelian, Michael L. Steinberg, Percy Lee.
Figure 1. Trial Flow Diagram: 28 Patients with locally advanced, stage II-III NSCLC enrolled after confirming eligibility. 28 Underwent FDG-PET/CT and 4DCT simulation and were treated to 4 Gy x 10 fractions; after the eighth or ninth fraction, restaging 4DCT simulation with or without FDG-PET/CT was obtained. 10 Received 5 Gy x 5 fractions boost; 9 Received 6 Gy x 5 fractions boost; 9 Received 7 Gy x 5 fractions boost.
@PercyLeeMD
[Slide B] Dose-Intensified Chemoradiation + SABR Boost: Early Signal
- Early-phase, single-institution trial
- Clinical stage II (inoperable/patient refusal of surgery) or III NSCLC (AJCC 7th)
- First received 4 Gy x 10 fractions -> adaptive SABR boost to residual metabolically active disease, consisting of an additional (with concurrent weekly carboplatin/paclitaxel): Low (n=10): 25 Gy (5 Gy x 5 fractions) vs Intermediate (n=9): 30 Gy (6 Gy x 5 fractions) vs High (n=9): 35 Gy (7 Gy x 5 fractions)
- Overall survival (P=.07), Local control (P=.36), Progression-free survival (P=.48) by RT boost cohort (Low/Int/High)
- Protocol-specified MTD was not exceeded
- Non-hematologic acute & late (>90 days) G3 +AE: 11% & 7%
- No G3 toxic effects in intermediate-dose boost
Wu TC and Lee, P, et al. JAMA Oncol. 2024;10(3):352-359. @PercyLeeMD
———
[Slide 3]
[Slide A] Moving the SBRT Boost Before Chemoradiation
- A Phase II Trial of Primary Tumor SBRT Boost Prior to Concurrent Chemoradiation for Locally-Advanced Non-Small Cell Lung Cancer
- 21 patients (median pre-treatment primary tumor size 5.0 cm [range 1.0-8.3]) received an SBRT boost in 2 fractions (central 12 Gy, peripheral 16 Gy) to the primary tumor, followed by standard CRT (60/2 Gy)
- Toxicity: Grade >=3: esophagitis (14.3%), lung infection/pneumonia (14.3%), pneumonitis (9.5%); 1 treatment-related grade 4 non-hematologic toxicity (respiratory failure/radiation pneumonitis)
- Outcomes: 2-yr outcomes: primary tumor control 92.3%, DFS 46.1%, OS 50.3%; Median survival 37.8 months
Williams TM, et al. Int J Radiat Oncol Biol Phys. 2024;120(3):681-694.
[Slide B] Phase II: Full Dose SBRT in Combination with Mediastinal Chemoradiation - Treatment Guide to Phase III LU-008
- Phase II multisite, single-arm trial. 60 pts: Stage II-III NSCLC. SBRT to primary tumor 50 Gy/12.5 Gy, 54 Gy/18 Gy, 50 Gy/10 Gy; Mediastinal chemoradiation Carboplatin/Paclitaxel or Cisplatin/Etoposide 60 Gy/2.0 Gy +/- Consolidation chemotherapy/adjuvant immunotherapy.
- 1-yr PFS [all pts]: 62.8%; 1-yr PFS [received durvalumab]: 69.6%. Median PFS: 25.3 mo. (95% CI: 11.5, 54.1). Median OS: 47.1 mo.
Patterns of Failure & Toxicities: Any failure within 1 year 22 (36.1%): Distant failure 10 (16.4%), Regional failure 3 (4.9%), Distant + regional failure 1 (1.6%), Death 8 (13.1%). Any failure on study 36 (59.0%): Distant failure 20 (32.8%), Regional failure 3 (4.9%), Distant + regional failure 2 (3.3%), Death 10 (16.4%), Local failure 1 (1.6%). G3+ toxicity related to SBRT and/or mediastinal RT: 13.1%; G3 pneumonitis: 3 pts (5%).
Heinzerling JH, et al. Lancet. 2024; Preprint. @PercyLeeMD
———
[Slide 4]
Phase III NRG Oncology LU008 trial
Population: Locally advanced stage II-III (node positive) NSCLC. Patient Screening -> R -> [SBRT (primary) -> Chemoradiation (mediastinum)] or [Chemoradiation (primary + mediastinum)] -> Maintenance Immunotherapy x 12 months.
Stratification: Stage (II/IIIA vs. IIIB/IIIC); PD-L1 Status.
- Control arm: chemoradiation to the primary and mediastinal disease (60 Gy/2 Gy) -> immunotherapy maintenance x 12 months
- Experimental arm: SBRT to the primary (standard BED >=100 Gy dose regimen) -> chemoradiation to mediastinal disease (60 Gy/2 Gy) -> immunotherapy maintenance x 12 months. SBRT to primary tumor: 3 fractions to 54 Gy (BED10 of 151.2 Gy) [peripheral]; 4 fractions to 50 Gy (BED10 of 112.5 Gy) [peripheral]; 5 fractions to 50 Gy (BED10 of 100 Gy) [peripheral or central]. Radiation to involved hilar/mediastinal lymph nodes: 2 Gy x 30 fx to 60 Gy, IMRT or proton therapy.
Concurrent chemotherapy: carboplatin + paclitaxel, cisplatin + etoposide, cisplatin + pemetrexed, or carboplatin + pemetrexed. Maintenance immunotherapy: durvalumab x 12 months [if durvalumab is NOT given, carbo/paclitaxel pts receive 2 cycles of consolidation].
1. Heinzerling JH, et al. Lancet. 2024; Preprint. 2. Nrgoncology.org. @PercyLeeMD
NBTXR3, an intratumoral hafnium oxide radioenhancer, is in study in NSCLC: Dr. @StevenLin_MDPhD, (@MDAndersonnews) presented Phase I/II re-irradiation study in recurrent disease and Ph II CONVERGE on CRT and durvalumab in Stage III; delivery reported safe. #DAVALung
NANORAY-312
[Slide 1]
Why focus on Hafnium-oxide? Late-stage product in clinical testing in number of disease sites with radiotherapy
- Hafnium Oxide Nanoparticle NBTXR3 has 9x enhancement of radiation dose over subcellular distances
- Only one administration directly injected into tumors before XRT
- Positive phase II/III trial in STS showing doubling of pathologic complete response after preoperative XRT (Lancet 2019) (CE marked in 2019 in EU (Hensify(TM))
(Diagram: Radiotherapy vs Radiotherapy with NBTXR3; 9X Dose around nanoparticles; Clusters of Nanoparticles; Local absorption of energy; Hf Hafnium 72, 178.49)
NANOBIOTIX EXPANDING LIFE; JANSSEN Pharmaceutical Companies of Johnson & Johnson; UT MD Anderson
———
[Slide 2]
Trials in Progress combining NBTXR3 with RT/CRT
Patients (Current Study) | N | Phase | Operational Sponsor:
Head & Neck — Elderly Cisplatin-ineligible (NANORAY-312, RT-R3 +/- cetuximab vs RT +/- cetuximab) | 500 | Nanobiotix/Janssen*; R/M IO Naive (Study 1100, RT-R3 fb anti-PD-1) | 35+ | Nanobiotix; R/M IO Resistant (Study 1100, RT-R3 fb anti-PD-1) | 35+ | Nanobiotix; R/M (MDA-0541, RT-R3 fb anti-PD-1) | 60 | MD Anderson Cancer Center
Lung — Inoperable, Stage 3 | NA | Janssen; Inoperable, Recurrent (MDA-0123, Reirradiation RT-R3) | 24 | MD Anderson Cancer Center
Other early trials: LAPC (MDACC) (Koay); Esophagus (MDACC) (Lin); Advanced Lung (MDACC, Gandhi, Welsh)
Hypothesis: 1) Inoperable, radiorecurrent NSCLC: could NBTXR3 provide better tumor control with reirradiation? 2) Inoperable, treatment naive LA-NSCLC: could NBTXR3 enhance cures with CRT+durvalumab?
UT MD Anderson
---
Phase I/II study of re-irradiation with intratumoral injection of NBTXR3 for unresectable locoregionally recurrent non-small cell lung cancer
N = 24; PI: Saumil Gandhi, MD, PhD
(Study schema: Simulation, Verification Simulation, Nanoparticle injection D1, IMRT 45 Gy 15 fx or 30 Gy in 10 fx D15-D43, Safety assessment EOT D85, Efficacy assessment, End of Trial, Progression; Q3M for 1 yr after RT, Q3M for 2 yrs, Q6M until progression)
MDA - Nanobiotix Strategic Alliance IIT; UT MD Anderson
———
[Slide 3]
Study Objectives
Primary: Determine whether re-irradiating lung tumors after intratumoral/intralesional injection of NBTXR3 is feasible with acceptable rates of toxicity.
Secondary: 1-year Local disease control rate; Time to distant metastasis; 1- and 2-year PFS and OS
Tissue and blood correlatives: Explore markers of response to NBTXR3 activated by radiation therapy; Determine immunomodulatory effects of NBTXR3 activated by radiation therapy; Tissue: PD1 expression, CD4/CD8 TCR diversity, tumor immune microenvironment profile; Blood: cfDNA, immune cell activation
UT MD Anderson
---
Phase I results in 12 pts (dose escalation 22% to 33%)
No DLTs, all patients completed therapy (30 Gy - 45 Gy in 10/15 fx)
Table 1: Patient Characteristics — Patient Number, Age years, Sex, reRT Interval years, Prior RT Fractionation, Prior RT Dose Gy/Fractions, reRT Dose Gy, GTV mL, GTV Coverage (V45Gy %), PTV mL, PTV Coverage (V45Gy %) for 12 patients (e.g. Pt1 70 Female 1.6 CFRT 50/25 45 6 65% 31 28%; Pt5 76 Female 2.4 SBRT 50/5 45 157 100% 522 100%; etc.)
reRT: Re-irradiation, CFRT: Conventionally Fractionated Radiotherapy, SBRT: Stereotactic Body Radiotherapy, GTV: Gross Tumor Volume, PTV: Planning Target Volume; V45Gy: Percent volume receiving at least 45 Gy; Under review
———
[Slide 4]
Part 1: Sequential Procedure Optimization Run-in Cohorts
Cohort A: Eligibility -> N= up to 5 -> JNJ-90301900 injected at dose level of 22% -> Concurrent CRT (cCRT) -> If no evidence of PD -> Consolidation Durvalumab (cIT) -> Follow-up; Cohort A evaluation: 24-hour post injection confirmation CT
Cohort B: Eligibility -> N= up to 5 -> JNJ-90301900 injected at dose level of 33% -> Concurrent CRT (cCRT) -> If no evidence of PD -> Consolidation Durvalumab (cIT) -> Follow-up; Cohort B evaluation: 24-hour post injection confirmation CT
J&J; Concurrent CRT = 60/2 Gy IMRT + Carboplatin/Paclitaxel qwk x6; INTERVENTIONAL ONCOLOGY 5; UT MD Anderson
---
Early results in 7 patients reported at ESTRO 2026
- Overall response rate 85.7% (6 of 7 patients) after full regimen
- Complete response rate 57.1% (4 of 7 patients) reported
- Disease control rate 100% (7 of 7 patients) observed
- Intratumoral/intranodal JNJ-1900 administration reported as feasible and safely performed
- Responses described as deepening over time, suggesting potential durability
- Current accrual = 48
Dr. Jun Zhang (@HoustonMethodist) reviews the evidence for Tumor Treating Fields in mesothelioma (STELLAR) and NSCLC (LUNAR, METIS) plus practical tips for managing TTFields-related skin reactions. #DAVALung
SF SBRT in practice: Dr. Gregory Videtic (@ClevelandClinic) reviews RTOG 0915, RPCI I 124407, ASTRO 2025 utilization data, and CCF 2025 1000+ pt analysis supporting SF SBRT, while its overall utilization remains strikingly low. #DAVALung
[Slide 1]
SBRT as standard of care for medically inoperable lung cancer
SBRT Evolution
Early 2000s Milestone - RTOG 0236
- First Lung SBRT North American prospective cooperative group trial
- Purpose: Phase II multicenter study of medically inoperable patients with biopsy-proven peripheral T1-T2N0M0 non-small cell tumors (measuring <5 cm in diameter)
- Methods: SBRT prescription dose was 20 Gy (18 Gy hetero-corrected) per fraction x 3 fractions 60 Gy total (54 Gy heterogeneity-corrected)
- Primary endpoint was 2-year local control
- 3-year Primary Tumor Control rate 97.6%
- 3-year rate of Distant Failure 22.1%
- 3-year Overall Survival 55.8% (Median 48.1 months)
- Grade 3 AEs were reported in 7 pts. (12.7%); grade 4 in 2 pts. (3.6%). No grade 5. Rib fractures and dermatitis have been observed especially for chest wall tumors
———
[Slide 2]
RTOG 0915- rPh II of 1-fraction vs. 4-fraction lung SBRT
RTOG 0915 (NCCTG N0927): A Randomized Phase II Study Comparing 2 Stereotactic Body Radiation Therapy (SBRT) Schedules for Medically Inoperable Patients with Stage I Peripheral Non-Small Cell Lung Cancer
Gregory Videtic, Chen Hu, Anurag Singh, Joe Y. Chang, William Parker, Kenneth Olivier, Steven E. Schild, Ritsuko Komaki, James Urbanic, Hak Choy
- 34 Gy/1 fx vs. 48 Gy/4 fx
- At 1 year, 34 Gy/fx "winner" when compared to 48 Gy/4 fx because: Lower absolute >grade 3 toxicity rate; Equal local control
Long-term Follow-up on NRG Oncology RTOG 0915 (NCCTG N0927): International Journal of Radiation Oncology*Biology*Physics, Volume 103, issue 5, 1 April 2019, Pages 1077-1084
- No excess in late-appearing toxicity was seen in either arm.
- Primary tumor control rates at 5 yrs. were similar by arm.
- Median survivals of 4 yrs. for each arm suggest similar efficacy between the two fractionation schedules, pending any larger studies appropriately powered to detect survival differences.
———
[Slide 3]
RPCI I 124407: rPh II of 1-fraction vs. 3-fraction lung SBRT
One Versus Three Fractions of Stereotactic Body Radiation Therapy for Peripheral Stage I to II Non-Small Cell Lung Cancer: A Randomized, Multi-Institution, Phase 2 Trial
Anurag K. Singh, MD; Jorge A. Gomez-Suescun, MD; Kevin L. Stephans, MD; Jeffrey A. Bogart, MD; Gregory M. Hermann, MD, MPH; Lili Tian, PhD; Adrienne Groman, MS; and Gregory M. Videtic, MD
Received Jun 6, 2019. Accepted for publication Aug 5, 2019.
- Demonstrate 30 Gy in 1 fraction equivalent to 60 Gy in 3 fractions in terms of toxicity and PFS [and OS].
- Single fraction SBRT is a valid regimen
———
[Slide 4]
The Real World and the Utilization of SF SBRT
- ASTRO 2025
- Fifteen-Year Trends in Single-Fraction SBRT Utilization for Stage I Non-Small Cell Lung Cancer- Moghanaki et al.
- There have been 2 randomized phase II trials in lung SBRT comparing One vs. Fractionated Rxs.
- Identify patients with stage I NSCLC treated with SBRT from 2006 to 2021 with either a SF or multi-fraction (MF) prescription.
- The proportion of facilities delivering SF significantly increased over time, from 0% in 2006 to 11% in 2021 (p<0.0001), with a greater increase observed at higher-volume centers and academic facilities
- Despite the increased overall utilization, the proportion of lung SBRT treatments delivered as SF remained low, increasing from 0% to only 1.6% over the study period (p<0.0001)!!
- Conclusion: Although the use of SF SBRT for stage I NSCLC has been gradually increasing, particularly at high-volume academic centers, its overall utilization remains strikingly low.
CCF 2025 Retrospective Analysis of SF SBRT vs. MF SBRT- 1000+ pts.
IASLC 2025 World Conference on Lung Cancer, September 6-9, 2025, Barcelona, Spain #WCLC25
"Simply the Best": Analysis of 1000+ Patients Comparing Single-Fraction to Three-Fraction Lung SBRT for Early-Stage Inoperable Lung Cancer. Gregory M. M. Videtic, MDCM; Taussig Cancer Institute, Cleveland Clinic, Cleveland, OH, USA
Conclusions: In this analysis of over 1000 pts treated in a single institution, there were no differences seen in OS between SF and TF lung SBRT pts. Rates of high-grade toxicity (including of the chest wall) were similar between Fx schedules, as were LF and DF rates. These results suggests that SF may be the preferred lung SBRT option for ES-LC, potentially offering logistical and resource advantages.
Stage III NSCLC strategy check: Everett E. Vokes (@eevokes, @UChicagoMed) maps the road from PACIFIC durvalumab to COAST, ROSETTA, PACIFIC-2, EA5181, APOLO and InTRist as IO moves earlier. #DAVALung
[Slide 1]
ROSETTA Lung-201
Randomized, Multicenter, Open-label, Phase 3 study to Evaluate Pumitamig Versus Durvalumab Following Concurrent Chemoradiation Patients With Unresectable Stage III NSCLC
Key Eligibility Criteria:
- Locally Advanced, unresectable Stage III (A,B,C) NSCLC
- Must have received at least 2 cycles of CCRT
- No PD after CCRT
- No other therapy given for locally advanced disease
- No prior anti-PD1/PD-L1
- ECOG 0-1
- No documented EGFR mutations or ALK rearrangements
N=850, R 1:1 (Randomization within 14 to 42 days after completion of CCRT)
Arm A: Pumitamig 1500 mg Q3W (BM ≥50 kg) / 1200 mg Q3W (BW<50 kg)
Arm B: Durvalumab 1500 mg Q4W
Treatment until Disease Progression (BICR confirmed), Unacceptable toxicity, or Consent withdrawal, or for a maximum duration of treatment of 12 months
Stratification Factors: Disease Stage (IIIA vs B vs C); Histology (Sq vs Non-Sq); PD-L1 (<1%, ≥1%, NE)
Primary endpoint: PFS (RECIST 1.1) by BICR
Key Secondary endpoint: OS
NCT07361497
———
[Slide 2]
ECOG-ACRIN EA5181: Phase 3 Trial of Concurrent and Consolidative Durvalumab vs Consolidation Durvalumab Alone for Unresectable Stage III NSCLC
EA5181: Overall Survival - HR = 1.03 (95% CI: 0.80-1.32)
ChemoRT-IO: 38.5% participants with events; Median OS 41.5 (34.4, NR)
ChemoRT: 38.2% events; Median OS 38.4
EA5181: Progression-free Survival - HR = 1.05 (95% CI: 0.86-1.29)
ChemoRT-IO: 66% participants with events; Median PFS 15.3 (13.8-20.0)
ChemoRT: 68.4% events; Median PFS 14.8 (12.0-20.1)
Varlotto JM et al, WCLC, 2025
———
[Slide 3]
Current Opportunities (Key Questions)
- Has PACIFIC been validated (yes, GEMSTONE, Real World)
- Should PD-L1 negative patients receive consolidation (likely not)
- Further Incorporation of novel agents and which segment
- During Consolidation (Coast, Pacific-9, Rosetta-201) (Skyscraper-03, 73L, Bintrafusp were negative)
- Addition of concurrent IO (STAY AWAY)
- Stage III Neoadjuvant CT-IO (AFT-16, APOLO)
- Potential SBRT to primary (NRG LU-08)
- Duration of consolidation (ctDNA)
———
[Slide 4]
Simultaneous Durvalumab and Platinum-Based Chemoradiotherapy in Unresectable Stage III NSCLC: The Phase III PACIFIC-2 Study
Study Population: Patients with unresectable, Stage III NSCLC; All-comers (PD-L1 expression-agnostic); ECOG PS 0-1
Randomised N=300 patients (2:1)
Arm: Durvalumab 1500 mg Q4W + CRT (n=300) -> Durvalumab 1500 mg Q4W
Arm: Placebo + CRT -> Placebo
Stratification: Age (<65, ≥65); Stage (IIIA vs IIIB/C)
Primary Endpoints: ORR, PFS; Key Secondary Endpoints: OS, OS24; Treat to progression
Study Chair: Bradley
Figures A (PFS) and B (OS): Durvalumab + CRT vs Placebo + CRT
Bradley JD et al, J Clin Oncol, 43(33):3610-3621, 2025
Precision radiation, sharper targeting. @PercyLeeMD, @cityofhope reviews MR-guided SBRT for central lung tumors, with adaptive planning, smaller PTVs, and 40% lower PTV volume (20.8 vs 34.1 cc). #DAVALung
[Slide 1]
Ongoing trials for MR guided RT for Lung
Table 2. Ongoing trials of magnetic resonance imaging-guided radiation therapy in treatment of lung tumors. Columns: NCT Number (Registration Year), Study Type, RT Regimen, Combined Therapy, Trial Design (Aim), Primary Outcomes, Notes. Multiple prospective and Phase 1/2 trials listed (NCT numbers, MRgRT regimens, SBRT/SABR, chemoradiation, primary outcomes including MRI dose escalation feasibility, toxicity, local control). Table continues (Cont.) with additional NCT-registered trials. City of Hope.
———
[Slide 2]
Magnetic resonance guided RT (MRgRT)
- MRgRT has several advantages that increase the therapeutic ratio
- Improved tumor / normal tissue visualization
- Daily online adaptive therapy
- Continuous, real-time imaging during radiation delivery
- Most beneficial to tumors adjacent to multiple OARs (i.e. central tumors)
(Results by year chart 1999-2024; MR images of central lung tumor with isodose lines) @PercyLeeMD
———
[Slide 3]
THE PURSUIT OF MOTION MANAGEMENT
Timeline: Varian RPM System 1999; Calypso RF Fiducials 2006; BrainLab ExacTrac 2006; ViewRay 4 FPS 2012; Accuray Synchrony 2013; Surface Guidance Vision RT 2013; Elekta/Aktina ABC 2015; ViewRay 8 FPS 2020.
Synchrony is a registered trademark of Accuray. ExacTrac is a registered trademark of Brainlab. Calypso is a registered trademark and RPM is a registered trademark of Varian. ABC is a trademark of Elekta.
———
[Slide 4]
MR-guided Single Fraction Lung SABR
Tekatli et al, Radiotherapy and Oncology 2023:
- SF-SABR with BH (often same day)
- 50 patients, 69% with primary NSCLC
- Median PTV 11.2 mL
- 80% GTV within 2.5 cm from chest wall
- 34 Gy/1, 30 Gy/1, or 20-28Gy/1
- 2-year OS 82%, 3-year LC 97%
- 1 patient with grade 3+ CW pain
Chuong et al, SMART One, IJROBP 2025:
- 1-year LC 96.2%, OS 86.3%, 1 acute grade 3 AE, no late grade 3-5 AE
Theme · 32 talks
IO Combinations, Perioperative, Surgery & Screening
Screening nonsmokers with family history: Dr. Jamie Chaft (@MSKCancerCenter) reviews LUNG-CARE and TALENT data, the adenocarcinoma in situ question, and Sybil AI via LEGACY trial, and concluded that there is no role for early screening in the US today. #DAVALung
LUNG-CARETALENT
[Slide 1]
[Slide A] Overall survival among screen-detected and non-screen-detected lung cancer cases
Strata: Screening vs Non-Screening. HR 0.13 (95% CI 0.09-0.19), p < 0.001.
Screen-detected cases had markedly better survival, with 87% 5-year OS versus 39% in non-screened patients (HR 0.13, P<0.001).
Number at risk: Screening 227, 220, 214, 208, 206, 193, 167, 132; Non-Screening 1105, 717, 584, 518, 379, 223, 119, 38.
Caichen Li, Wenhua Liang et al. Slides adapted from discussion by Prof Joachim Aerts, ELCC 2026.
[Slide B] Cumulative lung cancer-specific mortality, and stratified by sex
Overall: HR 0.45, 95% CI 0.32-0.65, P < 0.001. Males: HR 0.55, 95% CI 0.36-0.83, P = 0.004. Females: HR 0.28, 95% CI 0.13-0.60, P < 0.001.
LDCT screening was associated with substantial mortality reduction overall (HR 0.45), with a notably greater benefit observed in women (72% risk reduction) compared with men (45% risk reduction).
———
[Slide 2]
[Slide A] Is this lung cancer that kills patients / Adenocarcinoma in situ?
Stage and Histologic Type: Non-screening group (n=1,105) vs Screening group (n=227), number/total number (percent)
Stage: 0: 8/1,105 (0.7) vs 8/227 (3.5); I: 277/1,105 (25.1) vs 185/227 (81.5); II: 50/1,105 (4.5) vs 3/227 (1.3); III: 199/1,105 (18.0) vs 14/227 (6.2); IV: 571/1,105 (51.7) vs 17/227 (7.5).
Histologic type: Adenocarcinoma: 799/1,105 (72.3) vs 212/227 (93.4); Squamous-cell carcinoma: 129/1,105 (11.7) vs 6/227 (2.6); Large-cell carcinoma: 7/1,105 (0.6) vs 0/227 (0.0); Small-cell carcinoma: 65/1,105 (5.9) vs 1/227 (0.4); Carcinoid: 2/1,105 (0.2) vs 0/227 (0.0); Lymphoepithelioma-like carcinoma: 10/1,105 (0.9) vs 0/227 (0.0); Unknown: 93/1,105 (8.4) vs 8/227 (3.5).
[Slide B] Comparisons of different screening trials
LUNG-CARE Project | TALENT | FANSS | NLST
N: 11,708 | 12,011 | 1,000 | 26,722
Screened population: LUNG-CARE General population aged 40-74 years (non-risk-based); TALENT Asian individuals aged 55-75 years who have never smoked, with additional risk factors; FANSS Asian women aged 40-74 years who have never smoked; NLST Individuals aged 55-74 years with >=30 pack-years smoking history, and if former smokers, quit within the previous 15 years.
Baseline lung cancer detection rate: LUNG-CARE 1.9% (includes in situ and minimally invasive), 1.4% (invasive adenocarcinoma only); TALENT 2.6% (includes in situ and minimally invasive), 1.5% (invasive adenocarcinoma only); FANSS 1.3%; NLST 1.1%.
Chang GC, et al. Lancet Respir Med. 2024 Feb;12(2) 141-152. Shum E, et al. WCLC. 2025 Oct. Aberle D, et al, N Engl J Med. 2011 Aug 4;365(5):395-409.
———
[Slide 3]
Having a family history of lung cancer significantly increases lung cancer risk
[Left] Dose-dependent relationship between # first-degree relatives and LC Risk. Invasive lung cancer detection rate (%) by number of first-degree relatives: 1.6%, 2.5% (p<0.001), 3.7% (p<0.001), 7.2% (p=0.001). Chang et al., Lancet Resp Med 2024.
[Right] With >1 first- and/or second-degree relatives, lung cancer risk is comparable to that in the National Lung Screening Trial. Cumulative detection rate over years since first LDCT: Multiplex, NLST, Simplex. 43/50 (86%) invasive carcinomas. Wang et al., JTO 2023; Aberle et al., JTO 2020.
———
[Slide 4]
[Slide A - WCLC25] Sybil is an AI model that can measure future lung cancer risk based on a CT Chest
Model maps CT Chest to risk score over Time (years) for future lung cancer vs no future lung cancer.
Key advantages: No image annotation required; No clinical input needed; Instant readouts; Open source.
Mikhael et al, J Clin Oncol 2023
[Slide B - WCLC25] LEGACY: A large, prospective trial to validate Sybil in individuals with a lung cancer family history
Individuals with a lung cancer family history: >=1 first-degree relative OR >=2 second-degree relatives. Getting a CT Chest scan (Boston), can also provide images from prior scans, OR provide images from prior CT Chest scan(s). Database containing: 1. CT Chest scan images; 2. Clinical information (medical history, family history, exposures); 3. Longitudinal cancer outcomes. Analyze all scans with Sybil.
Goal enrollment: >=2500 participants. Global, remote enrollment permitted! NCT07600801. PI: Allison Chang.
TNM has evolved from 3,753 pts in 1986 to IASLC datasets of 76k+ in the 9th edition. James Huang, MD (@MSKCancerCenter) asks whether biomarkers/ctDNA should enter the next staging framework. #DAVALung
[Slide 1]
The Purpose and Value of TNM.
- TNM is descriptive: Defines anatomic extent of disease.
- TNM is prognostic: Up to a point.
- Other factors may help refine prognostic discrimination or augment it.
———
[Slide 2]
IASLC Era - TNM Staging.
7th Edition (2007): 67,725 pts.
8th Edition (2015): 94,708 pts.
9th Edition (2024): 76,518 pts.
———
[Slide 3]
ctDNA.
B Longitudinal setting: PFS vs Time (months). ctDNA negative vs ctDNA positive. p=0.0001. Number at risk: ctDNA negative 8, 7, 3, 0; ctDNA positive 9, 1, 0, 0.
Lebow, Front Oncol, 2023.
Right panel: MRD tracking schematic — Primary tumor development, Adjuvant chemotherapy, MRD-neg but residual disease, Relapse, Microscopic disease on scan, MRD detection space, Tumor burden better (ctDNA LOD). PATIENT 1, PATIENT 2.
Abbosh, Trends in Cancer 2024.
———
[Slide 4]
How Exactly Should We Revise TNM?
- TNM-B
- (B)iomarker or (B)lood
- T: T1-T4
- N: N0-N3
- M: M0-M1
- B: B1,B2,B3?
I had a terrific time at #DAVALung learning from some of the brightest minds in thoracic oncology and connecting with collaborators old and new. Thanks to Dr. Jain and @DAVAOnc for including me in this wonderful event!
Access to specialty palliative care remains an important focus in advanced lung cancer. Fionnuala Crowley, MD (@FionnualaCrowle@TischCancer@SinaiHemeOnc) reviews evolving models of specialty palliative care, including early integration, telehealth approaches, evidence-based
[Slide 1]
Addressing supply vs demand issue
Quality of life (FACT-L score) box plots at weeks 0, 12, 24 after randomization.
Stepped Specialty Palliative Care: No. of patients - Stepped palliative care 250, 171, 146; Early integrated palliative care 256, 178, 145.
Telehealth Specialty Palliative Care (Video visits vs In-person visits): No. of patients - Video visits 618, 395, 311; In-person visits 606, 398, 319.
Temel et al 2024, JAMA; Greer et al, JAMA 2024.
———
[Slide 2]
Primary versus Specialty Palliative Care in Oncology
Primary palliative care (Delivered by primary oncology team): Symptom assessment and management; Prognostic communication; Advance care planning; Goals of care discussions; Emotional and psychological support.
Specialty palliative care (Delivered by specialty palliative care team): Management of refractory symptoms; Complex family/caregiver situations; Hospice and care transition planning; Ethical conflicts and difficult decisions; Complex psychosocial care.
Primary palliative care Advantages: Scales across clinical settings; Builds on existing patient-clinician relationships; Enables early and continuous integration; Supports quality of life as a core goal; Preserves specialist resources; Extends care to resource-limited settings; Reduces patient burden (time toxicity).
Specialty palliative care Advantages: Expert management of complex symptoms and distress; Interdisciplinary team-based care; Dedicated time for in-depth discussions; Independent focus on quality of life; Support for complex family dynamics and decision making.
Crowley et al, JCO 2026.
———
[Slide 3]
Physical Supportive Care Needs of Patients with Lung Cancer (Symptom / First Line treatment)
Nociceptive Cancer Pain: Opioids - No organ dysfunction: Morphine; Kidney/Liver dysfunction: Fentanyl/methadone preferred; Hydromorphone, oxycodone with caution. Adjuvants: Tylenol, NSAIDS.
Neuropathic pain: Chemo-related - Duloxetine; Non-chemo related - Pregabalin (insurance usually requires gabapentin having been tried); Integrative: Acupuncture, scrambler therapy.
Cough: Opioids - Hycodan; Non-opioid - Dextromethorphan, benzonatate.
SOB: Low dose opioids.
Nausea: HEC: Carboplatin AUC >4, Cisplatin, DatoDx, Enhertu - 4 agent antiemetics; Refractory: Olanzapine.
Reduced Appetite/Anorexia: Olanzapine 2.5mg; Mirtazapine only in depression; Steroids end of life.
———
[Slide 4]
The secret sauce of SPC- Coping
Increased patient use of approach-oriented coping strategies (B = 1.09; SE = 0.44; P = .01) and slightly reduced use of avoidant strategies (B = -0.44; SE = 0.23; P = .06) from baseline to 24 weeks.
Increased use of approach-oriented coping and reduction in avoidant coping were associated with higher QOL and lower depressive symptoms at 24 weeks.
Greer et al, Journal of Clinical Oncology, 2018.
Dr. @eevokes@UChicago highlights the evolution of head & neck cancer care: from stigma and functional morbidity to multidisciplinary, patient-centered treatment. Tobacco + alcohol remain a dominant classic exposure pattern in HNC, with synergistic effects. #DAVALung
NRG-005OPTIMA
[Slide 1]
HNC Patients are particularly vulnerable
- Visible and functional changes: scars, facial asymmetry, altered voice/speech, drooling, dental loss, eating in public.
- Etiology stereotypes:
- Association with Tobacco and alcohol can invite blame.
- HPV-associated oropharyngeal cancer can prompt sexual-behavior judgments and relationship stress (proper counseling needed).
- Cultural context: norms around appearance, speech, sexuality, and "personal responsibility" shape stigma by region and community.
- Lower treatment adherence and care fragmentation; esp in LMICs.
- Delayed help-seeking and screening (fear of blame, appearance concerns).
- Worse psychosocial outcomes: depression, anxiety, social isolation, body-image dissatisfaction.
- Work discrimination and job loss in survivorship.
———
[Slide 2]
Head and Neck Cancer Risk Factors
Rank | Risk factor | Approximate risk increase | Main relevance / comments | Key reference
1 | Combined tobacco + alcohol use | OR 20-30. Together they account for about 72% of HNC cases and have a synergistic combined effect | The dominant classic exposure pattern; especially important for OC, hypopharynx, and larynx cancers | nature.com pmc.ncbi.nlm.nih.gov
2 | Tobacco smoking | OR about 2.1 to 2.6 overall; higher for some subsites such as larynx, oropharynx (about 3.7) and oral cavity (about 2.5) | One of the strongest independent risk factors; particularly important for laryngeal cancer | nature.com pmc.ncbi.nlm.nih.gov
3 | HPV infection, especially HPV16 | Currently 60-70% of US/European oropharyngeal cancer are HPV-related; complex carcinogenesis | A major driver of oropharyngeal cancer, but not the cause of most non-oropharyngeal HNSCC | pubmed.ncbi.nlm.nih.gov nature.com nih.gov
4 | Heavy alcohol consumption | OR about 3.76 for heavy alcohol use in HPV-negative oropharyngeal cancer | Strong independent risk factor, especially for oral cavity and oropharyngeal cancer; often combined with smoking | pmc.ncbi.nlm.nih.gov nature.com
5 | Betel quid / areca nut chewing | Strong increase, but no single robust pooled OR number | Especially important in South and Southeast Asia; strongly linked to oral cavity cancer (buccal) | nature.com
6 | Smokeless tobacco | Increased risk, but no single stable pooled estimate in the reviewed source | Likely relevant to oral cavity cancer
7 | Poor oral hygiene / poor oral health | Modest increase relative to tobacco, alcohol, and HPV | Likely contributes, but effect size is smaller and more confounded | nature.com
8 | Low fruit / vegetable intake and other dietary factors | Modest increase; no single reliable pooled effect | Secondary compared with the major carcinogenic exposures above | nature.com
(row) Occupational, genetic, hormonal, and socioeconomic factors | Variable and generally less consistently quantified | Usually lower-impact or more context-dependent
———
[Slide 3]
Synergistic Effect of Alcohol Consumption and Tobacco Smoking on Salivary Acetaldehyde Concentration
A. Ethanol ingestion in Smokers (without Concomitant Smoking) and in Nonsmokers — Salivary Acetaldehyde (umol/liter) vs Minutes; Smokers vs Nonsmokers
B. Ethanol ingestion in Smokers (with Concomitant Smoking) and in Nonsmokers — Salivary Acetaldehyde (umol/liter) vs Minutes; Smokers vs Nonsmokers
Gapstur SM et al, N Engl J Med 389(26):2486-2494, 2023
———
[Slide 4]
HPV-positive HNC Research Directions for De-Intensification
- High cure rates suggest that less toxic therapies may be feasible for pt subsets
- Explore surgical options (TORS)
- Use less toxic or no chemotherapy (cetuximab failed)
- Lower XRT doses and reduced field size as single modality or with chemo (60 Gy with weekly cis per NRG-005 failed, Hypoxia-directed for earlier stage)
- Use Induction Chemotherapy to eradicate systemic micrometastases and select patient with most favorable prognosis (ECOG, Optima trials)
- Immunotherapy (no evidence yet outside of surgical setting)
- Include long-term functional outcomes
Targeting the Hippo pathway in mesothelioma! Dr. Sandip Patel (@PatelOncology) presents SW-682, a pan-TEAD inhibitor in Phase 1 trials, aimed at NF2/LATS2-mutated tumors driving TEAD upregulation, a promising new mechanism-based approach. #DAVALung
[Slide 1]
Hippo/YAP Pathway
(Pathway schematic showing KIBRA, NF2, SAV1, MST1/2, DLG5, TAO, STRIPAK, MOB1A/B, LATS1/2, MAPK4, STRN4, RAP2, YAP/TAZ, 14-3-3, TEAD1-4, ILK, FAK, Src, Rho GTPases, Acto-myosin; Inhibitors of YAP/TAZ expression (IK0N537); Inhibitors of YAP/TAZ-TEAD interaction (IAG933); Inhibitors of TEAD palmitoylation (VT3989/IK-930).)
Hippo Pathway Active = YAP Inactive; Hippo Pathway Inactive = YAP Active (leading to tumor growth).
- Genomic alterations in the Hippo signaling pathway occur in approximately 10% of cancers, leading to constitutive activation of transcriptional co-activators, YAP1/TAZ.
- YAP/TAZ binds to the transcription factor TEAD, resulting in expression of target genes involved in cell proliferation and tumor progression.
- SW-682 is an investigational, small molecule pan-TEAD inhibitor that blocks TEAD-dependent transcription by binding to the palmitoylation pocket of all TEAD isoforms.
- In Hippo-mutant mesothelioma models, SW-682 downregulates transcription of YAP/TAZ target genes, inhibits proliferation in vitro and results in tumor regression in vivo.
Source: Papavassiliou JCMM 2024. Slide 266
———
[Slide 2]
SW-682 is a pan-TEAD inhibitor
- MW < 400
- TPSA < 90
- Pan-TEAD binder
- hERG blockade IC50 > 10 uM
- No CYP IC50 < 10 uM (7 isoforms)
- Binding mode confirmed by high-resolution co-crystal structure (TEAD1)
SW-682 demonstrates robust anti-tumor activity in mesothelioma xenograft models in vivo: MSTO-211H (LATS1/2-del), H226 (NF2-del), H2052 xenografts (Mean Tumor Volume and Best Response in % Tumor Volume from Baseline).
Source: Chen et al AACR 2023. Slide 267
BNT116 targets six tumor-associated antigens frequently expressed in NSCLC and is being evaluated as monotherapy and in combination regimens. Zhonglin Hao, MD, PhD (@UKMarkey) reviews Phase I combination data with docetaxel (ORR 30%, DCR 85%) and the ongoing LuCa-Merit-1 study.
BNT116LuCa-MERIT-1
[Slide 2]
Components of BNT116 are abundant expressed in NSCLC
Six BNT116 TAAs (targets): KK-LC-1, MAGE-A3, PRAME, MAGE-A4, CLDN6, MAGE-C1.
Figure 2: In silico analysis of transcript abundance of the six BNT116 TAAs in an NSCLC cohort. TCGA RNA-Seq data derived from NSCLC specimens (n=881) analyzed for gene expression using the STAR RNA-Seq aligner. (Non-small cell lung cancer TCGA RNA-Seq in rpkm values, n=881.)
Figure 3: In-house assessment of expression of the six BNT116 TAAs, MAGE-A3, CLDN6, KK-LC-1, PRAME, MAGE-A4, and MAGE-C1 in a cohort from clinical routine using RT-qPCR (n=184). (Non-small cell lung cancer BioNTech RT-qPCR data pos/neg by cut-off, n=184.)
red = TAA expression detected, white = TAA expression not detected.
Abbreviations: CLDN6 = claudin-6; KK-LC-1 = kita-kyushu lung cancer antigen 1; MAGE-A3 = melanoma-associated antigen A3; MAGE-A4 = melanoma-associated antigen A4; MAGE-C1 = melanoma-associated antigen C1; PRAME = preferentially expressed antigen on melanomas; RT-qPCR = real-time quantitative polymerase chain reaction; TAA = tumor-associated antigen.
———
[Slide 3]
FIH Combining BNT116 and Docetaxel in NSCLC
Preliminary Results of BNT116 Show Encouraging Antitumor Activity and Manageable Safety Profile in Combination with Docetaxel.
Phase 1 FIH study (NCT05142189): Clinical activity and tolerability. Oven BB. et al. Presented at AACR 2024. #CT051.
Cohort 3: BNT116 + docetaxel (n=20): ORR, n (%) = 6 (30); DCR, n (%) = 17 (85); mPFS, n = 4.4.
BNT116 + docetaxel shows activity in heavily pretreated patients with NSCLC.
Safety: Manageable safety profile, comparable to other FixVac candidates. No signs of the combination treatment increasing the severity or duration of the adverse events were observed.
Historical efficacy of docetaxel monotherapy (Caron et al. Lancet, 2014): ORR <10%; mPFS ~3 months; mOS >9 months.
FIH = first in human; ORR = objective response rate; DCR = disease control rate; mPFS = median progression free survival; mOS = median overall survival; PR = partial response; SD = stable disease; PD = progressive disease; NSCLC = non-small cell lung cancer.
———
[Slide 4]
LuCa-Merit-1
BNT116: Broad Evaluation in NSCLC as Monotherapy and in Combination
LuCa-MERIT-1: FIH, Open Label Phase I Trial Evaluating Safety, Tolerability, and Preliminary Efficacy of BNT116 Alone and in Combinations in NSCLC (NCT05142189). N=130.
Inclusion criteria: Cohort 1-4: Unresectable (Stage III) or metastatic (Stage IV) NSCLC; Cohort 5: Unresectable (Stage III) NSCLC after CRT; Cohort 1, 4 and 6: Resectable (Stage II or III at diagnosis) NSCLC; Cohort 1-5: ECOG PS 0-2; Cohort 2, 3 and 6: ECOG PS <=1.
Arms: BNT116 monotherapy (n=30) Oven D et al. SITC 2023; BNT116 + cemiplimab (n=20) PD-1 <50%, progressive disease on PD-1 or PD-L1 inhibitor as first line Tx; BNT116 + docetaxel (n=20) Oven BB et al. AACR 2024; BNT116 + cemiplimab (n=20) (trial patients); BNT116 + cemiplimab (n=20) (after concurrent CRT); BNT116 + cemiplimab + carboplatin + paclitaxel (nocad, therapy) -> (BNT116+cemiplimab (adjuvant therapy) (n=20)).
Primary Endpoints: DLT occurrence during Cycle 1, safety. Secondary Endpoints: ORR, DoR, DDC, PFS, OS.
EmpowerVax-Lung: Phase 2 Study of Cemiplimab in Combination with BNT116 vs. Cemiplimab Monotherapy in First-Line Treatment of Patients with Advanced NSCLC with PD-L1 >=50% (NCT05557591). N=130. Randomized 1:1. Arm A: Cemiplimab; Arm B: BNT116 + cemiplimab. Up to 24 months or until disease progression. Key inclusion criteria: Advanced untreated NSCLC (Stage IIIB, IIIC or IV) squamous or non-squamous NSCLC who are ineligible for surgical resection or definitive chemoradiation; PD-L1 expression TPS >=50%; at least 1 radiographically measurable lesion by RECIST 1.1; ECOG PS <=1. Primary Endpoint: ORR. Secondary Endpoints: OS, PFS, DOR, TEAEs, SAEs.
C7: BNT316 (Gotistobart); C8: BNT324 (DB-1311 B7H3); C9: BNT326 (YL202 HER3); C10: BNT327 (PD-L1/VEGFA, Pumitamig); C11: BNT327 post chemoradiation now in phase III.
That's a wrap on the 2026 Hawaii Lung Summit! Huge thanks to our brilliant faculty, speakers, and industry partners for making it such an incredible success. Grateful for the science, the connections, and the momentum we're taking forward. #DAVALung
A liquid-biopsy view of metastasis biology: Steven H. Lin (@StevenLin_MDPhD, @UTMDAnderson) explores CAMLs, where large cells (≥50 µm) are prognostic after CRT in stage II-III NSCLC and across cancers. #DAVALung
[Slide 1]
Circulating Giant Cancer Associated Macrophage-Like Cells ("CAMLs")
- Multinucleated giant cells of myeloid lineage (CD14+/CD11c+) and are CD45+, and are variably also CK8, 18, 19, and EpCAM+
- These are only found in cancer patients and not seen in health subjects
Table S1. Summary of healthy subject data, CAML patient data, and CTC patient data separated by stage and therapy type (Disease characteristics / No. of subjects / CAML % / Mean CAML +/- SD / Median CAML / CAML range / CTC % / Mean CTC +/- SD / Median CTC / CTC range). Categories include Healthy normal, Nonmalignant cancer, Stage I-IV, and Treatment (No treatment, Hormone, Chemotherapy). Total patients with malignant cancer: 91% CAML, 62% CTC.
Source: Adams D et al., PNAS 2014
———
[Slide 2]
We found CAMLs to be present in all stages of cancers, with larger CAMLs more predominant in advanced cancers
Cancers (Total n=293): Breast (n=59); Prostate (n=52); Pancreatic (n=52); NSCLC (n=59); RCC (n=37); Esophageal (n=27).
A. Percent of patients positive for CTCs and CAMLs by stage (Normal, Stage I-IV).
B. Number of CAMLs per sample by stage.
C. Average # of CAMLs by size (Normal, Stage I-IV); legend: >100um, 50-100 um, 25-50um.
———
[Slide 3]
Experimental giant hybrid cells with intradermal injected B16F10 increases tumor growth and metastatic potential
Figure panels A-G: B16F10 (H-2Db-RFP-Cre) surgically removed 1-cm tumor; Ai9-GFP; C57Bl/6; RFP/GFP/Merge imaging of Hybrid, Phagocytosis; flow cytometry (0.48% RFP+); Mice with tumor (%); Tumor volume (mm3) over Days; B16F10 vs Hybrid gross tumor and H&E; Metastatic area (% of lung) B16F10 vs Hybrid (*); Primary tumor and Metastatic tumor GFP/MITF imaging.
Source: Gast et al., Sci Adv 2018
———
[Slide 4]
Giant CAMLs are prognostic in stage II-III NSCLC after CRT
KM curves Probability of PFS (%) vs Time from Diagnosis (Months). Legend: <50um CAML (solid red); >=50um CAML (dashed red); Training set (n=54, black).
- Baseline (BL): >=50um CAML associated with worse PFS (curves separate ~50% at 12-18 months; <50um group ~25% PFS at 24 months).
- Follow up time (T1) (First F/U after CRT): >=50um CAML remains prognostic (~75% PFS maintained vs <50um ~25% at 24 months).
Mary Jo Fidler, MD (@maryjofidlerMD@RushMedical) reviews the evolving science of cancer cachexia, highlighting GDF-15 as a therapeutic target and Phase II ponsegromab data in GDF 15-selected patients (40% NSCLC; 90% receiving anticancer therapy), where the 400 mg dose
[Slide 2]
Ponsegromab - humanized subcutaneous monoclonal antibody targeting GDF-15
- Phase II randomized study of 100 mg, 200 mg, or 400 mg or placebo, every 4 weeks for three doses
- 40% NSCLC (plus pancreatic and colorectal) circulating GDF-15 selected patients >= 1500 pg per milliliter
- ECOG <= 3 and a life expectancy of least 4 months
- Primary end point: change from baseline body weight at 12 weeks
- Secondary endpoints: QOL/diary endpoints, physical activity and gait end points with wearable digital health device, CT derived skeletal muscle measurements (exploratory)
Groarke et al NEJM 2024
———
[Slide 3]
Results
Change in Body Weight from Baseline (kg) bar chart, Treatment Policy and On-Treatment groups: Placebo; Ponsegromab 100 mg; Ponsegromab 200 mg; Ponsegromab 400 mg (increasing weight gain with dose; placebo shows weight loss). Approximate 400 mg gain ~2 kg (Treatment Policy) and ~2.6 kg (On-Treatment).
No. of Patients: 45, 46, 46, 50. No. of Patients with Wk-12 Data: 32, 32, 39, 34 (Treatment Policy); 45, 46, 46, 50 / 32, 32, 38, 31 (On-Treatment).
- 90% of patients were receiving cancer treatment with median interval from diagnosis to randomization of 11.7 months
- The effect of 400 mg consistent across cancer type, quartile of serum GDF-15 level, platinum chemotherapy exposure, BMI, and baseline systemic inflammation
- Changes in weight were consistent with GDF-15 suppression at 12 weeks
- Favorable QOL in the 100mg and 400mg dosing and favorable activity for the ~60 patients that met device wearing metrics
Groarke et al NEJM 2024
———
[Slide 4]
Active Cancer Cachexia Therapeutic Studies (Agent / NCT Number / Tumor Inclusion / Primary Endpoint)
- TCMCB07 (MC4R) | NCT06937177 | Newly diagnosed metastatic colorectal cancer undergoing chemotherapy | Maintenance of body weight/muscle mass
- AV-380 (GDF-15) | NCT05865535 | Advanced/metastatic cancers with cachexia and elevated GDF-15 | Safety/tolerability
- Visugromab (GDF-15) + checkpoint blockade + Lenvatinib | NCT07219459 | Hepatocellular carcinoma | Progression-free survival
- Ponsegromab (GDF-15) | NCT06989437 | Metastatic pancreatic cancer | Percent change body weight and Change from baseline in Functional Assessment;
MUC16-targeting bispecific in solid tumors: Dr. @maryjofidlerMD (@RushMedical) presented ubamatamab (REGN4018), a novel MUC16xCD3 bispecific being developed for NSCLC, no added benefit from cemiplimab, and CRS as the main adverse event. #DAVALung
[Slide 1]
Strategies to target MUC16
- MUC16-targeted CAR T cells (eg PRGN-3005, Regeneron 27T51)
- Antibody Drug Conjugate (eg HWK-016)
- As part of a personalized vaccine
- Bispecific antibody
- REGN4018 Ubamatamab
- Binds to the MUC16 proximal membrane region
- MUC16 x CD3
———
[Slide 2]
[Slide A] R4018-ONC-2476 - Study Flow Diagram
Key inclusion criteria: Advanced NSCLC; Prior 1L SOC therapy; Measurable disease; ECOG 0-1; Adequate organ function; Stable/asymptomatic CNS metastases.
Cohort Allocation -> Cohort 1: Anti-PD-(L)1 experienced -> Treatment Allocation: MUC16 IHC -> MUC16 TC >=25% -> R -> Arm 1A: ubamatamab / Arm 1B: ubamatamab + REGN7075; MUC16 TC <25% -> Arm 1C: ubamatamab + REGN7075.
Cohort 2: Anti-PD-(L)1 inexperienced -> Treatment Allocation: MUC16 IHC -> MUC16 TC >=25% -> R -> Arm 2A: ubamatamab / Arm 2B: ubamatamab + REGN7075; MUC16 TC <25% -> Arm 2C: ubamatamab + REGN7075.
[Slide B] Dosing schema of Ubamatmab with or without cemiplimab
- Platinum refractory Ovarian cancer cohort
- 150 patients enrolled
Screening (up to 28 days) -> Cycle 1 (monotherapy lead-in) -> Cycle 2+. Day 1, 8/9, 15, 22, 29, 36. Initial dose (1 mg), Transitional dose (20 mg), Full dose. Monitored setting in all arms (pink star); Monitored setting in Arm C only (purple star). Ubamatamab: Arm A 250 mg IV Q3W; Arm B 800 mg IV Q3W; Arm C 250 mg IV Q3W. Cemiplimab (Arm C only): 350 mg IV Q3W.
Source: Lee JY ESMO 2025
———
[Slide 3]
Adverse event profile ubamatamab
- Most common treatment emergent events:
- cytokine release syndrome 85% and pain 73.3%
- Anemia and neutropenia 8.0% and 14% grade 3+
- 5% discontinuation rate
- Other noteworthy side effects from dose escalation R4018-ONC-1721
- dry eyes 16.7% all grades, zero grade 3+
- pleural effusions 15.4% all grades, 2.6% grade 3+
Source: Lee JY ESMO 2025, Moore KN, et al. ESMO; 2023
———
[Slide 4]
EGFRxCD28 (REGN7075) + Cemiplimab
Table Total (N=84), n (%) Any Grade / Grade 3-4*:
TRAEs occurring in >5% of patients 76 (90.5) / 6 (7.1)
IRR 49 (58.3) / 2 (2.4)
Fatigue 14 (16.7) / 0
Rash maculopapular 11 (13.1) / 1 (1.2)
Dermatitis acneiform 9 (10.7) / 0
Nausea 9 (10.7) / 0
Pruritus 7 (8.3) / 0
Diarrhea 6 (7.1) / 0
Pyrexia 6 (7.1) / 0
Vomiting 5 (6.0) / 0
- Dose escalation, multiple tumor types, no NSCLC, 94 patients enrolled and ORR 20%
- Infusion reactions led to discontinuation in 4/84 patients
- 17.9% serious treatment emergent events
Source: Segal NH, et al. ASCO; 2024
Dr. Arjan Gower @ArjanGower (@UCLA) presents Phase 1 data on VT3989: 26% ORR, 85% disease control in heavily pretreated patients, with manageable safety. Antitumor activity enriched in low/absent Merlin expression. TEAD inhibition shows promise in mesothelioma. #DAVALung
[Slide 1]
TEAD targeting drugs in clinical trials
Drug | Sponsor | Mechanism of Action | TEAD selectivity | Clinical trial
VT3989 | Vivace | Non-covalent autopalmitoylation inhibitor | TEAD 1,(2),3,(4) | NCT04665206 Phase I/II started 3/2021
IAG933 | Novartis | YAP/TAZ-TEAD PPI inhibitor | Pan-TEAD | NCT04857372 Phase I started 10/2021
BPI-460372 | Betta | Covalent autopalmitoylation inhibitor | TEAD 1,3,4 | NCT05789602 Phase I started 4/2023
BGC515 | BridGene | Covalent autopalmitoylation inhibitor | Pan-TEAD | NCT06452160 Phase I started 6/2024
SW-682 | SpringWorks | Autopalmitoylation inhibitor | Pan-TEAD | NCT062513010 Phase I started 7/2024
ISM6331 | Insilico | Non-covalent autopalmitoylation inhibitor | Pan-TEAD | NCT06566079 Phase I started 12/2024
Source: Adapted from Harvey and Tang, Nat. Rev. Drug Discov. 2025. Slide 278
———
[Slide 2]
VT3989 Background
- Oral, selective small molecule inhibitor of TEAD autopalmitoylation to disrupt YAP transcriptional activity
- Binds all 4 TEAD paralogs (TEAD 1-4), though it more strongly blocks TEAD1 and TEAD3 in preclinical studies
- VT3989 cell proliferation assays in meso cell lines
- Merlin-positive cells retain expression of NF2-encoded tumor suppressor merlin
- In Merlin-positive cell lines, VT3989 was ~100-1000X less efficacious
Table (Cell Line | VT3989 GI50 (nM) | Max inh % | NF2 Mutation | Merlin Level): NCI-H226 9/101; NCI-H2373 8/92; SDM103T2 26/82; NCI-H2052 16/93; ACE-MESO-1 15/84; SPC212 60/72; JU77 74/82; Mero-48a 38/109; ZL34 20/95; ZL55 48/87; Mero-14 60/94; Mero-82 118/75; ONE58 186/67; Mero-83 118/75; Mero-95 297/67; Mero-41 260/71; ZL5 178/80; SPC111 1511/64; NO36 >3000/95; Mero-84 >3000/33; ACE-MESO-4 879/67; Mero-25 2494/54; NCI-H28 >3000/0; NCI-H2452 >3000/0; HMMME >3000/0. (Merlin Level Low/Undetectable for NF2-truncated/deleted lines; Detected for no-mutation lines.)
Source: Yap et al, Nature Medicine 2025. Slide 279
———
[Slide 3]
First-in-human Phase 1 Schema of VT3989
Enrolled (N=172) -> Dose-escalation phase (N=85) and Dose-expansion phase (N=87 [75]).
Dose-escalation: Continuous dosing schedule Cohorts 1-5 (N=27 [13]) - 200 mg 4 pts (0 DLT), 150 mg 6 pts (0 DLT), 100 mg 6 pts (0 DLT), 50 mg 6 pts (0 DLT), 25 mg 5 pts (0 DLT); Intermittent dosing schedule Cohorts 6-14 (N=58 [47]) - 200 mg daily 2W/1W n=6, 200 mg daily 1W/2W n=6, 200 mg daily 2W/2W n=5, 100 mg daily 2W/2W n=6, 150 mg daily 1W/3W n=6, 100 mg daily 2W then 100 mg QW n=7, 50 mg daily 2W then 50 mg QW n=6, 50 mg daily 2W/2W n=10, 50 mg BIW n=6.
Dose-expansion: EC-1: 100 mg daily 2W/2W (NPM/PM) N=27; EC-2: 50 mg daily 15 days followed by 100 mg weekly (NPM/PM) N=27. RP2D: EC-3: 100 mg daily 2W/2W (NPM) N=17; EC-4: 100 mg daily 2W/2W (other solid tumors) N=12; EC-5: 100 mg daily 2W/2W (PM) N=4.
- 100 mg qD, 2 weeks on, 2 weeks off as RP2D. Exposure-response analysis revealed higher dosing did not enhance efficacy, but correlated with increased toxicity (proteinuria).
- After a protocol amendment, 22 additional pts with advanced mesothelioma received VT3989 treatment under a higher UACR threshold.
- Primary efficacy analysis included pts (N=47) with advanced mesothelioma treated at the clinically optimized regimen: 50 mg QD 2 W/2 W and 100 mg QD 2 W/2 W with a higher prespecified UACR threshold.
Source: Yap et al, Nature Medicine 2025. Slide 280
———
[Slide 4]
VT3989 activity in mesothelioma at RP2D
Waterfall plot (Best change from baseline, +75 to -50) with PR (blue), SD (green), PD (red).
Table Investigator-assessed response | Clinically optimized dose regardless of UACR threshold (N=47) | Clinically optimized dose and optimal UACR threshold (N=22):
Partial response; n (%) 12 (26%) / 7 (32%)
Stable disease; n (%) 28 (60%) / 12 (54%)
Disease control rate; n (%) 40 (85%) / 19 (86%)
Duration of response (median weeks) 24 / NE
PFS (median weeks) 25 / 40
100% had prior immunotherapy, and 82% had prior chemotherapy.
Source: Yap et al, Nature Medicine 2025. Slide 281
Molecular profiling is rewriting mesothelioma surgery. Dr. Marc de Perrot (@UofT) breaks down BAP1/p16-guided strategies, SMARTEST trial data & the shift to personalized, multimodal care integrating RT, IO & surgery. #DAVALung
EORTC 1205IMPRINTMARS 2SMARTSMARTERSMARTEST
[Slide 1]
Surgery for mesothelioma: multimodal strategy
Trimodality approach (chemo-EPP-radiation) branches into:
- Chemotherapy combined with EPD: MARS 2 trial, EORTC 1205 trial -> Phase II trials (Induction ICB-surgery)
- EPD followed by Hemithoracic radiation: IMPRINT trial (Phase III ongoing)
- Hemithoracic radiation before surgery: SMART trial, SMARTER trial -> SMARTEST trial (RT-surgery-adjuvant ICB)
Footer: UHN Princess Margaret Cancer Centre
———
[Slide 2]
Circulating tumor DNA to select patients for surgery
Oncoprint/heatmap rows: PFS (PFS months 10-40), Arm (A/B), Surgery feasible (No/Yes), Surgery completed (No/Yes), All, C1D1, C2D1, C3D1, Pre-surgery, Post-surgery. ctDNA evaluable legend: Detectable (yellow), Undetectable (blue), Not evaluable (grey).
Long PFS = ctDNA negative (n=10) or clearance with ICB and surgery (n=3).
Source: Reuss et al. Nat Med 2025;31:4097-108
———
[Slide 3]
Designing the SMART approach - change of paradigm
Old: Chemotherapy / EPP / Hemithoracic radiation => New: Hemithoracic radiation / Surgery / +/- Systemic therapy
Rational:
- Optimal delivery of radiation based on PET and CT findings
- Sterilization of the tumor before surgery with less risk of seeding
- Shorter treatment
- BAP1 loss tumor cells are particularly responsive to radiation
- Potential immunogenic benefit
Footer: UHN Princess Margaret Cancer Centre
———
[Slide 4]
Surgery for mesothelioma after radiation therapy using exquisite systemic therapy - SMARTEST trial
Schema: Eligibility (Untreated MPM, T1-3N0-1M0, Surgically resectable) -> Radiation (24-36 Gy combined with 8-12 Gy in 3 fractions on alternate days) -> R 1:1 N=30 -> [Cyclophosphamide 50 mg po bid x 7 days starting on the last day of radiation OR No treatment] -> Surgery (MCR) EPP or EPD on Day 14+/-2 -> Assessment for immunotherapy at 6 weeks after surgery -> Tremelimumab durvalumab Q 4 weeks x 4 cycles then Durvalumab Q 4 weeks x 9 cycles.
Primary endpoint: CD8 TILs density at surgery.
Secondary endpoints: OS and DFS; Toxicity; Subgroup analysis by genotypes (BAP1loss p16HD).
Footer: UHN Princess Margaret Cancer Centre
Smoking history continues to shape lung cancer outcomes long after diagnosis. Lawson Eng, MD (@Lawson_Eng@pmcancercentre@UHN) reviews prognostic data by smoking status, timing of cessation interventions, standardized tobacco assessment in clinical trials, and ongoing research
[Slide 1]
The Impact of Smoking Status on Lung Cancer Staging
- Evaluation of smoking status on IASLC 9th edition staging cohort consisting of 48,531 NSCLC cases with smoking data
Cancer-specific survival curves (CSS %) by stage and smoking status (Never/Former/Current) over Years from Diagnosis. Data table (Deaths / N; Median in Years; 5-Year Estimate):
- IB Never: 384 / 1606; NR; 76% (74, 79)
- IB Former: 594 / 2003; 8.9 (7.8, .); 66% (64, 69)
- IB Current: 343 / 1164; 8 (6.9, .); 66% (63, 69)
- IIA Never: 267 / 929; NR; 69% (64, 71)
- IIA Former: (values); NR; 71%
- IIA Current: 291 / 784; 6.5 (5.5, .); 56% (52, 60)
- Within each stage, patients who currently and formerly smoked had poorer prognosis than patients who never smoked
- Between stage groups, patients who smoked had a prognosis similar to those who never smoked in the next highest stage group
- In recursive partitioning analysis, among patients who had up to T3 N1 stage NSCLC, smoking status had a greater impact on prognosis than N0 vs N1 status
Eng et al. J Thorac Oncol. 2025 Oct;20(10):1441-1458
———
[Slide 2]
Why Timing of Smoking Cessation Interventions Matters
- Prospective cohort study for patients enrolling at MD Anderson Tobacco Treatment Program from 2006 to 2022 (n=4256)
KM survival curves (Abstinent vs Nonabstinent), Survival % over Years from diagnosis:
A <6 mo: median survival gap markers 2.1 y and 3.9 y; Log-rank P<.001. No. at risk: Abstinent 1067, 537, 227, 51; Nonabstinent 1076, 509, 208.
B 6 mo to 5 y: markers 4.8 y and 6.0 y; Log-rank P<.004. No. at risk: Abstinent 586, 417, 223, 46; Nonabstinent 1117, 726, 338, 87.
C >5 y: curves overlap; Log-rank P=.99. No. at risk: Abstinent 247, 247, 187, 104; Nonabstinent 433, 433, 347, 186.
Starting smoking cessation treatment within 6 months of diagnosis leads to a 2 year improvement in OS for the 75th percentile among patients who quit; benefit diminishes over time.
Cinciripini et al. JAMA Oncol. 2024 Dec 1;10(12):1689-1696
———
[Slide 3]
What are some knowledge gaps to fill moving forward?
- Tobacco negatively impacts surgical outcomes, radiation therapy outcomes and some systemic therapy outcomes
- What about newer drugs or treatments? Newer TKIs? ADCs? Cell therapy? Bi-specifics?
- Systematic Scoping Review of published Cancer Cooperative Group Clinical trials from January 2017 to June 2019
- 91 studies identified representing 90 trials
- Only 19 / 91 (21%) studies reported data collection on tobacco use; mainly lung and head and neck trials
- Only about half of trials collecting tobacco report analyzing or present tobacco data
Table (Variable / Category / Number of studies (n=19) (%)):
- Format For Baseline Smoking Status: Ever Smoked / Never Smoked 37%; Current / Former / Never 53%; Unknown 11%
- Smoking Intensity Collected at Baseline: Pack Years 21%; Not Captured 79%
- Smoking Information Presented in Tables: Presented in Main Tables 89%; Not Presented 11%
- Reported Verification of Smoking Status: Yes 0%; No 100%
- Reported Follow-up Smoking Status Collected: Yes 11%; No 89%
- Smoking Status Used in Analysis: Yes 37%; Analyzed but not displayed 26%; No 47%
- Second-Hand Smoke Exposure Reported: Yes 0%; No 100%
Eng L et al. ESMO Open. 2022 Dec;7(6):100605.
———
[Slide 4]
IASLC Position Statement on Documentation of Smoking Status in Cancer Clinical Trials
The Lancet Oncology, Volume 26, Issue 8, August 2025, Pages 990-993. "Cancer clinical trials should capture tobacco smoking status." William K Evans, Matthew Evison, Mehdi Sheikh, Lawson Eng, Oladelson Ayo-Yusuf, Abhishek Shankar, Joelle T Fathi; International Association for the Study of Lung Cancer Tobacco Control and Smoking Cessation Committee.
Recommendations:
- Document tobacco use status at cancer diagnosis and at clinical trial registration using standardized definitions from the validated Cancer Patient Tobacco Use Questionnaire (C-TUQ)
- Document the use of tobacco products (including electronic cigarettes and heated tobacco products) at regular intervals over the course of the clinical trial
- Document any methods of smoking cessation used by tobacco users over the course of the clinical trial and their effectiveness
- Verify smoking status using biochemical measures, whenever possible
- Analyze the effect of tobacco use on clinical trial outcomes including response rate, progression free and overall survival, treatment related toxicity, adverse events, compliance with trial procedures, and quality of life
Collecting this information may help provide further data to support the importance of smoking cessation in lung cancer survivorship.
Evans WK. Lancet Oncol. 2025 Aug;26(8):990-993
Dr. John Heymach (@MDAndersonNews) unveils a multimodal AI digital twin for lung cancer, predicting patient trajectories using radiomics, synthetic PET, and ctDNA. #DAVALung
[Slide 1]
Construction of a multimodal patient-specific digital representation: the Lung Foundation Model
Transforming multimodal patient data into quantitative representations of patient biology
Radiomics
- Whole-body 3D tumor burden & their evolution under treatment
- Habitat imaging for intratumoral heterogeneity
- Synthetic PET
Clinical & Molecular
Pathomics
- Patch Embeddings
- Foundation modeling
Patient-specific digital representation
- disease burden
- cancer biology
- microenvironment
- molecular evolution
- clinical context
- response dynamics
Trajectory Prediction
LLM/Agentic AI
- Radiology, Pathology, Clinical Notes -> Multimodal Fusion -> Knowledge -> Agent AI
a) Wu et al, Radiology, 2018. b) Wu et al, Nat Mach Intell. 2021. c) Salehjahromi et al, Cell Rep Med. 2024. d) Waqas et al, NPJ Precis Oncol. 2026. e) Bandyopadhyay et al, AACR Press Program. 2026
324
———
[Slide 2]
Response prediction using Synthetic PET From CT
1. Generating Synthetic PET (CT -> Synthetic PET)
2. Imaging Validation - Imaging Similarity Metrics; Radiogenomics (GSEA); Imaging Feature Correlation; Quality Assessment; Turing Test
3. Clinical Validations - Prognosis; Diagnosis; Cancer Prediction; Imaging Prediction
The challenge: standard CT response assessment typically based on tumor linear measurement (RECIST) or volumetrics.
Can more useful data regarding response be derived from CT?
[Image panels: MDA-TEST and TCIA-STANFORD showing CT, ground truth PET, synthetic PET]
Cell Reports Medicine, 2024 (Wu lab)
collaborators include C.Wu, J. Zhang, C. Chung, D. Gibbons, A. Vaporciyan
———
[Slide 3]
Multimodal AI model integrating radiomics and ctDNA to predict neoadjuvant IO response in AEGEAN
RECIST uses delta SLD (sum of longest diameter). Doesn't take into account changes in volume or density (e.g., necrotic regions). ~3 cm.
Example of negative delta energy (i.e., shrinkage in tumor volume and decrease in intensity). Screening -> Pre-surgery. delta E < 0.
Energy = sum of squares of voxel values within the primary lung tumour.
delta energy = percentage change of energy*
- Here, tumour response was based on changes in radiomic features (the delta energy of the primary lung tumour*)
- Radiomic features and ctDNA detection status (i.e., positive or negative) at C3D1 were used to train models to predict pCR in patients treated with durvalumab, and assessed via Cox regression for associations with EFS and OS
- Clinical features comprising age, sex, ECOG PS, race, smoking status, disease stage, histology, PD-L1 status, BMI and lab variables were also included in models to predict pCR
Heymach et al, ESMO 2025; collaboration with AstraZeneca.
———
[Slide 4]
Application of MDA Lung Foundation Model to estimate treatment effects from single arm study
Estimating treatment benefit through patient-specific counterfactual simulation
(1) Clinical Challenge
- BrightStar (Phase II Clinical Trial): BrighStar Trial (P): Your Choice; 9 patients Brigatinib vs Brigatinib + LCT; Does LCT work??
- Single-arm Trial + Missing control arm = Quantify trial results??
- ALTA-1L Phase III Trial: 1st gen TKI (126); 2nd gen TKI (118)
(2) MATRIx Digital Twin
- GEMINI (~10k) + No LCT -> RADiCC (N = 613) + Real-world Data -> MATRIx-DT -> Clinical trial; Observed outcome (with LCT); Synthetic outcome (no LCT)
Digital Twin of each TKI Generation: PFS by TKI generation; 1st gen TKI HR 0.58 (95% CI: 0.4 - 1.2), p = 0.44; 2nd gen TKI HR 1.80 (95% CI: 0.68 - 4.7), p = 0.002
(4) Estimate Treatment Benefit
- 32 Patients Received LCT; BrightStar Phase II Trial: 2nd gen TKI (32) + LCT; What if these patients had not receive LCT? Digital Twin PFS; HR = 2.8 (1.4-6.4); Log-rank test p = 0.002
Wu, Elamin et al AACR 2026
330
Targeting MYB in adenoid cystic carcinoma: Dr. Renata Ferrarotto (@MDAndersonNews) presented Ph1/2 ARIA data on REM-422, an oral MYB mRNA degrader, showing ORR 43% and DCR 100% in biomarker+ R/M ACC at the 24mg RP2D. #DAVALung
ARIA
[Slide 1]
[Slide 1] REM-422 induces MYB mRNA degradation through inclusion of a poison exon (PE)
- Small molecule, once daily oral administration
- REM-422 promotes poison exon inclusion in the MYB pre-mRNA
- Poison exon incorporation results in degradation of MYB mRNA and protein
[Diagram: pre-mRNA with Poison exon / Premature termination codon (PTC); EXONs; mRNA; protein]
Ferrarotto R, ASCO, 2026
[Slide 2] Ph1/2 ARIA (A study of REM-422 In ACC)
Ph1 DOSE ESCALATION (all-comers): N = 69
PRIMARY OBJECTIVE - SAFETY, RP2D
Secondary objectives - PK, PD and efficacy
- Recurrent or metastatic (R/M) ACC
- Tumor biopsies retrospectively assessed for MYB status
Dosing: oral REM-422 once daily
DL1 (3mg) N = 6; DL2 (6mg) N = 4; DL3 (13mg) N = 4; DL4 (18mg) N = 16; DL5 (24mg) N = 15; DL6 (30mg) N = 9; DL7 (38mg) N = 9; DL8 (48mg) N = 6
18 and 24mg doses evaluated to identify optimal dose -> RP2D 24mg
Ph2 CONFIRMATORY COHORT (PE+): N = 40-50; PRIMARY OBJECTIVE - ORR (BICR)
Key Eligibility: R/M, locally advanced unresectable ACC; Disease progression within 12m; Biomarker positive tumor
Ferrarotto R, ASCO, 2026
———
[Slide 2]
TRAEs Gr3-4
Columns: 3mg QD N=6 | 6mg QD N=4 | 12mg QD N=4 | 18mg QD N=16 | 24mg QD N=15 | 30mg QD N=9 | 38mg QD N=9 | 48mg QD N=6 | TOTAL N=69
(values shown as n (%))
Lymphocyte count decreased: 1(17), 0, 0, 1(6), 0, 1(11), 3(33), 2(33), 8(12)
Neutrophil count decreased: 0,0,0,0,0,0,1(11),1(17),2(3)
White blood cell count decreased: 0,0,0,0,0,0,1(11),1(17),2(3)
Aspartate aminotransferase increased: 0,0,0,0,0,0,0,1(17),1(1)
Blood alkaline phosphatase increased: 0,0,0,0,0,0,0,1(17),1(1)
Anaemia: 0,0,0,1(6),0,2(22),1(11),2(33),6(9)
Fatigue: 0,0,0,0,0,1(11),1(11),1(17),3(4)
Face oedema: 0,0,0,0,0,0,1(11),0,1(1)
Malaise: 0,0,0,0,0,0,1(11),0,1(1)
Peripheral motor neuropathy: 0,0,0,1(6),1(7),1(11),0,0,3(4)
Peripheral sensory neuropathy: 0,0,0,0,0,1(11),1(11),0,2(3)
Muscular weakness: 0,0,0,1(6),0,1(11),0,0,2(3)
Acute kidney injury: 0,0,0,0,0,0,1(11),0,1(1)
Proteinuria: 0,0,0,0,0,0,1(11),0,1(1)
Epistaxis: 0,0,1(25),0,0,0,0,1(17),2(3)
Only 2 patients had Gr4 TRAEs: 1) 38mg: neutrophil and lymphocyte counts decreased 2) 48mg: lymphocyte count decreased
No DLTs. No D/C due to TRAE at RP2D
Ferrarotto R, ASCO, 2026
———
[Slide 3]
[Slide 1] Change in tumor size by biomarker status
Waterfall plot: Best % change in target lesions (axis 40 to -80). Biomarker Status: Biomarker Positive (red); Biomarker Negative (black); Unknown; Ongoing (arrow).
Radiographic images: Baseline; On-treatment (M5)
[Slide 2] Best % change in tumor size from baseline by dose
Waterfall by dose: 3mg, 6mg, 12mg, 18mg, 24mg (RP2D), 30mg, 38mg, 48mg. Best % change in tumor size (axis 60 to -80). Ongoing (arrow).
Table: Evaluable | N | Responders | ORR | DCR
BM+ >= 24mg: 19 | 7 | 37% | 95%
BM+ at 24mg: 7 | 3 | 43% | 100%
- Responses achieved in BM+ patients at doses of >=12mg
- In BM+ patients, ORR = 43% and DCR = 100% indicates encouraging clinical activity at RP2D
- Best efficacy profile at 24mg (RP2D) due to combination of robust target engagement and tolerability
———
[Slide 4]
Responses across ACC-I/II and irrespective of prior lines
Spaghetti plot: Best % change in target lesions (20 to -80) vs Months (1-25); Pt1-Pt9.
Table: Pt ID | Dose Level | Response | Histology | ACC Subtype | # Prior Lines of Therapy | DOT (months) | DOR (months)
1 | 12mg | cPR | Solid component | ACC-II | 0 | 23+ | 15+
2 | 18mg | cPR | Cribriform | ACC-I | 2+ | 10+ | 6+
3 | 24mg | uPR | Cribriform | ACC-II | 1 | 20+ * | 6
4 | 24mg | cPR | Unknown | ACC-I | 1 | 19+ | 12+
5 | 24mg | cPR | Solid component | Unknown | 2+ | 19+ | 13+
6 | 38mg | cPR | Unknown | Unknown | 2+ | 12+ | 5+
7 | 38mg | cPR | Tubular | ACC-I | 2+ | 16+ | 1+
8 | 48mg | uPR | Cribriform | ACC-I | 2+ | 5 | 2
9 | 48mg | cPR | Unknown | Unknown | 2 | 14+ | 7+
- Anti-tumor activity across ACC subtypes, and after multiple lines of therapy (including ADCs)
- Long durability with patients on therapy for up to 2 years and ongoing (mDOR not reached)
Can mRNA vaccines enhance immunotherapy? Steven Lin, MD, PhD (@StevenLin_MDPhD@UTMDAnderson) reviews retrospective NSCLC data showing improved outcomes with COVID-19 mRNA vaccination across PD-L1 TPS subgroups (TPS <1%: HR 0.53; TPS 1–49%: HR 0.48; TPS ≥50%: HR 0.55), with
[Slide 1]
COVID mRNA vaccines are associated with improved responses to ICI in NSCLC, regardless of TPS scores for PD-L1
Unresectable Stage III NSCLC (CRT->durva): adj HR, 95% CI: 0.37, 0.16-0.89 (COVID mRNA Vaccine vs No Vaccine). No. at risk: No Vaccine 108, 83, 54, 35, 23; COVID mRNA Vaccine 30, 24, 16, 10, 0.
Stage IV NSCLC (overall) (frontline IO +/- chemo): adj HR, 95% CI: 0.52, 0.37-0.73. No. at risk: No Vaccine 574, 340, 200, 106, 61; COVID mRNA Vaccine 540, 90, 64, 33, 3.
Stage IV NSCLC, TPS <1%: HR 1.22, 95% CI = 0.73-2.04. No. at risk: No vaccine 152, 97, 51, 23, 11; Pandemic era no vaccine 46, 33, 18, 9, 1.
Stage IV NSCLC, TPS 1-49%: HR = 0.46, 95% CI = 0.31-0.76. No. at risk: No vaccine 205, 124, 74, 43, 20; COVID mRNA vaccine 24, 25, 16, 8, 1.
Stage IV NSCLC, TPS >=50%: HR = 0.55, 95% CI = 0.34-0.87. No. at risk: No vaccine 187, 128, 74, 43, 20; COVID mRNA vaccine 37, 27, 21, 13, 1.
Grippin, et al., Nature 2025. UT MD Anderson.
———
[Slide 2]
Survival benefits were NOT observed with chemotherapy or non-mRNA vaccines
NSCLC + Chemotherapy +/- SARS CoV2 vaccine: HR, 95% CI: 0.77, 0.51-1.17. Overall Survival % over Months from Therapy Start. No Vaccine 169, 105, 73, 54, 37; COVID Vaccine 62, 47, 35, 22, 4.
NSCLC + ICI +/- influenza vaccine: HR, 95% CI: 1.10, 0.83-1.45. Months from ICI Start. No Vaccine 477, 286, 159, 85, 53; Influenza Vaccine 95, 60, 37, 19, 11.
NSCLC + ICI +/- pneumococcal vaccine: HR, 95% CI: 1.10, 0.71-1.70. Months from ICI Start. No Vaccine 580, 356, 209, 114, 75; Pneumonia Vaccine 33, 26, 13, 7, 4.
Grippin, et al., Nature 2025. UT MD Anderson.
———
[Slide 3]
COVID mRNA vaccines are associated with increased PD-L1 expression in lung cancer
NSCLC n=2,358. Closest vaccine prior to biopsy? None n=1980; <100 Days n=151; >100 Days n=227. Measured PDL1 (TPS).
Bar chart PDL1 (%): No Vaccine (n=1980) ~25%; <100 Days (n=151) ~31% (elevated, * significant); >100 Days (n=227) ~23%. * markers indicate significant differences between <100 Days vs None and vs >100 Days.
Violin plot PDL1 (%) with % of cases >=50% (green dashed line at 50): No Vaccine 28%; <100 Days 33%; >100 Days 24%. * significance markers between <100 Days and adjacent groups.
Grippin, et al., Nature 2025. UT MD Anderson.
———
[Slide 4]
Emerging validation studies in other cohorts
Bulgaria National Study: "Impact of COVID-19 and vaccination on long-term survival in patients with solid malignancies: A nationwide cohort study." George Dimitrov, Radka Argirova, Trifon Valkov (Medical University of Sofia, Bulgaria). OS % over Months curves: SM w/o comorbidities (mRNA); SM w/o comorbidities (vector); SM w/o comorbidities (non-vaccinated). chi2=12.36, df=1, log-rank P=0.0003. No at risk: SM w/o comorbidities (mRNA) 334, 283, 174; (vector) ..., 93; (non-vaccinated) 1174, 821, 246.
Israel National Study: "Validation of 'SARS-CoV-2 mRNA vaccines sensitize tumors to immune checkpoint blockade' in an independent cohort of 4,407 patients." Ronen Arbel, Lior Rokach, Talish Razi, Tamar Tadmor. KM curves Vaccinated vs Not vaccinated for Melanoma (p<0.001) and Lung cancer (p<0.001).
Dimitrov et al., Eur J Cancer 2026. Arbel et al., Cancer Letters 2026. UT MD Anderson.
Beyond one-size-fits-all salvage therapy: @ValsamoA from @HopkinsMedicine, discussed how multi-omic profiling of IO-resistant NSCLC could inform biomarker-driven and combination treatment approaches. #DAVALung
HUDSON
[Slide 1]
Clinical and molecular features of immunotherapy resistance
Immunotherapy (IO) resistance is broadly classified into two categories:
Primary resistance: No measurable response to therapy within 6 months.
Acquired resistance: Initial clinical benefit for 6 months (24 weeks), followed by disease progression.
Resistance to immune checkpoint inhibition in advanced non-small cell lung cancer (NSCLC) is driven by tumor-intrinsic and tumor-extrinsic mechanisms.
Acquired resistance-associated genotypes detected in ~28% of IO-treated NSCLC. [Oncoprint of genes: STK11, KEAP1, SMARCA4, ...]
Chronic IFN-gamma signaling linked with dysfunctional immune response in acquired resistance. [Hallmark / Literature / Immune Cells bar plot]
Understanding the shared and unique molecular mechanisms driving immunotherapy acquired and primary resistance is essential for overcoming therapeutic failure.
Anagnostou V, Sci Transl Med, 2022; Alsaafeen BH, Mol Cancer, 2025; Schoenfeld AJ, Cancer Discov 2020; Anagnostou V, Cancer Discov, 2017; Adapted from Ricciuti B, J Clin Oncol 2024; Memon D, Cancer Cell, 2024
———
[Slide 2]
HUDSON: Phase 2 multi-drug, biomarker-directed, umbrella study in NSCLC progressed on anti-PD(L)-1 therapy
HUDSON central screening (N = 951). Eligibility Criteria: Locally advanced or metastatic NSCLC; progression following previous platinum-based chemotherapy; failure of prior anti-PD-(L)1 immunotherapy; suitable for new tumor biopsy post-progression on anti-PD-(L)1 therapy; no targetable alterations in EGFR, ALK, ROS1, BRAF, MET, or RET.
Group A: Biomarker-matched - HRRm: Olaparib (PARPi) + durvalumab; LKB1: Ceralasertib (ATRi) + durvalumab; ATM: Ceralasertib (ATRi) + durvalumab; ATM: Single-agent ceralasertib (ATRi); RICTOR: Vistusertib (mTORi) + durvalumab; CD73: Oleclumab (CD73 mAb) + durvalumab; HER2a: Trastuzumab deruxtecan (HER2i) + durvalumab; HER2m.
Group B: Biomarker-non-matched - Primary resistance (disease progression <=24 weeks) vs Acquired resistance (disease progression >24 weeks): Olaparib (PARPi) + durvalumab; Danvatirsen (STAT3i) + durvalumab; Ceralasertib (ATRi) + durvalumab; Oleclumab (CD73 mAb) + durvalumab; Cediranib (VEGFi) + durvalumab.
Group C: Molecular aberration independent - Ceralasertib (ATRi) + durvalumab; Single-agent ceralasertib (ATRi).
Exploratory endpoints - Landscape Characterization: Delineate the genomic, transcriptomic, and immune architectures distinguishing primary versus acquired resistance to prior IO (HUDSON screening population). Biomarker Discovery: Identify predictive biomarkers and mechanisms mediating response or resistance to durvalumab-based combination therapies.
Iyer S, et al. presented at AACR 2023 (Abstract CT039); Besse B et al., Nat Med, 2025; Besse B et al., Manuscript in preparation
———
[Slide 3]
Comprehensive multi-omic analyses of IO resistance in NSCLC: Cohort description and sample disposition
IO-resistant NSCLC (N=951*), HUDSON screening population. Acquired IO resistance (n = 507); Primary IO resistance (n = 393). Sequencing modality by PD-L1: Targeted tumor NGS (Pre-IO / Post-IO), ctDNA analysis, Bulk RNA sequencing, TCR VB sequencing, Single-cell RNA seq.
- Largest-to-date cohort of IO resistance in NSCLC (n=951).
- HUDSON trial: Phase 2 multi-drug, biomarker-directed, umbrella study in NSCLC progressed on anti-PD(L)1 therapy.
- Tumor genomic profiling by targeted NGS in unpaired pre- and post-IO (pre-HUDSON) tumor biopsies to assess TMB, clonal composition, genotype enrichment, mutational signatures, and genomic instability.
- Circulating tumor DNA analysis to evaluate post-IO (pre-HUDSON) tumor burden, and TCR NGS for peripheral T-cell repertoire profiling.
- Transcriptomic profiling by bulk RNA sequencing of post-IO (pre-HUDSON) tumors, followed by gene set enrichment analyses and sequence deconvolution.
- Single-cell RNA sequencing of post-IO (pre-HUDSON) tumors used for high-resolution cell-type annotation and differential cell cluster enrichment analyses in the acquired vs primary resistance subsets.
*Resistance not annotated, n=51. Abbreviations: IO, immunotherapy; NGS, next-generation sequencing; ctDNA, circulating tumor DNA; seq, sequencing; TCR, T-cell receptor.
———
[Slide 4]
Putting together the immunotherapy resistance puzzle
We analyzed the largest-to-date cohort of IO resistance in NSCLC, compiled within the HUDSON phase 2 clinical trial.
IO resistance is multi-factorial, as cancer cells acquire a fitness advantage through differential activation of cancer hallmarks, cell states, and immune escape, pointing towards convergent evolution.
Divergent genomic landscapes: Primary and acquired resistance differ: Primary links to STK11, MYCN, NF2 mutations; acquired shows cell-cycle/DDR (CDK4, RB1, MSH3), chromatin regulation, proliferative signaling (FGF10, RICTOR) and dedifferentiation (SMARCA4) alterations. Both display increased genomic instability; driver landscapes demand state-specific targeting.
Lineage plasticity & metabolic reprogramming: Acquired resistance is strongly associated with a "pluripotent stem-like" epithelial phenotype and Epithelial-to-Mesenchymal Transition (EMT), while metabolic rewiring post-IO (up OxPhos/Glycolysis/MYC) enhances immunosuppression.
Immune hypofunctional states: Acquired resistant tumors remain inflamed (IFNy, TNFa), harbor tumor-reactive CD8 TRMs and show enrichment of pre-exhausted stem-like T cells, suggesting hypofunctional T cell states rather than exclusion.
The evolutionary cost of IO resistance, mediated by defects in DNA damage repair/homologous recombination deficiency, cell cycle deregulation, metabolic reprogramming, and lineage plasticity, creates actionable vulnerabilities.
Personalized, combination strategies are required in the post-IO setting rather than a 'one-size-fits-all' salvage approach.
#PM2.5 & lung cancer risk: Dr. @HinaKhanMD (@BrownUniversity) reviewed epidemiologic & mechanistic evidence that PM2.5 (IARC Group 1 carcinogen) raises lung cancer risk with no safe threshold, and highlighted local Breathe Providence data in RI. #DAVALung
[Slide 1]
EPIDEMIOLOGICAL EVIDENCE
Year | Study | Population | Major Finding
1975-1997 | Harvard Six Cities | ~8,000 (25-74 years) | Monitoring stations in each community. Adjusted lung cancer mortality rate ratio RR; 1.37 per 10 µg/m3 increase in PM2.5
1982-2012 | ACS CPS-II | 1.2 million (>30 years) | Every 10 µg/m3 PM2.5 increased lung cancer mortality by ~14-27%. Adjusted lung cancer mortality RR was 1.14 for a 10 µg/m3 increase in PM2.5
1974-1983 | Japanese | 63,530 | Adjusted lung cancer mortality hazard ratio (HR) was 1.24 for a 10 µg/m3 increase in PM2.5
2001 | Italian | 1,265,058 (>30 years) | 5% higher lung cancer mortality risk was observed for a 10 µg/m3 increase in PM2.5
2013 | ESCAPE | 312,944 Europeans | PM associated with incident lung cancer; strongest association for adenocarcinoma
2021 | ELAPSE | 306,550 Europeans | Increased lung cancer risk even at low PM2.5 concentrations; no clear safe threshold
2022 | UK Biobank | 298,069 | PM2.5 associated with adenocarcinoma and squamous carcinoma; genetic risk did not eliminate PM effect
2023 | Nature (Swanton et al) | Human + mouse + UK Biobank | PM2.5 promotes expansion of EGFR-mutant clones through inflammation (IL-1β)
2025 | NI Case-Control | 917 cases / 8,088 controls | 37% higher lung cancer odds in highest PM2.5 exposure group despite relatively low pollution.
———
[Slide 2]
MOLECULAR PATHOGENESIS AND EMERGING HYPOTHESIS
- PM 2.5 penetrates deep into the alveoli and are absorbed into the bloodstream
- Swanton et al (2023):
- proposed that PM2.5 acts as a tumor promotor following exposure of lung cells harboring oncogenic driver mutations (potential mechanism in non-smokers)
- Focusing on EGFR-driven lung cancer: found a significant association between PM2.5 levels and the incidence of lung cancer for 32,957 EGFR-driven lung cancer cases in the UK.
- Functional mouse models revealed that air pollutants cause an influx of macrophages into the lung and release of interleukin-1β. This process results in a progenitor-like cell state within EGFR mutant lung alveolar type II epithelial cells that fuels tumorigenesis.
Particle size diagram: <5 µm in diameter -> Alveoli; 5-10 µm -> Trachea, Bronchi; >10 µm -> Nasal passage. The smaller the particles, the more damage they can do to lung -> Oxidative stress (Generation of oxygen-free radicals and oxidative DNA damage) and Inflammation (NF-κB activation, increased release of pro-inflammatory cytokines, and decreased immune function) -> Lung cancer
Valavanidis. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev. 2008;26:24. Swanton, Nature 2023.
———
[Slide 3]
BREATHE PROVIDENCE PROJECT
- Monthly average values reached peaks of 16 µg/m3 during the summer months
- The number of days/year that exceeded the WHO daily limit (15 µg/m3)
- 2023: 17-19 days across all monitors
- 2024: seen in 67 days in some monitors (with peak PM2.5 upto 42 µg/m3)
Given the high summer concentrations in 2024 as well, we suspect the pattern of air pollutant peaks in the summer cannot be attributed to the record-breaking 2023 Canadian wildfires alone, but rather additional meteorological or anthropogenic source.
Sensor modes used from Berkeley Environmental Air-quality and CO2 Network (BEACO2N) project at the University of California, Berkeley
———
[Slide 4]
GEOSPATIAL MAPPING OF PM 2.5 IN RI STATE
Specific Aim 1:
- To determine whether cumulative individual-level PM2.5 exposure is higher among patients with lung cancer compared with matched controls.
Specific Aim 2:
- Evaluate whether long-term PM2.5 exposure independently predicts lung cancer risk after adjustment for smoking and socioeconomic variables.
Specific aim 3:
- Explore disparities in PM2.5-associated lung cancer risk across vulnerable populations.
Can ICI pneumonitis be identified sooner, even before symptoms? Dr. Antonious Hazim from @MayoClinic, explored remote patient monitoring strategies to support earlier recognition and escalation of care. #DAVALung
[Slide 1]
IMMUNE CHECKPOINT INHIBITORS
- Immune checkpoint inhibitors (ICIs) have prolonged survival in patients with advanced staged cancers
- Approved for over 17 cancer types following first ICI FDA approval in 2011...
- Increasingly more frequent as part of the treatment: 2011: 1.54% -> 2018: 43.64%
- Roughly more than 233,000 patients eligible for ICIs per year
- Increase in use of ICIs -> Increase prevalence of toxicities
- Onset varies from 2-24 months with median time of 3 months; Can present after discontinuation
- The incidence of a fatal ICI-associated adverse event is estimated to be approximately 0.3-1.3%
Haslam A, Prasad V. Estimation of the Percentage of US Patients With Cancer Who Are Eligible for and Respond to Checkpoint Inhibitor Immunotherapy Drugs. JAMA Netw Open.
———
[Slide 2]
IMMUNOTHERAPY-ASSOCIATED PNEUMONITIS
- ICI therapy becoming increasingly more frequent
- Incidence of ICI pneumonitis approximately 5%
- Approximately one-third of patients are asymptomatic
- Most ICI pneumonitis is grade 1-2
- Pneumonitis can delay cancer therapy & treatment may cause opportunistic infections
Can we identify pneumonitis sooner and/or before symptoms?
———
[Slide 3]
INCLUSION CRITERIA
Cohort 1: Patients with newly diagnosed grade 1 ICI pneumonitis continuing therapy
Cohort 2: Patients with prior ICI pneumonitis who are being rechallenged
Cohort 3: Patients with COPD or ILD who will be starting an ICI
General RPM inclusion criteria: Age 18+; English speaking or able to use interpreter service; Mayo Clinic PCP or specialty provider managing care; Willing to actively use technology
———
[Slide 4]
Journal of Clinical Oncology — Meeting Abstract: 2024 ASCO Annual Meeting I; Care Delivery/Models of Care; May 29, 2024
Remote patient monitoring for early detection of immune checkpoint inhibitor therapy-related pneumonitis in high-risk patients: A pilot-feasibility study
Authors: Antonious Ziad Hazim, Gordon Ruan, Joshua Pritchett, Bobby Anderson, Konstantinos Leventakos, and Ashley Egan
Publication: Journal of Clinical Oncology, Volume 42, Number 16_suppl; https://doi.org/10.1200/JCO.2024.42.16_suppl.e13806
- 11 underwent monitoring; 5 graduated; 1 patient diagnosed w/ grade 2 ICI pneumonitis
RPM expanding into ICI-related toxicities and other non-ICI drugs (i.e. T-Dxd) within the Division of Oncology
Can CAR T finally work in solid tumors? Dr. Mehmet Altan (@MDAnderson) presents STAR-101: SynKIR-110, a novel KIR-CAR T targeting mesothelin, showed a confirmed partial response in a heavily pretreated mesothelioma patient. #DAVALung
STAR-101
[Slide 1]
SynKIR-110
- SynKIR-110 is engineered with a multichain CAR design mimicking the natural multichain activating killer immunoglobulin like receptors (KIRs).
- SynKIR-110 utilizes the SS1 antibody(Ab)-derived single chain variable fragment to target mesothelin-expressing tumors (targeting domain)
- DAP12 is a transmembrane adapter and transduce activating signals in NK cells, granulocytes, it's a signal transmitter (signaling domain)
- Two separate independent chains forms a complex only when it is bound to a tumor target.
- Separated binding and T cell activation = natural on/off switch = allows T cell rest and recovery
[Diagram: KIR-CAR T; scFv; KIRDS2; DAP12; Modeled after Natural Multi-chain Receptors]
MD Anderson Cancer Center
———
[Slide 2]
STAR-101 Phase 1 Clinical Study Design and Objectives
ClinicalTrials.gov NCT05568680
Refractory: Ovarian/fallopian carcinoma; Epithelial mesothelioma; Cholangiocarcinoma. Max n = 42 pts
Timeline: Leukapheresis -> SynKIR-110 MFG -> LD with Cy/Flu -> SynKIR-110 Single IV infusion; Enrollment screening period; Treatment Period; Post-infusion 12-month follow up; 12 mo
3+3 dose escalation: 1: 1x10^7 cells/m2; 2: 3x10^7 cells/m2; 3: 1x10^8 cells/m2; 4: 3x10^8 cells/m2; 5: 1x10^9 cells/m2; 6: 3x10^9 cells/m2; Dose expansion at RP2D
Primary objectives: Safety and feasibility
Secondary/exploratory objectives: KIR-CAR persistence levels in blood (PK); T cell-associated cytokines in serum (PD); Clinical response (iRECIST); Tumor mesothelin antigen levels (IHC)
———
[Slide 3]
STAR-101 Adverse Events and Toxicites
- Events of special interest
- Low-grade (1 or 2) CRS only, in 3 of 9 pts and was not dose-dependent
- No ICANS (0 of 9)
- Multiple grade 4 toxicities attributed to fludarabine lymphodepletion were experienced by a single patient
Table: Adverse Event Term | Cohort 1 (1x10^7 KIR-CAR T/m2) N=3 | Cohort 2 (3x10^7 KIR-CAR T/m2) N=3 | Cohort 3 (1x10^8 KIR-CAR T/m2) N=3 | Total N=9
CAR T effector cell-associated events
Cytokine release syndrome (any Grade): 2 | 0 | 1 | 3*
Grade 1: 1 | - | 1 | 2
Grade 2: 1 | - | - | 1
ICANS (any Grade): 0 | 0 | 0 | 0
AACR 2026
———
[Slide 4]
Tumor reductions following KIR-CAR T cell treatment
Spider plot: Change from baseline (%) (-50 to 50) vs Timepoints after SynKIR-110 infusion (D28, M2, M3). Cohorts 1-3 (001-001 through 004-006 patient IDs).
Waterfall plot: Change in target lesions from baseline (%) (-60 to 60); Dose cohort 1, 2, 3. * = ongoing PR 3+ mo.
- Spider plot by total sum of tumor sizes per patient at all 3 dose levels
- Waterfall plot showing best overall change in total tumor size by patient. *1 of 3 pts in DL3 = RECIST cPR
AACR 2026
Pulmonary rehabilitation extends beyond exercise. Melinda Hsu, MD, from @UHhospitals highlights a multidisciplinary approach integrating exercise training, nutrition, psychosocial support, and patient education, alongside evidence for functional improvements in lung disease.
[Slide 1]
Pulmonary rehabilitation helps in Lung diseases
Pulmonary rehabilitation (PR) improves dyspnea, fatigue, exercise tolerance, and QoL in patients with COPD, and improves respiratory function and exercise capacity perioperatively in patients with resectable lung cancer.
Components triangle: Patient Education (Interval-based exercise training; Resistance training for peripheral musculature; Inspiratory muscle exercises; Breathing retraining; Flexibility exercises; Bridge gaps in understanding of disease; Symptom management strategies; Medication management support; Smoking cessation resources); Exercise Training; Nutritional Support (Diet counseling; Weight management programs; Strategies to combat malnutrition); Psychosocial Resources (Cognitive-based therapy; Counseling; Antidepressant therapy; Family-based resources).
Zhong, J, et al. JCM 2025. Wang Q, et al. J Ca Survivorship 2026. Cleveland | Ohio.
———
[Slide 2]
Pulmonary rehabilitation helps in lung diseases - meta-analysis forest plots (Experimental vs Control; random/fixed-effects mean difference, 95% CI). Four pulmonary-function / exercise-capacity outcomes were pooled, each favouring pulmonary rehabilitation over control:
a) FVC (forced vital capacity) - favours experimental. Studies: Brock 2014, Jiang 2021, Kendall 2020, Yu 2015.
b) FEV1 - favours experimental. Studies: Brock 2014, Jiang 2021, Qiu 2021, Sui 2015, Yu 2015.
c) VO2 peak - favours experimental. Studies: Edvardsen 2015, Quist 2018, Yu 2015.
d) 6MWD (6-minute walk distance) - favours experimental.
(Pooled effect-size values are in small print and not reliably legible from the slide photo; see the source slide and publications for the exact figures.)
Zhong J, et al. JCM 2025. Wang Q, et al. J Cancer Survivorship 2026.
———
[Slide 3]
NCCN guidelines for PR perioperatively
NCCN Guidelines Version 6.2026 Non-Small Cell Lung Cancer.
Cancer Survivorship Care:
Monitoring and Managing Survivorship Needs During Systemic Therapy:
- Symptom/patient-reported outcome monitoring (NCCN Guidelines for Palliative Care, PAL-2); ESMO Clinical Practice Guideline - The Role of Patient-Reported Outcome Measures in the Continuum of Cancer Clinical Care
- Identification and management of cancer-related complications and side effects of therapy: NCCN Guidelines for Cancer-Associated Venous Thromboembolic Disease; NCCN Guidelines for Management of Immune Checkpoint-Related Toxicities; NCCN Guidelines for Cancer-Related Fatigue; NCCN Guidelines for Antiemesis
- Psychosocial evaluation and referrals: NCCN Guidelines for Distress
NSCLC Long-Term Follow-up Care:
- Cancer surveillance (NSCL-17)
- Immunizations: Annual influenza vaccination; Herpes zoster vaccine; Pneumococcal vaccination with revaccination as appropriate; COVID vaccination as per the guidance of the Centers for Disease Control and Prevention (CDC); Hepatitis vaccination
- NCCN Guidelines for Survivorship: Lung cancer-specific exercise recommendations; Consider perioperative pulmonary rehabilitation for patients with comorbid COPD and those who have undergone lung surgery; Smoking cessation: NCCN Guidelines for Smoking Cessation; Chronic cancer pain management: NCCN Guidelines for Adult...
———
[Slide 4]
Pulmonary rehabilitation in advanced NSCLC
Phase II RCT + Qualitative barriers assessment of patients and thoracic oncologists.
Study flow: Screening -> Baseline assessment -> 8 WEEKS -> Post-assessment.
Inclusion criteria: Stage III/IV NSCLC; ECOG 0-3; Self-reported dyspnea; Clinically stable on systemic therapy.
Exclusion criteria: Cardiac exclusion criteria; Mental impairment; High risk of fracture; Absence of dyspnea.
Baseline assessment (All patients): 6MWT; Pulmonary function testing; Quality of life questions; Dyspnea and fatigue assessments; Blood draw.
Randomization R 1:1 -> Systemic therapy: PR vs Systemic therapy: Usual care. All receive education: nutrition and physical activity.
Post-assessment (All patients): 6MWT; Spirometry; Quality of life questions; Dyspnea and fatigue assessments; Blood draw.
University Hospitals Seidman Cancer Center; Case Comprehensive Cancer Center; CDMRP. Cleveland | Ohio.
Radiologist shortages are slowing lung cancer trials. Dr. Dhruv Bansal (@EndeavorHealth) shows how AI-assisted radiomics cut error rates from 30.5% to 0% and nearly halved read times, while improving agreement between readers. #DAVALung
[Slide 1]
Ongoing Challenges
- Shortage of qualified radiologists
- Inter-reader disagreement among expert radiologists ranges from 20-40%
- Mean discordance in lung cancer trials reaches 32.9%
- On-site radiologists may constitute a source of bias
Schmid et al., Ther Innov Regul Sci, 2021; Beaumont et al., Cancers, 2021
Endeavor Health
———
[Slide 2]
Current Scenario
Table 3. Discrepancies at Baseline Scan Evaluation in Oncologist Assessment
Response Criteria | Reason for Discrepancy | n
RECIST version 1.0 | Patient enrolled without target lesions | 1
RECIST version 1.1 | Lymph node <15-mm short axis included as target | 3
RECIST version 1.0 | Target lesion not considered reproducible | 3
RECIST version 1.0 | Lesion <10 mm included as target | 1
RECIST version 1.1 | Lesion <10 mm included as target | 4
RECIST version 1.1 | >2 target lesions included per organ | 3
RECIST version 1.1 | >5 target lesions included per scan | 1
Source: Hersberger et al., JNCCN, 2019
Endeavor Health
———
[Slide 3]
Tumor Metrics Imaging Core Lab
Workflow: Sponsor -> PI identified in cancer center -> Protocol Reviewed / Charges Reviewed -> Patients enrolled -> Scan performed -> Radiologist A provides clinical interpretation; Radiologist B provides tumor response evaluation -> Study Coordinator reviews CRF -> Oncologist confirms overall response -> Data Coordinator submits eCRF
Source: Gurudu, Bansal et al., Abdom Radiol, 2026
Endeavor Health
———
[Slide 4]
Cost and Personnel
AI-Assisted Radiomics
- Reduced error rate from 30.5% to 0%
- Mean read time decreased from 13.1 to 6.4 minutes
- Improved interobserver agreement
- Preferred by 100% of readers
Allen et al., JCO Clin Cancer Inform, 2017
Endeavor Health
Addressing immune resistance remains a key challenge in relapsed/refractory metastatic NSCLC. Jun Zhang, MD (@Junzhang007@MethodistHosp) reviews the STOMP study, highlighting a 33.3% ORR in the efficacy-evaluable population, manageable safety, and immune profile changes
[Slide 1]
Study Design (Study Flow Diagram)
Eligibility: mNSCLC previously treated with ICI or Chemotherapy or treatment naive, EGFR or ALK positive pts failed TKIs are also eligible.
D0: ADV/HSV-tk (5 x 10^11 vp) in 2-mL volume intratumorally. Day 0 core biopsy.
D1: Valacyclovir 2 g orally t.i.d. for 14 days -> D15.
D2: SBRT 30 Gy (6 Gy X 5 fractions) over 2 weeks -> D16.
D17: PEMBROLIZUMAB 200 mg IV over 30 min Q3W until disease progression, unacceptable toxicity, or up to 24 months (35 cycles) in subjects without disease progression. Core biopsy 3 (+/- 2) days after the first pembrolizumab dose.
PD-L1 by Ventana SP142. RECIST v1.1.
Primary endpoint: ORR (CR, PR). Secondary endpoints: CBR (CR, PR, SD); OS; PFS; safety. Exploratory endpoint: immune response to treatment.
Guan J, et al. Int J Radiat Oncol Biol Phys. 2024 Apr 1;118(5):1531-1540. Houston Methodist Neal Cancer Center.
———
[Slide 2]
Results (Best response - no. (%))
By ICI treatment: Naive (n=19) / Refractory (n=8). By PD-L1 level: 0% (n=15) / 1-49% (n=10) / >50% (n=2). All patients (n=27).
- Confirmed CR: 2 (10.5) / 0 (0) | 0 (0) / 2 (20) / 0 (0) | 2 (7.4)
- Confirmed PR: 5 (26.3) / 2 (25.0) | 4 (26.7) / 2 (20) / 1 (50.0) | 7 (25.9)
- Stable disease: 6 (31.6) / 4 (50.0) | 5 (33.3) / 5 (50) / 0 (0) | 10 (37.0)
- Progressive disease: 6 (31.6) / 2 (25.0) | 6 (40.0) / 1 (10) / 1 (50.0) | 8 (29.6)
- ORR - no. (%): 7 (36.8) / 2 (25.0) | 4 (26.7) / 4 (40.0) / 1 (50.0) | 9 (33.3)
- Clinical benefit - no. (%): 13 (68.4) / 6 (75) | 9 (60.0) / 9 (90.0) / 1 (50.0) | 19 (70.4)
Abbreviations: CR = complete response, PR = partial response, SD = stable disease, PD = progressive disease, ORR = overall response rate, CBR = clinical benefit rate, ICI = immune checkpoint inhibitor.
KM curve: Log Rank P-value <0.001 (responders vs non-responders). mOS: 18.1 months vs. NR.
Guan J, et al. Int J Radiat Oncol Biol Phys. 2024 Apr 1;118(5):1531-1540.
———
[Slide 3]
AEs (Events / Any grade / Grade 3 or 4)
- Treatment-related AEs: 17 (60.7) / 6 (21.4)
- AEs leading to discontinuation: 4 (14.3) / 4 (14.3)
- Treatment-related death: 0 (0) / 0 (0)
Gastrointestinal: Mucositis 0(0)/0(0); Nausea 2(7.1)/0(0); Vomiting 1(3.6)/0(0); Colitis 2(7.1)/1(3.6); Diarrhea 3(10.7)/1(3.6); Constipation 0(0)/0(0); ALT elevation 0(0)/0(0); AST elevation 0(0)/0(0); ALP elevation 2(0)/2(0); Abdominal pain 2(7.1)/0(0); Decreased appetite 2(7.1)/1(3.6).
Hematologic toxicity: Anemia 1(3.6)/1(3.6); Leukocytosis 0(0)/0(0).
Pulmonary toxicity: Pneumonitis 3(10.7)/2(7.1); SOB 4(14.3)/0(0); DOE 2(7.1)/0(0); Cough 4(14.3)/0(0).
Endocrine: Hypothyroidism 2(7.1)/0(0); Hyperthyroidism 0(0)/0(0); Adrenal insufficiency 1(3.6)/0(0); T1DM 1(3.6)/1(3.6).
Infection: Pneumonia 1(3.6)/1(3.6); Shingles 1(3.6)/1(3.6); Sepsis 1(3.6)/2(7.1).
Rash 3(10.7)/1(3.6); Itching 1(3.6)/0(0); Fever 1(3.6)/0(0); Fatigue 7(25.0)/0(0); Arthralgia 1(3.6)/0(0); Others 14(50.0)/2(7.1).
Guan J, et al. Int J Radiat Oncol Biol Phys. 2024 Apr 1;118(5):1531-1540.
———
[Slide 4]
Immune profile analysis (2B) - box plots of Percentage over CD45 (%) by response group (R = responder, SD = stable disease, N/R = non-responder), colored by Day1/Day17/Day30:
- CD8: p=0.021; p=0.004; p=0.093
- Effector CD8
- Naive CD8: p=0.836
- PD1+ CD8: p=0.007; p=0.039
- Tem CD8: p=0.021
- PD1+ classical monocyte: p=0.018
Guan J, et al. Int J Radiat Oncol Biol Phys. 2024 Apr 1;118(5):1531-1540.
Robotic bronchoscopy for lung cancer: Dr. Matthew Bott (@MSKCancerCenter) presented robotic bronchoscopy for diagnosis of pulmonary lesions, providing molecular and staging information, with a safety profile and emerging applications in nodule localization. #DAVALung
[Slide 1]
Results
Overall Diagnostic Yield = 81.7%
Of 29 non-diagnostic lesions: 14 proved malignant (48%); 2 proved non-malignant (7%); 8 remained stable or regressed (27%); 2 increased in size (7%); 3 had insufficient follow-up (10%)
[Flow: Pulmonary Parenchymal Lesion Targeted for Sampling N=159; Specimen Acquired? No -> Non-Diagnostic N=2; Yes N=157; Pathologic Classification: Malignant N=90, Non-Malignant N=42, Insufficient N=25; Clinical-Radiographic-Pathologic Correlation: Diagnostic N=90; Diagnostic N=40; Non-Diagnostic N=2; Non-Diagnostic N=25]
Kalcheim-Dekel O, et al. Shape-Sensing Robotic-Assisted Bronchoscopy in the Diagnosis of Pulmonary Parenchymal Lesions. Chest. 2022; 161(2):572-582.
Safety
Overall: 44 complications (any grade) in 1455 patients (3.0%)
- Grade 3 or higher = 2 complication (0.14%)
- Grade 5 = 1 mortality (0.06%) from CVA following GA
- Grade 3 = 1 small volume hemoptysis requiring repeat bronchoscopy 10 days later
- 3 pneumothorax (0.2%), 2 requiring tube thoracostomy (Percutaneous = 17-26%)
- 5 cases of hemoptysis (0.3%), 1 repeat bronchoscopy, 4 monitored without intervention (percutaneous = 4-27%)
- 8 cases of post-op hypoxia (0.5%), all monitored without intervention
Courtesy of Or Kalcheim-Dekel. Wu C et al. Complications of CT-Guided Percutaneous Needle Biopsy of the Chest: Prevention and Management. Am J Roentgenology. 2011; 196: W678-W682.
———
[Slide 2]
Molecular Diagnostics
Retrospective review of 128 diagnostic NSCLC samples obtained via robotic bronchoscopy. Assessed suitability for molecular testing in commonly used assays
[Flow: 128 malignant robotic-assisted bronchoscopy samples; Pathologist review for molecular adequacy; Adequate (N=108) / Inadequate (N=20); PCR-based assay (N=52): Successful N=49, Failed N=3; NGS assay (N=26): Successful N=25, Failed N=1; Molecular not obtained (N=30)]
- Mean lesion size = 2.19cm (81% primary lung cancer)
- Adequate for molecular testing in 84%
- Median tumor cellularity = 60% (IQR 25-80%)
- NGS success in 25/26 samples (96%)
- PCR testing success in 49/52 (94%)
- PD-L1 IHC in 61/67 (91%)
Connolly J., et al. JTCVS. 2023; 166(1)231-240.
Conclusions
- Robotic bronchoscopy is a safe and effective technique for the diagnosis of pulmonary lesions
- Can provide staging and molecular information to guide peri-operative therapy - May enhance efficiency of care
- Additional applications such as nodule localization may be particularly useful for early stage lesions
- Therapeutic approaches are also in development
———
[Slide 3]
Navi bronch vs. Percutaneous Biopsy
The New England Journal of Medicine - ORIGINAL ARTICLE
Navigational Bronchoscopy or Transthoracic Needle Biopsy for Lung Nodules
R.J. Lentz, K. Frederick-Dyer, V.B. Planz, T. Koyama, M.C. Aboudara, S.K. Avasarala, J.D. Casey, G.Z. Cheng, P.-F. D'Haese, J.D. Duke, E.L. Grogan, T.C. Hoopman, J. Johnson, J.M. Katsis, J.S. Kurman, S.-W. Low, K. Mahmood, O.B. Rickman, L. Roller, C. Salmon, S. Shojaee, B. Swanner, M.M. Wahidi, C. Walston, G.A. Silvestri, L. Yarmus, N.M. Rahman and F. Maldonado for the Interventional Pulmonary Outcomes Group
- Multicenter randomized trial using Illumisite platform with tomosynthesis for biopsy of nodules measuring 10 to 30mm
- 119 pts vs. 110pts
- Yield with navi bronch = 79%
- Yield percutaneous = 73.6%
- P=0.003 for non-inferiority
Pneumothorax rate = 3% for navi bronch vs. 28% percutaneous
———
[Slide 4]
Therapeutic Applications
- Transbronchial ablation
- Injectable therapeutics: Pharmacologic; Gene therapy; Immune modulation
Novel Image-Guided Flexible-Probe Transbronchial Microwave Ablation for Stage 1 Lung Cancer
Michael A. Pritchett, Janani S. Reisenauer, Ryan Kern, David S. Wilson, Erin E. Meyers, Philippe O. Szapary, Paul F. Laeseke. Respirology. 2023; 102:182-193.
[NCI screenshot] A Study of JNJ-90301900 in Combination With Chemoradiation Followed by Consolidation Immunotherapy for Non-Small Cell Lung Cancer (NSCLC). Status Active.
Leveraging HLA-A*02 loss of heterozygosity, logic-gated CAR T-cell therapies are being evaluated to enhance tumor selectivity in solid tumors. Antonious Hazim, MD (@AHazimMD@MayoClinic) reviews the EVEREST-2 and DENALI-1 studies and early clinical activity. #DAVALung
BASECAMP-1DENALI-1EVEREST-2
[Slide 1]
LOGIC-GATED CAR T THERAPY WITH THE GOAL TO REDUCE TOXICITY: MSLN AND HLA-A*02
- The blocker receptor recognizes an HLA-A*02 allele that is present in normal cells and lost in tumor cells; the presence of the HLA-A*02 antigen in normal cells acts as an inhibitor of the CAR T cell
- The blocker therefore increases the therapeutic window by diminishing on-target, off-tumor toxicity
[Diagram: Tmod Cell; Activator + Blocker design achieves selectivity; HLA-A*02 Blocker; MSLN Activator; Block -> HLA-A*02, Normal cells are protected; Kill -> MSLN, Tumor cells lack blocker antigen, Tmod cells activate and kill tumor]
Punekar et al., WCLC 2025
———
[Slide 2]
Study Design: BASECAMP-1 to EVEREST-2
BASECAMP-1: Prescreening Trial - Initial screening; HLA-A*02 LOH confirmed; HLA-A*02 heterozygosity confirmed; Cryopreservation of leukapheresis product; Leukapheresis -> A2B694 manufacturing
EVEREST-2: Phase 1/2 Trial of MSLN Tmod CAR Ts (A2B694)
Patients: Metastatic NSCLC, PANC, CRC, OVCA, MESO, or other cancers with MSLN expression
Timeline: Eligibility screening; Lymphodepleting chemotherapy D-5 D-4 D-3; A2B694 infusion D0; Follow-up
———
[Slide 3]
Study Schema: BASECAMP-1 to DENALI-1
BASECAMP-1: Prescreening Trial - Initial screening; HLA-A*02 LOH confirmed; HLA-A*02 heterozygosity confirmed
DENALI-1: Phase 1/2 Trial of EGFR Tmod CAR Ts (A2B395)
Timeline: Eligibility screening; Lymphodepleting chemotherapy D-6 D-5 D-4 D-3; A2B395 infusion D0; Follow-up
Patients: Histologically confirmed recurrent unresectable, locally advanced, or metastatic CRC, NSCLC, HNSCC, TNBC, RCC, or other solid tumors with EGFR expression. Measurable disease is required with lesions of >=1.0 cm by CT; Received >=1 line of prior therapy; ECOG PS 0-1
———
[Slide 4]
CR in Patient with KRAS G12V/STK11 Mutated NSCLC
Timeline (Days before and after infusion, -200 to 275): PET-CT positive; ctDNA positive; Progression with new osseous lesions; End of first-line chemotherapy; Apheresis; Enrollment; Lymphodepletion; Infusion; Complete CR; Confirmed CR by central review per RECIST 1.1; Negative ctDNA, resolution of PET positive disease; CNS relapse; continued non-CNS CR; Gamma knife; Continued non-CNS CR
First patient with NSCLC to have a complete response after CAR T
Rethinking Multifocal GGOs: Dr. James Huang (@MSKCancerCenter) presented TSOG 102, an AATS active surveillance registry for multiple ground-glass opacities, tracking each lesion with serial CT and reserving intervention for progression to limit overtreatment. #DAVALung
[Slide 1]
Randomized Trial of Active Surveillance in Prostate Cancer
Prostate Cancer-Specific Survival KM curve: Prostatectomy vs Radiotherapy vs Active monitoring. No. at Risk 1643, 1589, 1490, 654, 282.
15 yr Survival: Surgery 97.2%; Surveillance 96.6%; RT 97.7%.
Hamdy FC et al. N Engl J Med 2023;388:1547-1558.
Take home messages - Active Monitoring in Prostate Ca:
- It's ok to wait. Electing for surgery or radiation right away did not lead to any improvement in survival vs. watchful waiting
- You won't miss the window of opportunity
- Consider tradeoffs between harms and benefits
- You may never actually need treatment
Memorial Sloan Kettering Cancer Center
———
[Slide 2]
Registry Trial for Multiple GGO
- Patients with 2 or more GGO enrolled in active surveillance registry
- Each lesion enrolled and tracked in registry
- Surveillance q6-12 m CT scan
Registry Trial of GGO - Schema
- Surveillance on protocol for 5 years
- Intervention (biopsy or surgery) reserved only for progression of a lesion, defined as either:
- Growth of greatest diameter by > 50% over baseline
- Increase in solid component with consolidation-tumor ratio threshold of > 50%
- At the discretion of the treating clinician
Registry Trial of GGO - Concept and Hypothesis
- Registry of GGO on active surveillance: Mirrors common practice; Prospective data about the natural history of these lesions; Standardized protocol for surveillance and intervention
- Hypothesis: Active surveillance for GGO is feasible and safe, and potentially spares patients from overtreatment
Memorial Sloan Kettering Cancer Center
———
[Slide 3]
GGO Registry: Patient Examples Growth Kinetics
Thoracic Surgery Oncology Group (AATS) - A joint venture between AATS and Memorial Sloan Kettering Cancer Center
"Patient 001": Size of GGO in greatest dimension (cm) vs Follow-up timepoint (0-5); lesions stable ~0.4-0.8 cm.
"Patient 003": Size of GGO in greatest dimension (cm) vs Follow-up timepoint (0-5); multiple lesions ~0.6-1.4 cm.
———
[Slide 4]
Ongoing Trials of Active Surveillance
TABLE 2. Ongoing prospective trials for active surveillance in patients with ground-glass opacities.
Trial | Region | Planned accrual | Primary end point | No. of lesions | Lesion eligibility | Surveillance interval | Indication for intervention | Accrual initiation | Anticipated completion
TSOG 102 | North America | 330 | 5-y LCSS | >=2 | 0.6-3.0 cm and CTR <0.5 | 6-12 mo | Growth >50% or CTR >0.5 (recommended) | 1/2019 | 8/2028
JCOG 1906 | Japan | 720 | 10-y OS | 1-3 | <=2 cm and CTR <=0.25 | 6-12 mo | Lesion >2 cm or CTR >0.25 | 6/2020 | 6/2036
ECTOP-1021 | China | 290 | 5-y OS | >=3 | 0.6-2.0 cm and CTR <0.25 | 12 mo | Growth >1.5 mm or appearance of solid component | 11/2023 | 11/2030
TSOG, Thoracic Surgical Oncology Group; LCSS, lung cancer-specific survival; CTR, consolidation to tumor ratio; JCOG, Japan Clinical Oncology Group; OS, overall survival; ECTOP, Eastern Cooperative Thoracic Oncology Project.
Huang J, JTCVS 2025
Questions and Food for Thought
- The question is not identifying whether these GGOs are cancer. The question is which of these GGOs will kill you if you don't intervene during your lifetime.
- Not every GGO will kill you: At what point does a GGO become deadly? At what point does a GGO become incurable? What should be the trigger point for intervention?
Memorial Sloan Kettering Cancer Center
New data worth a look: in STK11/KEAP1-mutant NSCLC, TRITON IA found T+D+CT beat P+CT on ORR (39.0% vs 34.9%) and DoR (NR vs 6.4 mo). Biagio Ricciuti, MD, PhD (@BRicciutiMD, @DanaFarber) breaks down the case for CTLA4-based strategies. #DAVALung
[Slide 1]
STK11 drives primary resistance to PD-(L)1 blockade
[B] CM-057: % with PR/CR as BOR by group. P = 0.047, Fisher exact test. Group KL / KP / K-only. ORR: KL 0% (0/6), KP 57.1% (4/7), K-only 18.2% (2/11).
[A] Response rate (%) in KRAS-MUT: STK11-WT 32.4% (129/398) vs STK11-MUT 11.6% (16/138). p < 0.0001.
Skoulidis et al. Cancer Discovery 2018, Ricciuti B et al. J Thorac Oncol 2022
———
[Slide 2]
CTLA4 blockade reduces KEAP1/STK11-related resistance to PD-(L)1 inhibitors in syngeneic models in vivo
f. Syngeneic mouse tumor models (Kras-mut Keap1-mut; Kras-mut Stk11-mut Keap1-mut; Kras-mut Stk11-mut): Tumour volume over time after randomization and probability of TV<1200 mm3 survival curves. Treatment arms: IgG control, Anti-PD-1, Anti-CTLA4, Anti-PD-1 + anti-CTLA4.
Skoulidis F et al. Nature 2024
———
[Slide 3]
TRITON: Phase 2b randomized, open-label, US multicenter study
An interim analysis of ORR, DoR, and safety was planned when the first patient randomized had a minimum follow-up of 15 months; at this time, 84 patients had the opportunity for a minimum follow-up of 3 months.
Study population N=100: NSQ metastatic NSCLC with STK11m +/- KEAP1m +/- KRASm; No prior systemic treatment for metastatic disease; No EGFRm or ALK alterations; ECOG PS 0 or 1; Tumor biopsy (if available) and baseline plasma sample (for ctDNA). R 1:1.
Arm 1: Tremelimumab + durvalumab + platinum-pemetrexed -> Tremelimumab (week 16 and month 24) + durvalumab + pemetrexed. Induction: 4 cycles, Maintenance treatment.
Arm 2: Pembrolizumab + platinum-pemetrexed -> Pembrolizumab + pemetrexed.
Stratification: STK11m vs KEAP1m vs KRASm | PD-L1 TC >=1% vs <1%.
Primary endpoint: PFS. Key secondary endpoints: OS (inc. rates at 12 & 24 mos), TFST, ORR, DoR (inc. rates at 3, 6, 9, & 12 mos), Safety/tolerability. Exploratory analyses: Outcomes by individual mutations.
Skoulidis et al ASCO 2026
———
[Slide 4]
TRITON IA: ORR and DoR were numerically greater with first-line T+D+CT vs P+CT in STK11 and/or KEAP1 and/or KRAS-mutated NSQ mNSCLC
ORR (95% CI): Tremelimumab + durvalumab + CT (n=41) vs Pembrolizumab + CT (n=43). Confirmed response: 39.0 vs 34.9. Unconfirmed response: 48.8 vs 41.9.
DoR KM: Proportion of patients still in response over time from first confirmed objective response. T+D+CT reaches 100%, P+CT 58.3%. Responders, n: T+D+CT 16, P+CT 15. Median DoR (95% CI), months: T+D+CT NR (6.3-NR), P+CT 6.4 (4.2-NR). No. at risk: T+D+CT 16, 14, 7, 2, 0, 0; P+CT 15, 12, 3, 2, 0, 0 (0-15 months).
Skoulidis et al ASCO 2026
After anti-PD-(L)1 failure, can ATR inhibition help? John Heymach (@UTMDAnderson) highlights HUDSON, where durvalumab+ceralasertib delivered mPFS 5.8 mo, with signals in KRAS/STK11/KEAP1 and ATM-altered NSCLC. Non-biomarker selected RP3 LATIFY study was negative.#DAVALung
HUDSON
[Slide 1]
ATR plays a key role in sensing DNA damage, halting cell cycle in response to DD or RS, and maintaining genomic integrity
Cell cycle checkpoint: Chk1, CDC25, Wee1, CDK, FOXM1. Mitosis: Chk1, Aurora A/B, CENP-F, ETAA1. Origin firing: Chk1, MCM2-7, CDC45, Treslin, DDK, MLL. RS tolerance: SMARCAL1, RNF4, PLK, PCAF, RPA, PALB2, XRCC3, REV1, PolH, PrimPol.
ATR inhibition: Early S phase -> Replication catastrophe; Late S to G2/M phase -> Mitotic catastrophe. High-dose ATRi (cell death) vs Low-dose ATRi. Normal cells; Cancer cells with low RS (Oncogenes+DDR defects); Cancer cells with high RS (Oncogenes+DDR defects+RS tolerance); Cancer cells with therapy (Oncogenes+DDR defects+RS tolerance+Drugs).
Tumor cells with replication stress, or ATM alterations, are potential targets for ATR inhibition.
Yano and Shiotani, Cancer Sci 2023
———
[Slide 2]
The (non-biomarker selected) RP3 LATIFY trial of durva/cerala vs docetaxel in advanced NSCLC patients without actionable mutations
RP3 LATIFY study: Post chemo/IO in 2L+ NSCLC without actionable mutations. R -> docetaxel vs Ceralasertib plus durvalumab.
Table: LBA1 - C+D (n=299) vs Docetaxel (n=295):
OS: Median duration of follow-up mo (range) 19.9 (0-32) vs 19.5 (0-31); Median OS, mo (95% CI) 11.1 (10.0-12.7) vs 10.0 (8.5-11.7); 12-mo OS rate, % (95% CI) 46.3 (40.4-52.1) vs 43.6 (37.6-49.4); HR (95% CI) 0.90 (0.75-1.09); 2-sided p-value 0.287.
PFS: Median PFS, mo (95% CI) 4.1 (3.8-4.4) vs 4.1 (3.5-4.3); 6-mo rate, % (95% CI) 35.3 (29.8-40.9) vs 33.5 (27.8-39.4); HR (95% CI) 0.87 (0.73-1.04); Nominal 2-sided p-value 0.133; ORR, % (95% CI) 7.7 (4.9-11.3) vs 17.3 (13.2-22.1).
Median duration of exposure, mo (range): C (n=297) 4.5 (0.4-31.9); D (n=297) 3.8 (0-31.7); Docetaxel (n=274) 3.0 (0.3-27.6).
Conclusions: C+D did not demonstrate a statistically significant improvement in OS vs docetaxel. C+D had manageable toxicity and AEs were consistent with the known safety profiles of each agent.
Besse et al., ESMO Open Volume 11, Supplement 3, 106957, April 2026
———
[Slide 3]
An Open-Label, Multi-Drug, Biomarker-Directed, Multi-Centre Phase II Umbrella Study in Patients with Non-Small Cell Lung Cancer, who Progressed on an anti-PD-1/PD-L1 Containing Therapy (HUDSON).
Study drug: Durvalumab; Danvatirsen; Ceralasertib; Vistusertib; Olaparib; Oleclumab; Trastuzumab deruxtecan; Cediranib.
[Study schema: Group A biomarker matched cohorts; Group B biomarker non-matched cohorts (Primary resistance vs Acquired resistance); modules of durvalumab + agent. Immunotherapy resistance; Primary resistance n=; Acquired resistance n=]
Besse et al., Nature Med 2024; https://www.astrazenecaclinicaltrials.com/study/D6185C00001/
———
[Slide 4]
PFS and OS with durvalumab-ceralasertib vs other combination arms in chemo- and IO-refractory patients in HUDSON
mPFS: Durvalumab-ceralasertib, 5.8 mo; Other, 2.7 mo.
mOS: Durvalumab-ceralasertib, 17.4 mo; Other, 9.4 mo.
[a] KM curve PFS (Ceralasertib+durvalumab n=; Other regimens n=); [b] KM curve OS.
Besse et al., Nature Med 2024
Can a PD-1/VEGF bispecific move the needle in NSCLC? @LeXiuning, @UTMDAnderson says yes — HARMONi-A showed ivonescimab+chemo improved PFS (7.1 vs 4.8 mo, HR 0.46) and OS (16.8 vs 14.1 mo, HR 0.74) over placebo+chemo. Ivonescimab exhibited similar irAEs to that of Pembro #DAVALung
Dr. Arjan Gower (@UCLA) presents Phase 1 data on VT3989: 26% ORR, 85% disease control in heavily pretreated patients, with manageable safety. Antitumor activity enriched in low/absent Merlin expression. TEAD inhibition shows promise in mesothelioma. #DAVALung
[Slide 1]
TEAD targeting drugs in clinical trials
Drug | Sponsor | Mechanism of Action | TEAD selectivity | Clinical trial
VT3989 | Vivace | Non-covalent autopalmitoylation inhibitor | TEAD 1,(2),3,(4) | NCT04665206 Phase I/II started 3/2021
IAG933 | Novartis | YAP/TAZ-TEAD PPI inhibitor | Pan-TEAD | NCT04857372 Phase I started 10/2021
BPI-460372 | Betta | Covalent autopalmitoylation inhibitor | TEAD 1,3,4 | NCT05789602 Phase I started 4/2023
BGC515 | BridGene | Covalent autopalmitoylation inhibitor | Pan-TEAD | NCT06452160 Phase I started 6/2024
SW-682 | SpringWorks | Autopalmitoylation inhibitor | Pan-TEAD | NCT062513010 Phase I started 7/2024
ISM6331 | Insilico | Non-covalent autopalmitoylation inhibitor | Pan-TEAD | NCT06566079 Phase I started 12/2024
Adapted from Harvey and Tang, Nat. Rev. Drug Discov. 2025
UCLA Health
278
———
[Slide 2]
VT3989 Background
- Oral, selective small molecule inhibitor of TEAD autopalmitoylation to disrupt YAP transcriptional activity
- Binds all 4 TEAD paralogs (TEAD 1-4), though it more strongly blocks TEAD1 and TEAD3 in preclinical studies
- VT3989 cell proliferation assays in meso cell lines
- Merlin-positive cells retain expression of NF2-encoded tumor suppressor merlin
- In Merlin-positive cell lines, VT3989 was ~100-1000X less efficacious
Table (VT3989): Cell Line | GI50 (nM) | Max inh % | NF2 Mutation | Merlin Level. Rows include NCI-H226 9/101, NCI-H2373 8/92, SDM103T2 26/82, NCI-H2052 16/93, ACE-MESO-1 15/84, SPC212 60/72, JU77 74/82, Mero-48a 38/109, ZL34 20/95, ZL55 48/87, Mero-14 60/94, Mero-82 118/75, ONE58 186/67, Mero-83 118/75, Mero-95 197/67, Mero-41 260/71, ZL5 178/80, SPC111 1511/64, NO36 >3000/33, Mero-84 >3000/13, ACE-MESO-4 879/67, Mero-25 2494/54, NCI-H28 >3000/..., NCI-H2452 >3000/..., HMMME >3000/...
Yap et al, Nature Medicine 2025
279
———
[Slide 3]
First-in-human Phase 1 Schema of VT3989
Enrolled (N = 172); Dose-escalation phase (N = 85); Dose-expansion phase (N = 87 [75]).
Dose-escalation: Continuous dosing schedule Cohorts 1-5 (N = 27 [13]) - 200 mg, 4 pts - 0 DLT; 150 mg, 6 pts - 0 DLT; 100 mg, 6 pts - 0 DLT; 50 mg, 6 pts - 0 DLT; 25 mg, 5 pts - 0 DLT. 3+3 design.
Intermittent dosing schedule Cohorts 6-14 (N = 58 [47]) - 200 mg daily 2W/1W, n=6; 200 mg daily 1W/2W, n=6; 200 mg daily 2W/2W, n=5; 100 mg daily 2W/2W, n=6; 150 mg daily 1W/3W, n=6; 100 mg daily 2W, then 100 mg QW, n=7; 50 mg daily 2W, then 50 mg QW, n=6; 50 mg daily 2W/2W, n=10; 50 mg BIW, n=6.
Dose-expansion phase: EC-1: 100 mg daily 2W/2W (NPM/PM), N=27; EC-2: 50 mg daily 15 days followed by 100 mg weekly (NPM/PM), N=27; RP2D EC-3: 100 mg daily 2W/2W (NPM), N=17; EC-4: 100 mg daily 2W/2W (other solid tumors), N=12; EC-5: 100 mg daily 2W/2W (PM), N=4.
- 100 mg qD, 2 weeks on, 2 weeks off as RP2D. Exposure-response analysis revealed higher dosing did not enhance efficacy, but correlated with increased toxicity (proteinuria).
- After a protocol amendment, 22 additional pts with advanced mesothelioma received VT3989 treatment under a higher UACR threshold.
- Primary efficacy analysis included pts (N=47) with advanced mesothelioma treated at the clinically optimized regimens: 50 mg QD 2 W/2 W and 100 mg QD 2 W/2 W with a higher prespecified UACR threshold.
Yap et al, Nature Medicine 2025
280
———
[Slide 4]
VT3989 activity in mesothelioma at RP2D
Waterfall plot (axis 100 to -100): PR (blue), SD (green), PD (red).
Table: Investigator-assessed response | Clinically optimized dose regardless of UACR threshold (N=47) | Clinically optimized dose and optimal UACR threshold (N=22)
Partial response; n (%): 12 (26%) | 7 (32%)
Stable disease; n (%): 28 (60%) | 12 (54%)
Disease control rate; n (%): 40 (85%) | 19 (86%)
Duration of response (median weeks): 24 | NE
PFS (median weeks): 25 | 40
100% had prior immunotherapy, and 82% had prior chemotherapy.
Yap et al, Nature Medicine 2025
281
ctDNA MRD may reshape resectable NSCLC care. @ValsamoA@HopkinsMedicine reviews 77T, where 87% of nivolumab-arm patients had baseline ctDNA and clearance may guide escalation/de-escalation. She emphasized on clinical sensitivity of ctDNA sensitivity. #DAVALung
[Slide 1]
Ultra-sensitive tumor-informed ctDNA MRD assays
Increasing number of variants interrogated: Tumor-informed whole genome sequencing bespoke ctDNA MRD. WGS (tumor), optimized cfDNA prep, library prep and capture from plasma samples; algorithmic selection of ~1,800 variants with high signal-to-noise ratio, probe optimization, panel manufacturing. Limit of detection ppm. LUAD and Non-LUAD detection rates by stage (Attobch 2017, Attobch 2022, Current study).
Reducing background sequencing error: Noise suppression by interrogation of genome-wide phased variants (in cis). Single nucleotide variant vs Phased variants; recovery of molecules by duplex sequencing (trans) or phased variants (cis). WGS from lymphoma tumors; ~7,500x enrichment vs WGS; ICGC (n=44), Qian (n=10), Morin (n=25).
Black et al., Nat Med, 2025; Kurtz et al., Nat Biotechnol, 2021
———
[Slide 2]
Bespoke panel-free tumor-informed whole-genome sequencing for minimal residual disease detection
Tumor-informed WGS: cfDNA (plasma) 10 ng input -> Library preparation -> WGS (30x) -> cfDNA SNVs; Tumor DNA (FFPE) 200 ng input -> WGS (80x); WBC DNA (buffy coat) 50 ng input -> WGS (40x) -> Tumor-specific SNVs -> Random forest machine learning model with informative features -> Noise subtraction; Noncancerous cfDNA reference (80 plasma samples from healthy donors) -> High-confidence tumor-specific cfDNA variants; ctDNA status (Detectable/Undetectable); cfDNA tumor fraction (%). LoD of 0.005% ctDNA content.
Tumor-naive targeted NGS: cfDNA (plasma) 10-25 ng input; WBC DNA (buffy coat) 10-25 ng input -> Library preparation & hybrid capture -> Ultra-deep targeted NGS (~20,000x) -> cfDNA variants / WBC variants -> Filtering of clonal hematopoiesis and germline variants -> Putative cfDNA variant origin; Variant allele frequency (%). LoD of 0.1% VAF.
Lee et al., presented at the AACR 2026 Annual Meeting (abstract # 1129)
———
[Slide 3]
ctDNA MRD in the 77T trial of perioperative nivolumab
NIVO (n=40) - ctDNA clearance before surgery, pCR status, MRD-positive before or during the adjuvant period:
ctDNA clearance: Yes 30 (75%), No 10 (25%)
pCR status: pCR 21 (70%), No pCR 10 (100% of the No-clearance group); No pCR 9 (30%)
MRD-positive before or during adjuvant: No 9 (90%) / Yes 1 (10%); No 20 (95%) / Yes 1 (5%); No 8 (89%) / Yes 1 (11%)
- 46 patients in the NIVO arm and 44 in the PBO arm were evaluable for ctDNA
- 40/46 (87%) in the NIVO arm had detectable ctDNA before neoadjuvant treatment
- 37/44 (84%) in the PBO arm had detectable ctDNA before neoadjuvant treatment
- Small fraction of patients with ctDNA MRD+ post-surgery
Cascone et al., presented at the AACR 2026 Annual Meeting
———
[Slide 4]
PRE0511-ctDNA biomarker clinical trial (TicTacToe)
Key Eligibility Criteria: Stage I-III, treatment-naive non-small cell lung cancer; >=18 yrs old; ECOG performance status 0-2
Endpoints: ctDNA correlation with 2-year DFS (primary)
Cohort A - Surgery First (N=103); Cohort B - Neoadjuvant First (N=202); Cohort C - Oncogene-driven (N=61)
Timepoints: Diagnosis, Cycle 3 Neoadj tx, Pre-op, Landmark MRD, Baseline Adj tx, @ 3 months, @ 6 months, @ 12 months, @ 18 months, Recurrence
Blood collection and Diagnostic tissue biopsy per cohort. Adjuvant IO therapy, Neoadjuvant IO therapy, Adjuvant TKI+/-chemotx. 40ml 4 x Streck tubes; 60ml 6 x Streck tubes. ctDNA MRD replicate 4-6w post-op; ctDNA MRD monitoring.
Clinical protocol in development by PRECOG (study chairs: Anagnostou V and Aggarwal C)
Named Trials & Studies
Trials Surfaced at DAVA Hawaii Lung 2026
Every clinical trial or study named across the presented slides (extracted via full-slide OCR). Linked badges open the full KOL Pulse trial profile.
DAVA Hawaii Lung 2026 is DAVA Oncology's summit on thoracic malignancies (Kona, Hawaii, Jul 8–11, 2026). This is a curated slide-intelligence view assembled by KOL Pulse from the public #DAVALung feed — every presented slide was OCR-transcribed, grouped by theme, with speakers linked to their X and institutional profiles and every named trial tagged. Slide images and summaries are the presenters' own as shared on X. Compiled by the KOL Pulse research team, led by Brian Shields, Founder, KOL Pulse. Last updated Jul 10, 2026.
×
Free access — track oncology’s top KOLs in your specialty: profiles, pharma influence, ad-board patterns & 2025 Open Payments analysis.Get free access